
Enhanced CT Based Texture Analysis and Machine Learning for Differentiation between Adenolymphoma and Mixed Tumors of the Parotid Gland
-
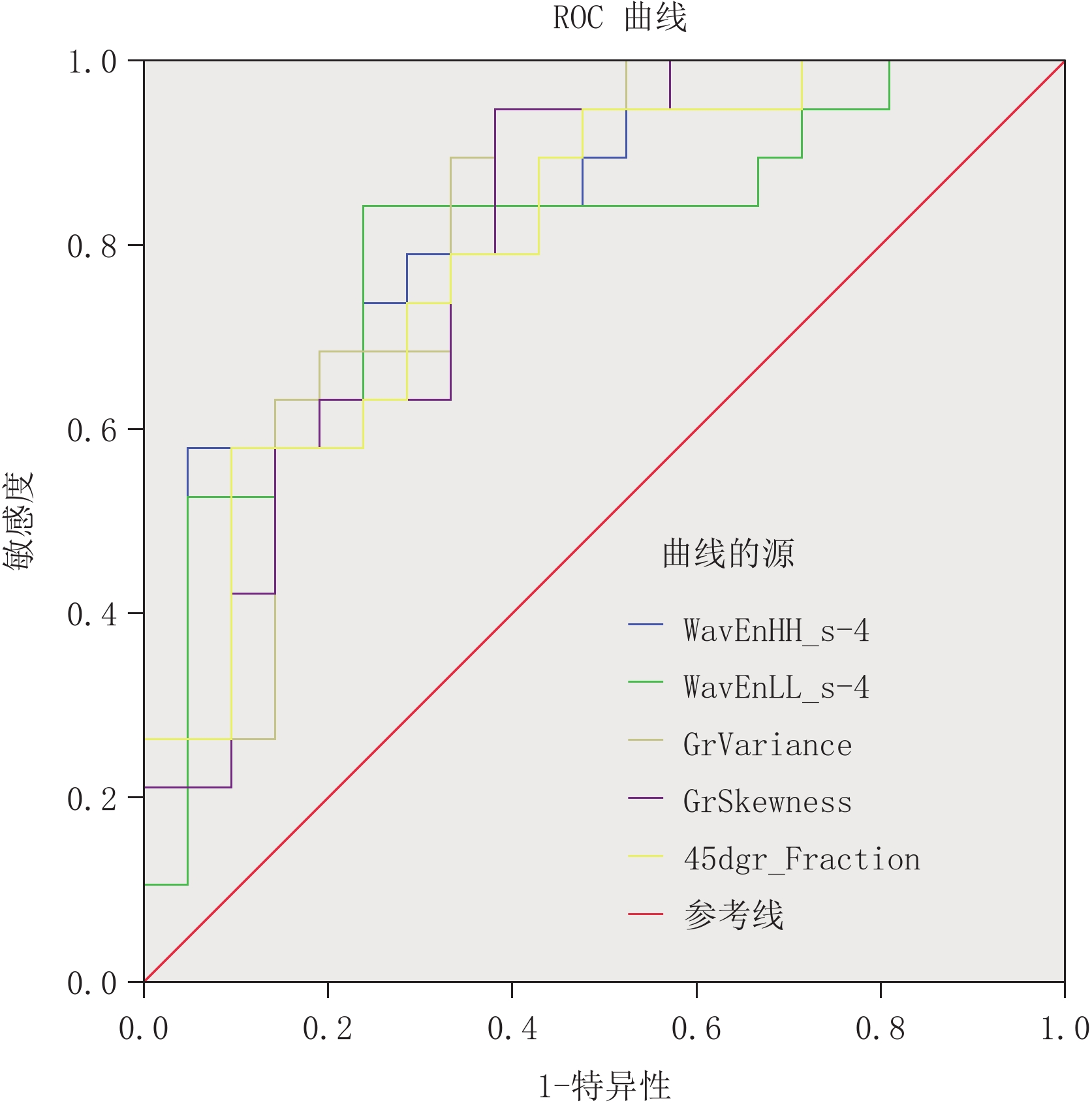
摘要: 目的:探究基于增强CT纹理分析技术联合机器学习在腮腺腺淋巴瘤与混合瘤鉴别中的应用。方法:回顾性分析40例于本院手术并有完整病理资料的腮腺腺淋巴瘤与混合瘤患者,其中腺淋巴瘤组21例,混合瘤组19例。运用Mazda软件在增强CT静脉期图像上手动勾画病灶最大层面ROI区;应用Fisher系数、POE+ACC、MI及三者联合应用(FPM)的方法,筛选出最佳纹理参数,通过ROC曲线评估其诊断效能;最后采用RDA、PCA和LDA、NDA四种机器学习算法进行分类分析,并分析不同算法的诊断效能。结果:纹理特征参数中腺淋巴瘤组的WavEnHH_s-4、GrVariance、45dgr_Fraction低于混合瘤组,WavEnLL_s-4、GrSkewness高于混合瘤组,且均在组间有统计学意义。ROC曲线显示WavEnLL_s-4的敏感性与特异性较为平衡,AUC值、敏感性、特异性分别为0.797、84.2%、76.2%,具有良好诊断效能;RDA、PCA、LDA、NDA算法的误判率范围分别为30.0%~37.5%、30.0%~37.5%、7.5%~37.5%、5.0%~12.5%,其中误判率最低的是FPM联合NDA分类分析法,为5.0%;准确率、敏感性、特异性、阳性预测值、阴性预测值分别为95.0%、95.2%、94.7%、95.2%和94.7%,分类效能最佳。结论:增强CT纹理分析提取的最佳特征参数在腮腺腺淋巴瘤与混合瘤间具有显著差异,FPM联合NDA分类分析法误判率最低,有助于鉴别腮腺腺淋巴瘤与混合瘤。Abstract: Objective: To explore the application of enhanced computed tomography (CT)-based texture analysis combined with machine learning in the differential diagnosis of adenolymphomas and mixed tumors of the parotid gland. Methods: We retrospectively analyzed 21 and 19 cases of adenolymphomas and mixed tumors of the parotid gland, respectively. Regions of interest (ROI) were chosen on axial enhanced-CT images of the tumor’s maximum cross section using the Mazda software. The optimal texture parameters were selected using Fisher’s coefficient, probability of classification error and average correlation coefficients, mutual information, and a combination of the three. Receiver operating characteristic (ROC) curve analysis was performed to evaluate the diagnostic efficacy. Finally, the texture parameters were classified and analyzed using the following four machine-learning methods: raw data analysis, principal component analysis, linear discriminant analysis, and nonlinear discriminant analysis (NDA). The diagnostic efficiencies of these classification algorithms were analyzed. Results: WavEnHH_s-4, GrVariance, 45dgr_Fraction, WavEnLL_s-4, and GrSkewness were the statistically significant texture feature parameters for differentiating between parotid adenolymphomas and mixed tumors.. ROC curve analysis revealed that WavEnLL_s-4 had a balanced sensitivity and specificity, and the area under the curve, sensitivity, and specificity were 0.797, 84.2%, and 62.5%, respectively. The misclassification rate of NDA (5.0%–12.5%) was lower than that of the other algorithms. The NDA of FPM had the lowest misclassification rate (5.0%); its accuracy, sensitivity, specificity, positive predictive value, and negative predictive value were 95.0%, 95.2%, 94.7%, 95.2, and 94.7, respectively. Conclusion: The optimum enhanced CT-based texture features differed significantly between parotid adenolymphomas and mixed tumors. A combination of FPM and NDA had the lowest misclassification rate; it can contribute toward the identification of parotid adenolymphomas and mixed tumors.
-
Keywords:
- enhanced CT /
- machine learning /
- texture analysis /
- parotid tumor
-
2002年世界卫生组织软组织肿瘤分类将腺泡状软组织肉瘤(alveolar soft part sarcoma,ASPS)归入“分化不明的肿瘤”类别[1]。ASPS是一种罕见的恶性软组织肿瘤,主要发生于青少年和年轻人,可以出现在身体的任何部位,但最常见于四肢的深层软组织。ASPS通常表现为一种相对惰性但致命的肉瘤,特点是晚期转移和延长的临床病程[2]。然而,当根治性切除时,局部复发很少见,长期生存是可能的[3]。因此,术前区分ASPS与其他软组织肿瘤对于优化患者管理和治疗计划以改善预后很重要,诊断成像在病变识别及在初步病变表征中起着至关重要的作用。
我国相关病例报道不多,目前临床对ASPS认知较少,为提高对ASPS认识,现将我院收治1例ASPS患者分析报道,主要对其CT及MRI特点进行归纳和总结,并复习相关文献,帮助临床医生将此病与其他常见的软组织肿瘤进行鉴别诊断。
1. 病例资料
1.1 临床表现
患者男性,37岁,以“5年前发现右腋窝肿物,诊断为血管瘤,未进行治疗,近期出现间断性头晕伴失写、视物变形”为主诉而入院。右侧腋窝触及约10 cm×5 cm大小肿块,肿物表面不规则,坚韧,活动度差,有压痛,右侧肱二头肌疼痛,肢端血运可,尺桡动脉可扪及;患者出现失写,视物变形,实验室检查阴性。
1.2 影像学表现
右侧上肢CTA提示右侧腋下肌肉深部不规则软组织肿块影,部分边界清晰,部分边界不清,平扫呈均匀等密度,增强后明显不均匀强化,肿瘤内和肿瘤周围可见多发迂曲增宽的血管影(图1)。
![]() 图 1 右肩关节CT图像注:CT平扫(a)示右侧腋窝浅分叶肿块;CT增强扫描(b)及冠状面重建(c)、(d)显示肿瘤明显不均匀强化,肿瘤内和肿瘤上下极可见多发粗大血管影,(c)中白色细箭头显示肿瘤内部粗大血管,(d)中白色粗箭头显示肿瘤上下极粗大血管。肿瘤部分边界不清。Figure 1. Computed tomography of the shoulder joint
图 1 右肩关节CT图像注:CT平扫(a)示右侧腋窝浅分叶肿块;CT增强扫描(b)及冠状面重建(c)、(d)显示肿瘤明显不均匀强化,肿瘤内和肿瘤上下极可见多发粗大血管影,(c)中白色细箭头显示肿瘤内部粗大血管,(d)中白色粗箭头显示肿瘤上下极粗大血管。肿瘤部分边界不清。Figure 1. Computed tomography of the shoulder joint右肩部MRI显示右侧腋下肌肉深部不规则软组织肿块影,T1WI呈均匀等、稍高信号,T2WI呈不均匀稍高信号,肿瘤内和肿瘤周围可见多发迂曲增宽血管流空信号影,增强后明显不均匀强化,可见多发增粗流空血管影,肿瘤部分边界不清(图2)。头颅MRI显示左侧顶枕叶巨大占位,周围大片水肿,侧脑室受压推移,中线结构明显右偏,增强扫描病灶明显不均匀强化,周围见增粗迂曲血管影(图3)。胸部X线片显示两肺多发结节(图4)。
![]() 图 2 右肩关节MRI图像注:(a)TIWI平扫示右侧腋窝等、稍高信号肿块,伴多发血管流空信号(白色箭头);(b)T2WI示肿块呈高信号伴多发血管流空信号(白色箭头);(c)TIWI增强后肿瘤明显强化,亦可见血管流空信号(白色箭头)。Figure 2. Magnetic resonance imaging scan of the shoulder joint
图 2 右肩关节MRI图像注:(a)TIWI平扫示右侧腋窝等、稍高信号肿块,伴多发血管流空信号(白色箭头);(b)T2WI示肿块呈高信号伴多发血管流空信号(白色箭头);(c)TIWI增强后肿瘤明显强化,亦可见血管流空信号(白色箭头)。Figure 2. Magnetic resonance imaging scan of the shoulder joint1.3 治疗
为缓解临床症状行颅内肿瘤切除术,病理提示“转移性腺泡状软组织肉瘤”。随后,行右侧腋下肿瘤切除,病理提示“腺泡状软组织肉瘤”,考虑右侧腋下为原发灶(图5)。
2. 讨论
2.1 病因及发病机制
ASPS是一种罕见实体瘤,它最初由Christopherson等[4]于1952年描述和命名,是由t(X;17)(p11;q25)染色体易位引起的,从而导致产生融合基因ASPSLTFE 3。
2.2 临床特点
ASPS在所有软组织肉瘤中占比不足1%[5-6],主要发生于青少年和年轻人,以女性为主。原发性肿瘤最常见的部位是四肢,主要是大腿和臀部(58%~60%)、躯干(16%~28%)和头颈部(12%)。也可起源于其他少见部位,比如前列腺、子宫、膀胱和乳房等部位。ASPS通常表现为一种相对惰性但致命的肉瘤,特点是晚期转移和延长的临床病程[2]。转移通常是肺(90%)、骨(26%)和脑(11%~19%)[5,7-9]。已发表的报道显示与其他肉瘤相比,脑转移的发生率高出3倍[10]。
本例患者为年轻男性,病灶发生于上肢深部,病灶惰性生长5年余,直至发生肺和脑转移后出现临床症状才被重视治疗。
2.3 影像学表现
ASPS在影像学上具有独特的影像学特征,最突出的影像学特征是肿瘤内和肿瘤周围血管的存在,应该有助于诊断。
超声通常作为一种成像方式,从发育、炎症、创伤或肿瘤等方面对软组织病变进行鉴别。有报道显示,ASPS病灶多为边界清晰的低回声或混合回声肿块,伴肿瘤周围粗大血管影[11-12]。MRI提示ASPS的一个特征是肿瘤存在流空信号,流空信号同时存在于肿瘤的外围和中心[11,13-18],同时MRI和CT显示大多数肿瘤外围血管呈上下极分布,这些血管向肿瘤中心汇聚[13,18]。传统血管造影显示这个血管丰富的肿瘤动脉期有许多粗大扩张血管,动静脉分流,随后有明显的肿瘤染色,尽管血液分流很快,但造影剂从病变中流出速度很慢[14-17],呈现出快进慢出的特点。ASPS肿瘤在增强MRI或CT表现为明显强化[13,15-16,19],少数表现出中度强化[18],尚未见任何肿瘤显示出轻微强化或完全没有强化的报道。本文报道这例也显示肿瘤外围血管主要分布于肿瘤上下极,增强后肿瘤呈明显强化。
另一个比较特征性的表现是肿瘤在MRI的T1WI序列上相对于肌肉多表现出稍高信号[13,15-16,19],而其他软组织肉瘤多为等信号或低信号[20]。此外ASPS大多数肿瘤的边缘清晰呈分叶状,较少出现坏死和钙化,当出现坏死时,坏死总是位于病灶中心位置,周围为厚壁的存活肿瘤组织[18]。本文这例T1WI呈等、稍高信号,肿瘤较大呈分叶状,大部分边缘清晰,无坏死钙化。
ASPS肿瘤转移率高,有研究报道了转移瘤的影像学特点:肺是最常见的转移部位,其次是骨和脑[5,7-9,12-13],淋巴结转移少见[12,21];转移瘤与原发肿瘤同样表现为具有粗大血管及明显强化的富血管特征[22]。此病例出现了肺和脑转移瘤,脑转移瘤可见肿瘤周围血管影及肿瘤明显强化,与报道一致。
2.4 治疗及转归
ASPS的治疗通常包括原发肿瘤手术切除和转移性疾病的全身治疗。传统的蒽环类化疗在很大程度上是无效的,实体瘤的反应率低于10%[23-25]。
对一些患者来说,完全广泛切除可能是可以治愈的,复发率低,但肿瘤转移在长期随访中很常见,有时在原发肿瘤切除后10年或更长时间。与其他软组织肉瘤一样,一些患者可以采取转移瘤切除术,但手术切除如何影响这些患者的生存尚不清楚[5,26]。本文报道的病例因出现脑转移、影响脑功能,而选择脑转移瘤切除,患者生存情况有待随访。
2.5 诊断及鉴别诊断
ASPS的诊断主要依靠病理,但其比较有特征性影像学表现,也可以给临床医生提供一些诊断依据。然而这些肿瘤的常见表现是缓慢生长的无痛肿块及其多发畸形血管及富血管性,它们经常被误诊为动静脉畸形(arteriovenous malformation,AVM),这些肿瘤最终由于诊断延误而出现远处转移,因为被误诊为动静脉畸形后几乎不进行组织病理学检查或手术。Pennacchioli等[27]的研究表明,大约9%(3/33)的患者最初在MRI上被认是血管畸形,因此延误了诊断治疗。与ASPS相比,AVM通常缺乏软组织成分,它们在T1WI和T2WI主要表现为流空的低信号,增强显示为早期动脉供血和早期静脉冲洗[13,27];而ASPS则以软组织成分为主伴有多发的血管流空低信号,增强表现为长期肿瘤染色和晚期冲洗的富血供病变[28],且T1WI上相对于肌肉为稍高信号[13,15-16,19]。
另一个比较容易混淆的良性肿瘤是血管瘤。在Viry等[13]对6名患有ASPS的儿童的综述中,1例眼眶ASPS最初被怀疑是血管瘤并栓塞。然而,已知血管瘤发生在比ASPS年轻得多的年龄组,通常从出生起就存在;此外,与ASPS相比,它们在动脉早期开始强化,ASPS则在动脉晚期或静脉早期开始强化;而且动脉瘤在T1WI多呈等信号或稍低信号,T2WI呈明显高信号,ASPS在T1WI多呈稍高信号,T2WI呈稍高信号。
我们在鉴别这些明显强化的富血管性病变时,也要考虑到来源于肾和甲状腺原发性肿瘤的转移瘤的可能性[12],另外,血管瘤样的肿瘤,如血管肉瘤、血管外皮瘤也可能有类似的影像表现[28]。然而,这些血管瘤样肿瘤通常会出现出血坏死,而ASPS出血坏死少见。
总而言之,ASPS是一种罕见的在青少年和年轻人中呈懒惰生长的软组织肉瘤。其较大的均匀肿块伴瘤内及肿瘤上下极粗大血管比较有特征性,T1WI上呈稍高信号也是一大特征,通过T1WI、T2WI上细微信号差别可以与部分肿瘤进行鉴别。肿瘤早期广泛切除可能有助于延长病程,早期误诊可导致晚期疾病的转移。
-
![]()
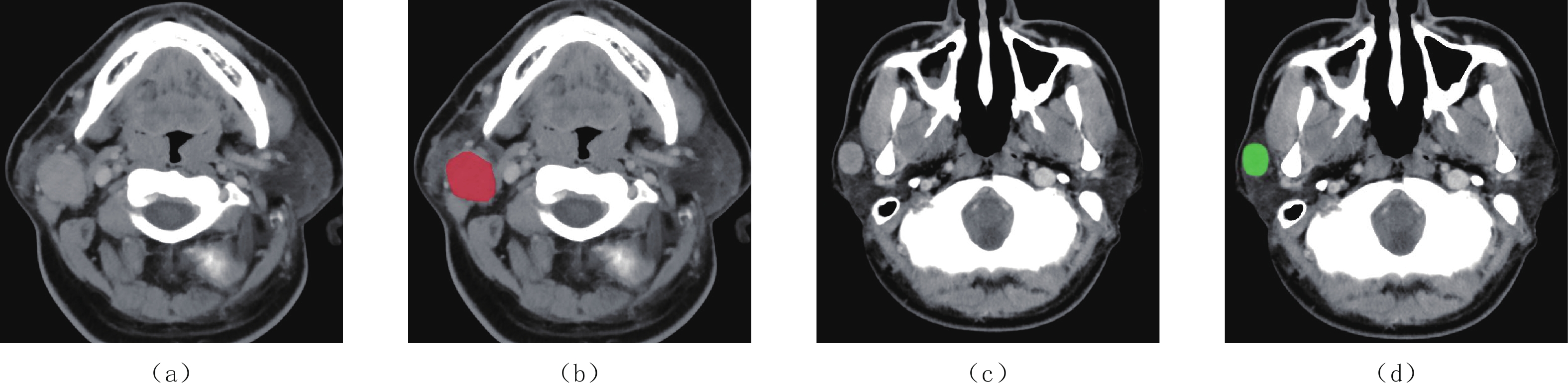
图 1 腮腺肿瘤CT静脉期图像以及ROIs
(a)和(b)腺淋巴瘤,男,45岁;(c)和(d)多形性腺瘤,男,40岁。
Figure 1. Enhanced CT images (with ROIs) of a parotid tumor
![]()
图 2 腮腺腺淋巴瘤与混合瘤组间WavEnHH_s-4、WavEnLL_s-4、GrVariance、GrSkewness、45 dgr_Fraction的ROC曲线
Figure 2. ROC curves for WavEnHH_s-4, WavEnLL_s-4, GrVariance, GrSkewness, 45 dgr_Fraction for differentiating between adenolymphomas and mixed tumors of the parotid gland
表 1 腮腺腺淋巴瘤与混合瘤间最佳纹理特征参数比较
Table 1 Comparison of the optimal texture feature parameters between parotid adenolymphomas and mixed tumors
参数 组别 统计检验 腺淋巴瘤组 混合瘤组 t/Z P WavEnHH_s-4 4.162±1.908 7.493±3.157 -4.084 <0.01 WavEnLL_s-4 21044.469±3887.164 16649.289±4309.226 3.392 0.002 GrVariance 0.185±0.046 0.236±0.033 -4.055 <0.01 GrSkewness 1.996±0.516 1.475±0.295 -3.291 0.001 45 dgr_Fraction 0.328±0.080 0.422±0.074 -3.854 <0.01  下载: 导出CSV
下载: 导出CSV
表 2 腮腺腺淋巴瘤与混合瘤间最佳纹理特征参数的诊断效能
Table 2 Diagnostic performance of the optimal texture feature parameters for parotid adenolymphomas and mixed tumors
参数 AUC 阈值 敏感性/% 特异性/% P WavEnHH_s-4 0.827 4.979 84.2 66.7 <0.01 WavEnLL_s-4 0.797 19227.148 84.2 76.2 0.001 GrVariance 0.815 0.200 89.5 66.7 0.001 GrSkewness 0.805 1.819 94.7 61.9 0.001 45 dgr_Fraction 0.802 0.384 73.7 71.4 0.001
下载: 导出CSV
表 3 腮腺腺淋巴瘤与混合瘤间不同机器学习算法的误判率
Table 3 False-positive rates of different machine-learning algorithms for parotid adenolymphomas and mixed tumors
组别 RDA/% PCA/% LDA/% NDA/% Fisher 37.5(15/40) 37.5(15/40) 10.0(4/40) 7.5(3/40) POE+ACC 35.0(14/40) 30.0(12/40) 22.5(9/40) 10.0(4/40) MI 30.0(12/40) 30.0(12/40) 37.5(15/40) 12.5(5/40) FPM 35.0(14/40) 32.5(13/40) 7.5(3/40) 5.0(2/40)
下载: 导出CSV
表 4 腮腺腺淋巴瘤与混合瘤间不同机器学习算法的效能比较
Table 4 Comparison of the performance of different machine-learning algorithms for parotid adenolymphomas and mixed tumors
分类算法 准确率/% 敏感性/% 特异性/% 阳性预测值 阴性预测值 Fisher/RDA 62.5 61.9 63.2 65.0 60.0 Fisher/PCA 62.5 61.9 63.2 65.0 60.0 Fisher/LDA 90.0 95.2 84.2 87.0 94.1 Fisher/NDA 92.5 90.5 94.7 95.0 90.0 POE+ACC/RDA 65.0 76.2 52.6 64.0 66.7 POE+ACC/PCA 70.0 76.2 63.2 69.6 70.6 POE+ACC/LDA 77.5 76.2 78.9 80.0 75.0 POE+ACC/NDA 90.0 85.7 94.7 94.7 85.7 MI/RDA 70.0 76.2 63.2 69.6 70.6 MI/PCA 70.0 76.2 63.2 69.6 70.6 MI/LDA 62.5 66.7 57.9 63.6 61.1 MI/NDA 87.5 81.0 94.7 94.4 81.8 FPM/RDA 65.0 66.7 63.2 66.7 63.2 FPM/PCA 67.5 71.4 63.2 68.2 66.7 FPM/LDA 92.5 95.2 89.5 90.9 94.4 FPM/NDA 95.0 95.2 94.7 95.2 94.7
下载: 导出CSV
-
[1] YAMAMOTO T, KIMURA H, HAYASHI K, et al. Pseudo-continuous arterial spin labeling MR images in Warthin tumors and pleomorphic adenomas of the parotid gland: Qualitative and quantitative analyses and their correlation with histopathologic and DWI and dynamic contrast enhanced MRI findings[J]. Neuroradiology, 2018, 60(8): 803−812. doi: 10.1007/s00234-018-2046-9
[2] ZHENG C Y, CAO R, GAO M H, et al. Comparison of surgical techniques for benign parotid tumours: A multicentre retrospective study[J]. International Journal of Oral & Maxillofacial Surgery, 2018, 48(2): 187−192.
[3] 胡涛, 刘琼, 邹玉坚, 等. 扩散峰度成像及动态增强MRI鉴别腮腺多形性腺瘤与Warthin瘤[J]. 放射学实践, 2021,36(9): 1089−1094. HU T, LIU Q, ZOU Y J, et al. Application value of DKI and DEC-MRI in the differential diagnosis of parotid pleomorphic adenoma and Warthin tumor[J]. Journal of Radiology Practice, 2021, 36(9): 1089−1094. (in Chinese).
[4] PARK H J, LEE S M, SONG J W, et al. Texture-based automated quantitative assessment of regional patterns on initial CT in patients with idiopathic pulmonary fibrosis: Relationship to decline in forced vital capacity[J]. American Journal of Roentgenology, 2016, 207(5): 976−983. doi: 10.2214/AJR.16.16054
[5] AHN S J, KIM J H, PARK S J, et al. Prediction of the therapeutic response after FOLFOX and FOLFIRI treatment for patients with liver metastasis from colorectal cancer using computerized CT texture analysis[J]. European Journal of Radiology, 2016, 85: 1867−1874. doi: 10.1016/j.ejrad.2016.08.014
[6] 刘文华, 张衡, 李敏, 等. CT图像纹理分析鉴别诊断腮腺混合瘤与腺淋巴瘤[J]. 临床放射学杂志, 2019,38(12): 2271−2274. LIU W H, ZHANG H, LI M, et al. CT texture analysis in the differential diagnosis of mixed tumor of parotid gland and adenolymphoma[J]. Journal of Clinical Radiology, 2019, 38(12): 2271−2274. (in Chinese).
[7] 任思桐, 李小虎, 刘斌, 等. CT平扫图像纹理分析鉴别腮腺多形性腺瘤与恶性肿瘤的初步研究[J]. CT理论与应用研究, 2019,28(6): 685−691. DOI: 10.15953/j.1004-4140.2019.28.06.06. REN S T, LI X H, LIU B, et al. Preliminary study on differentiating pleomorphic adenoma and malignant tumors of the parotid gland by texture analysis of non-enhanced CT images[J]. CT Theory and Applications, 2019, 28(6): 685−691. DOI: 10.15953/j.1004-4140.2019.28.06.06. (in Chinese).
[8] 茂盛, 王嗣伟, 晋丹丹, 等. 腮腺多形性腺瘤与腺淋巴瘤的CT影像特征及对比分析[J]. 实用放射学杂志, 2019,33(1): 28−46. MAO S, WANG S W, JIN D D, et al. CT imaging characteristics and comparative analysis of parotid pleomorphic adeonoma and adenolymphoma[J]. Journal of Practical Radiology, 2019, 33(1): 28−46. (in Chinese).
[9] 茅枭骁, 征锦. CT纹理分析技术在甲状腺结节影像研究中的应用进展[J]. 医疗卫生装备, 2020,41(12): 97−100. MAO X X, ZHENG J. Research progress of CT texture analysis for imaging studies of thyroid nodules[J]. Medical and Health Equipment, 2020, 41(12): 97−100. (in Chinese).
[10] 任继亮, 吴颖为, 陶晓峰, 等. 常规MRI纹理分析鉴别诊断眼眶淋巴瘤与炎性假瘤[J]. 中国医学影像技术, 2017,33: 980−984. REN J L, WU Y W, TAO X F, et al. MRI texture analysis in differential diagnosis of orbital lymphoma and inflammatory pseudotumor[J]. Chinese Journal of Medical Imaging Technology, 2017, 33: 980−984. (in Chinese).
[11] DODGSON T, MEDICINES M D, SCHEDAR N, et al. Can quantitative CT texture analysis be used to differentiate fat-poor renal policewoman from renal cell carcinoma on enhancement CT images[J]. Radiology, 2015, 276(3): 787−796. doi: 10.1148/radiol.2015142215
[12] SUDARSHAN V K, MOOKIAH M R, ACHARYA U R, et al. Application of wavelet techniques for cancer diagnosis using ultrasound images: A review[J]. Computers in Biology & Medicine, 2016, 69: 97−111.
[13] 徐圆, 段钰, 吴晶涛, 等. 基于CT增强扫描的纹理分析技术鉴别肾脏透明细胞癌恶性程度的可行性研究[J]. 临床放射学杂志, 2019,38: 1693−1697. XU Y, DUAN Y, WU J T, et al. Preoperative assessment of pathological grade of clear cell renal cell carcinoma by texture analysis based on CT enhanced images[J]. Journal of Clinical Radiology, 2019, 38: 1693−1697. (in Chinese).
[14] 周明, 钱斌, 翟晓东. 腮腺腺淋巴瘤与多形性腺瘤的双期增强CT表现与鉴别[J]. 临床放射学杂志, 2012,31: 1243−1246. ZHOU M, QIAN B, ZHAI X D. CT differential diagnosis between parotid gland lymphoma and pleomorphic adenoma[J]. Journal of Clinical Radiology, 2012, 31: 1243−1246. (in Chinese).
[15] 余先超, 孙宇凤, 李鹏, 等. 影像组学在腮腺多形性腺瘤与腺淋巴瘤鉴别诊断中的应用[J]. 现代肿瘤医学, 2021,29(5): 837−840. doi: 10.3969/j.issn.1672-4992.2021.05.025 YU X C, SUN Y F, LI P, et al. Application of radiomics in the differential diagnosis of parotid pleomorphic adenoma and adenolymphoma of the parotid gland[J]. Modern Oncology, 2021, 29(5): 837−840. (in Chinese). doi: 10.3969/j.issn.1672-4992.2021.05.025
[16] 尹进学, 汤日杰, 钟熹, 等. 常规T2WI纹理分析预测早期宫颈鳞癌盆腔淋巴结转移的价值[J]. 临床放射学杂志, 2020,39: 358−362. YIN J X, TANG R J, ZHONG X, et al. Value of conventional T2-weighted images texture analysis in predicting pelvic lymph node metastasis in early-stage cervical cancer[J]. Journal of Clinical Radiology, 2020, 39: 358−362. (in Chinese).
[17] 徐圆, 段钰, 曹正业, 等. CT纹理组学联合机器学习预测肺腺癌淋巴结转移[J]. 临床放射学杂志, 2020,39: 691−695. XU Y, DUAN Y, CAO Z Y, et al. Value of texture analysis combined with machine learning based on enhanced CT of lung adenocarcinoma in prediction of lymph node metastasis[J]. Journal of Clinical Radiology, 2020, 39: 691−695. (in Chinese).





计量
- 文章访问数: 261
- HTML全文浏览量: 163
- PDF下载量: 28


