
CT Spectral Imaging Study in Patients with Carotid Body Tumors at High Altitudes
-
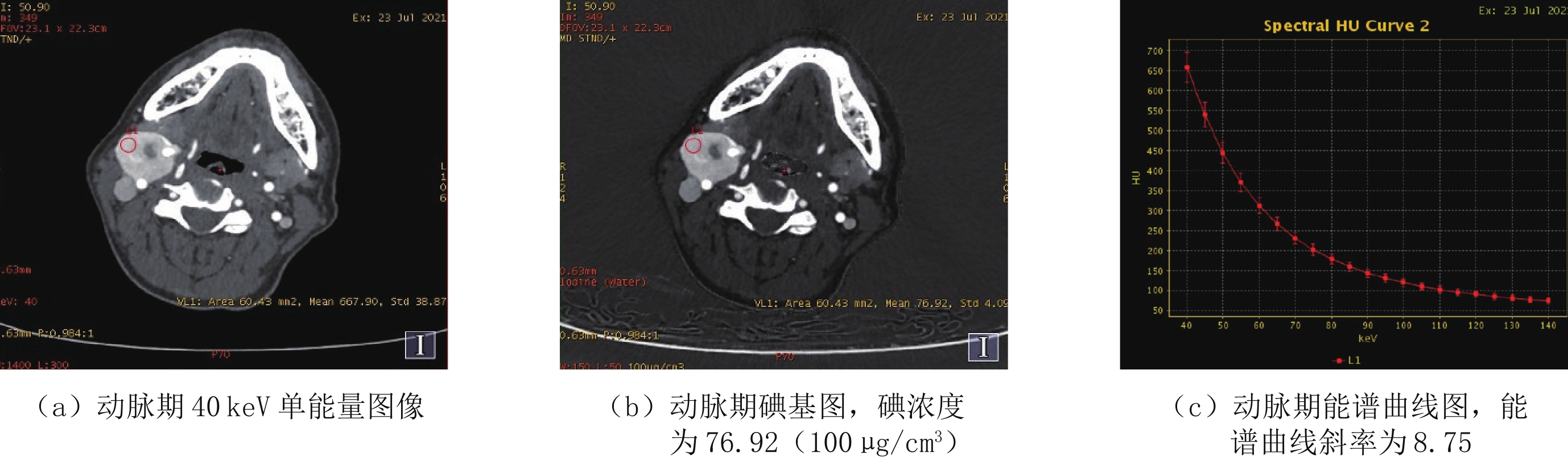
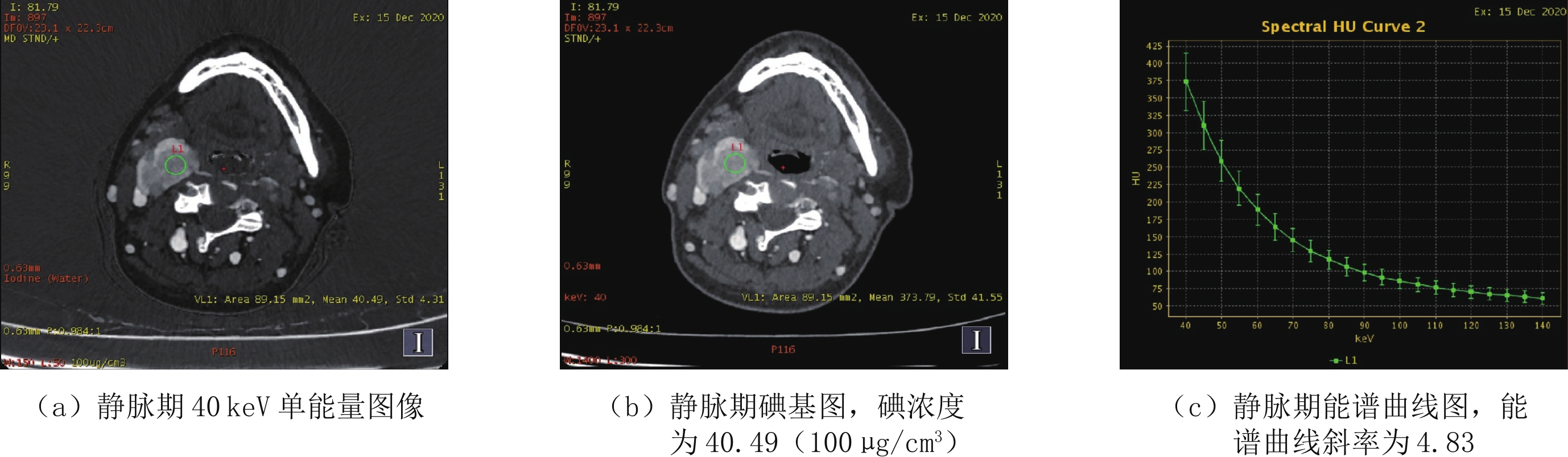
摘要: 目的:探讨CT能谱成像对颈动脉体瘤(CBT)的研究价值。方法:收集30例接受CT能谱检查并经手术确诊的CBT患者,通过GSI Viewer重建60 keV和40 keV单能量图像,对40 keV、60 keV单能量图像及120 kVp like三组图像的CBT供血动脉CT值、背景噪声(SD)、对比噪声比(CNR)、信噪比(SNR)及主观评分进行统计分析,分析CBT能谱参数及影像特征与手术结果的关系。结果:CBT动脉期及静脉期能谱参数与手术结果均无相关性;CBT横径、纵径、Shamblin分型与术中出血量呈强相关,供血动脉数量与术中出血量呈中度相关;横径、纵径、Shamblin分型与颅神经损伤呈中度相关,供血动脉数量与颅神经损伤呈强相关;40 keV是CBT供血动脉显示的最佳能级,CT值、SD、CNR及SNR均显著高于60 keV组及120 kVp like组,60 keV组CT值、噪声显著高于120 kVp like组,二者CNR及SNR差异无统计学意义;40 keV组主观评价分值最高,两位放射科医师主观评分一致性良好。结论:①CBT动脉期及静脉期能谱参数与GAPP评分无相关性;②CBT供血动脉数量是评估手术并发症重要参数之一,40 keV单能量图像可明显优化CBT供血动脉显示。Abstract: Objective: To investigate the value of CT spectral imaging in the study of carotid body tumors (CBT). Methods: Thirty patients with CBT who underwent CT energy spectrum examination and were confirmed by operation were included. Subsequently, 60 keV and 40 keV single energy images were reconstructed through the GSI viewer. The CT value, background noise (SD), contrast noise ratio (CNR), signal-to-noise ratio (SNR), and subjective score of CBT feeding arteries of the 40 keV, 60 keV single energy images and 120 kVp like images were statistically analyzed to evaluate the relationship between CBT energy spectrum parameters and imaging features with surgical results. Results: There was no correlation between energy spectrum parameters in the arterial and venous phases of CBT and the surgical results. However, CBT transverse diameter, longitudinal diameter, and Shamblin classification were strongly correlated with intraoperative bleeding, and the number of feeding arteries was moderately correlated with intraoperative bleeding. Additionally, the transverse diameter, longitudinal diameter, and Shamblin classification were moderately correlated with cranial nerve injury, and the number of feeding arteries was strongly correlated with cranial nerve injury. We also found that 40 keV was the best energy level for the CBT feeding artery display. Furthermore, the CT value, SD, CNR, and SNR of the 60 keV group were significantly higher than those of the 60 keV and 120 kVp like groups, and the CT value and noise of the 60 keV group were significantly higher than those of the 120 kVp like group. However, there was no significant difference in CNR and SNR between the two groups. The subjective evaluation score of the 40 keV group was the highest, and the subjective evaluation of the two radiologists had good consistency. Conclusion: (1) There was no correlation between the energy spectrum parameters in the arterial and venous phases of CBT and GAPP score. (2) The number of CBT feeding arteries is one of the important parameters for evaluating surgical complications and 40 keV single energy imaging can significantly optimize the display of CBT feeding arteries.
-
Keywords:
- CT spectral imaging /
- carotid body tumor /
- image quality /
- differentiation degree
-
新型冠状病毒感染(coronavirus disease 2019,COVID-19)自2019年底开始持续流行,SARS-CoV-2经过了多次的突变和变异,从原始株、德尔塔株,再到目前流行的奥密克戎(Omicron)株,已出现了多种变异毒株谱系[1-2]。
COVID-19病毒为β属的新型冠状病毒[3],其传播能力强,3年来已在全球多国蔓延。胸部CT检查在COVID-19的早期筛查、临床诊治以及病程观察中起着非常重要的作用[4-5]。按照新型冠状病毒感染诊疗方案(试行第十版)[6]进行COVID-19临床分型,轻型胸部CT表现无异常,本研究未纳入。既往COVID-19死亡病例多为重症(重型、危重型)患者,因此对于中型患者临床转归的研究就显得尤为重要。
本研究回顾性分析126例内蒙古自治区人民医院就诊的感染奥密克戎BF.7毒株的不同临床转归的中型COVID-19患者胸部CT,为临床诊治、预后评估提供参考。
1. 资料与方法
1.1 病例资料
回顾性分析2022年12月1日至2023年1月31日在内蒙古自治区人民医院确诊的126例Omicron变异株BF.7感染临床分型为中型的成年COVID-19病例,均有流行病学史。根据《新型冠状病毒感染诊疗方案(试行第十版)》临床诊断是否转为重症(重型/危重型)分为A组(未转为重症)、B组(转为重症)。A组103例,男65例,女38例,平均年龄(73.98±11.53)岁;B组23例,B组23例,男16例,女7例,平均年龄(73.43±12.53)岁。
纳入标准:符合新型冠状病毒感染诊疗方案(试行第十版)的临床诊断标准,具有完整CT检查资料且图像无伪影;排除标准:轻型及首诊即为重症患者;未成年(18岁以下)病例;患有肺部肿瘤、肺结核及其他肺部感染性疾病的病例;患有基础疾病如肺气肿,肺间质纤维化等影响病灶准确判断的病例;图像质量差、呼吸伪影严重等影像观察的病例。
1.2 影像检查方法
使用64排及以上螺旋CT,患者采用仰卧位,扫描范围从胸廓入口至包全肺底。扫描参数:管电压120 kV,自动管电流,层厚5 mm,重建1~1.25 mm,矩阵512×512。
1.3 资料分析
胸部CT薄层图像由两名高年资影像诊断医师进行阅片,统计病灶的分布特点及CT影像征象特征,当诊断结果出现争议时,再由第3名工作10年以上经验丰富的影像医学科胸组医生裁定。
1.4 统计学方法
A组(未转为重症)与B组(转为重症)两组患者性别构成、病灶分布及特征采用例数(构成比)描述,患者平均年龄采用(均数±标准差)描述,采用t检验比较,患者感染病灶占比采用中位数(四分位间距)描述,组间比较采用非参数U检验。以P≤0.05为差异具有统计学意义。
2. 结果
本研究126例患者,根据不同临床转归分为A组和B组,两组病例性别、平均年龄差异无统计学意义;病灶在左肺上叶、下叶、右肺上叶、中叶、下叶及双肺中分布体积占比高于A组(表1)。
表 1 126例中型COVID-19患者分组情况Table 1. Grouping of 60 patients with COVID-19分组 组别 统计检验 A组(n=103) B组(n=23) 统计量 P 病灶分布体积占比(%) 左肺上叶 11.0(16.6) 36.7(26.7) 4.623 <0.001 左肺下叶 32.7(29.3) 56.3(30.4) 3.278 0.001 右肺上叶 12.6(28.6) 36.4(29.5) 4.282 <0.001 右肺中叶 15.5(29.4) 34.7(32.7) 3.246 0.001 右肺下叶 30.9(30.9) 58.0(29.8) 4.067 <0.001 双肺 19.0(19.7) 40.5(12.0) 5.444 <0.001 年龄 平均年龄/岁 73.98±11.53 73.43±12.53 0.202 0.192 ${M}({Q_2}~{Q_3})$ 74.0(16.0) 75.0(19.0) 0.840 0.957 年龄范围/岁 44~95 48~89 两组病灶均以双肺分布磨玻璃阴影、实变为主。大部分呈双肺多叶分布。A组右肺上叶7例(7/103)、右肺中叶2例(2/103),左肺上叶、下叶各1例(1/103)无病灶分布;B组除1例(1/23)左肺下叶无病灶分布外其余22例(22/23)均为双肺5个肺叶分布。两组均可见大小不等磨玻璃斑片影、磨玻璃结节影,部分较淡薄,或部分实变影,索条、实变、铺路石征、小叶间隔增厚及病灶内增粗血管影,沿支气管血管束分布或肺叶外周带及胸膜下分布多见(图1和图2)。B组呈双肺胸膜下及肺叶外周带为主磨玻璃斑片影及实变,部分实变范围扩大,表现为双肺大片状磨玻璃影、实变,沿支气管血管束分布,可见多发条索及空气支气管征;B组病灶吸收较普通型A组慢。B组复查可见1例胸腔积液(图3),均未见纵隔、肺门淋巴结肿大。
![]() 图 1 COVID-19中型未转重症病例男,83岁。(a)2022.12.29双肺条片状磨玻璃密度影,胸膜下分布为主,可见增粗小血管。(b)2023.01.04磨玻璃影伴部分实变,可见小叶间隔增厚,可见索条。Figure 1. COVID-19 medium type that did not progress to a severe case
图 1 COVID-19中型未转重症病例男,83岁。(a)2022.12.29双肺条片状磨玻璃密度影,胸膜下分布为主,可见增粗小血管。(b)2023.01.04磨玻璃影伴部分实变,可见小叶间隔增厚,可见索条。Figure 1. COVID-19 medium type that did not progress to a severe case![]() 图 2 COVID-19中型未转重症病例男,52岁。(a)和(b)2022.12.19双肺斑片状磨玻璃密度影,胸膜下分布为主,部分沿支气管血管束分布。(c)和(d)2022.12.22双肺斑片状磨玻璃影范围较前增大,密度较前增高,伴部分实变,可见索条。Figure 2. COVID-19 medium type that did not progress to a severe case
图 2 COVID-19中型未转重症病例男,52岁。(a)和(b)2022.12.19双肺斑片状磨玻璃密度影,胸膜下分布为主,部分沿支气管血管束分布。(c)和(d)2022.12.22双肺斑片状磨玻璃影范围较前增大,密度较前增高,伴部分实变,可见索条。Figure 2. COVID-19 medium type that did not progress to a severe case![]() 图 3 男,COVID-19中型转重症病例男,50岁。(a)2022.11.30左肺不规则片状实变,胸膜下为著,另多发小片状磨玻璃影。(b)2022.12.03病灶范围较前增大,密度增高,左侧少量胸腔积液。Figure 3. COVID-19 medium type that progressed to a severe case
图 3 男,COVID-19中型转重症病例男,50岁。(a)2022.11.30左肺不规则片状实变,胸膜下为著,另多发小片状磨玻璃影。(b)2022.12.03病灶范围较前增大,密度增高,左侧少量胸腔积液。Figure 3. COVID-19 medium type that progressed to a severe case3. 讨论
随着SARS-CoV-2的不断变异,越来越多的不同变异株相继出现且倍受关注[7]。普通X线检查由于密度分辨率较差,肺部病灶特别是早期病灶漏诊率高,主要用于部分危重症患者的床旁摄影。胸部CT检查在COVID-19的早期筛查、快速检出微小病灶、临床病情评估以及病程观察中起着非常重要的作用[8]。本研究希望通过对比不同临床转归Omicron BF.7感染患者胸部CT特征的差异,为临床诊治、评估预后提供参考。
本研究中型COVID-19胸部CT多呈双肺多发形态不规则病灶,呈多样性,多为斑片状、楔形、类圆形,病灶多呈淡薄磨玻璃影,密度不均,可夹杂实变病灶,也可呈边缘模糊、伴有晕征的小叶中心结节,部分可见小血管增粗及空气支气管征;多以胸膜下肺外周分布为主,更容易出现沿支气管血管束分布,与之前研究报道结果基本一致[9],可能由于Omicron变异株在支气管中的复制优于在肺实质内[10]。病灶以肺外周带、下肺背侧胸膜下区及肺底多见,内可见小血管增粗或网格状小叶间隔增厚,随着病变进展表现为呈双侧非对称性胸膜下实变病灶,以双肺下叶分布为主,部分沿支气管血管束分布,同之前的研究[11]。转为重症(重型/危重型)的B组平均年龄较A组差异无统计学意义,与之前的研究结果不同[12],考虑与B组样本量较小及本研究未纳入可能病情较轻未至医院就诊的病例有关,存在病例选择偏倚。
胸部CT多表现为双肺弥漫磨玻璃密度影合并实变,可见空气支气管征,病灶分布随病情进展自胸膜下向肺门方向播散,病灶累及肺叶数量高于A组患者,两组患者均未见淋巴结肿大。本研究患者胸部CT可见斑片状磨玻璃密度影,可能是由于病毒定植于肺泡和呼吸性细支气管上皮[13],而病灶右肺下叶较常见可能与病毒更容易进入粗而短的右肺下叶支气管有关,同之前研究[12]。
同种类型病毒性肺炎可有类似表现[14],单纯影像表现很难鉴别;严重急性呼吸综合征和中东呼吸综合征的胸部影像学异常常见于单侧[15],有研究报道严重急性呼吸综合征单侧病灶的发病概率为54.6%[16],但新冠感染患者更倾向于累及双肺。另外,胸腔积液较COVID-19较常见[17-18]。甲型H1N1肺炎常合并胸腔积液和纵隔、肺门淋巴结轻度肿大[19],且患者多以中青年为主,临床进展较缓慢[20]。H7 N9禽流感肺炎早期可见病变同时发生于中心及外周,以一侧肺多见[21],胸腔积液较常见[22]。隐源性机化性肺炎以复发性或游走性的斑片状磨玻璃密度灶或实变灶为特征性CT表现[23-24]。
本研究的不足与局限:①未考虑患者治疗过程对临床转归的影响,譬如是否使用小分子抗病毒药物以及使用的时间等,对研究结果有一定的影响;②转为重症的病例均直接来自于临床指标的诊断,缺少24~48 h内的胸部影像学明显进展>50% 的影像证据;③本研究的图像来源于不同品牌的 CT设备,对病灶细节的观察略有影响。
综上所述,中型COVID-19不同临床转归病例胸部CT具有一定特点,对有重症转归倾向患者及早评估有助于COVID-19重症率的控制。
-
![]()
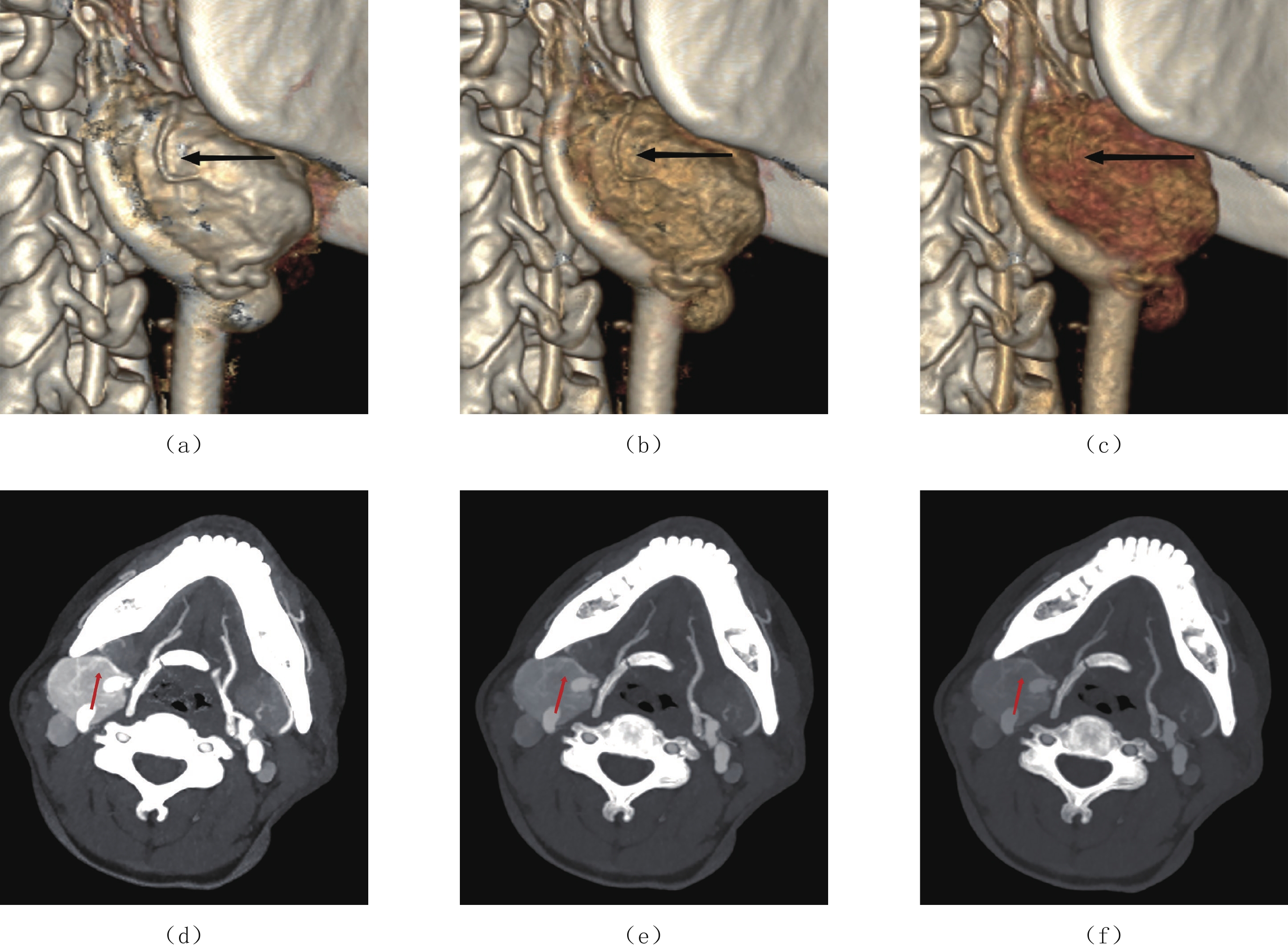
图 1 女,53岁,右侧颈动脉体瘤
(a)~(c)分别为CBT 40 keV、60 keV及120 kVp like的VR图像,黑色箭头所指为供血动脉;(d)~(f)分别为CBT 40 keV、60 keV及120 kVp like的MIP图像,红色箭头所指为供血动脉。
Figure 1. A right carotid body tumor of a 53-year-old female
表 1 30例患者的一般资料(
$\bar x \pm s $ )Table 1 The general information of 30 patients
$(\bar x \pm s )$ 变量 参数 数值(%) 变量 参数 数值(%) 年龄/岁 55.8±10.3 供血动脉数量/例 1支 15(50.0) 性别/例 男性 3(10.0) 2支 10(33.3) 女性 27(90.0) 3支及以上 5(16.7) 位置/例 左侧 13(43.3) Shamblin分型/例 Ⅰ型 13(43.3) 右侧 12(40.0) Ⅱ型 7(23.3) 双侧 5(16.7) Ⅲ型 10(33.3) 影像学特征 横径/cm 3.07±1.34 并发症 术中出血量/mL 157.3±237.5 纵径/cm 3.37±1.38 颅神经损伤 18(60.0)  下载: 导出CSV
下载: 导出CSV
表 2 CBT能谱参数及影像特征与手术结果的相关性分析
Table 2 Correlation analysis between CBT energy spectrum parameters, image characteristics, and surgical results
变量 参数 术中出血量 颅神经损伤 GAPP评分 r1 P1 r2 P2 r3 P3 动脉期能谱参数 碘浓度 0.104 0.791 0.414 0.268 -0.393 0.296 能谱曲线斜率 0.104 0.790 0.416 0.266 -0.341 0.369 有效原子序数 0.052 0.894 0.416 0.266 -0.366 0.332 静脉期能谱参数 碘浓度 -0.207 0.593 0.268 0.456 0.243 0.529 能谱曲线斜率 -0.311 0.416 0.151 0.699 0.076 0.847 有效原子序数 -0.156 0.689 0.192 0.620 0.117 0.765 影像特征 横径 0.788 0.000 0.476 0.008 0.296 0.112 纵径 0.669 0.000 0.550 0.002 0.287 0.124 供血动脉数量 0.583 0.001 0.629 0.000 0.209 0.268 Shamblin分型 0.672 0.000 0.529 0.003 0.276 0.140 注:r1、P1:术中出血量相关性分析结果;r2、P2:颅神经损伤相关性分析结果;r3、P3:GAPP评分相关性分析结果。
下载: 导出CSV
表 3 CBT术中出血量多因素线性回归分析
Table 3 Multivariate linear regression analysis of the intraoperative bleeding volume in CBT
变量 回归参数 统计校验 偏回归系数 标准误 标准回归系数 t P 常数 -184.039 97.241 -1.893 0.070 横径 96.770 39.797 0.538 2.432 0.023 纵径 -91.715 47.085 -0.521 -1.948 0.063 供血动脉数量 82.816 55.992 0.264 1.479 0.152 Shamblin分型 111.139 67.763 0.421 1.640 0.114
下载: 导出CSV
表 4 CBT颅神经损伤多因素线性回归分析
Table 4 Multivariate linear regression analysis of cranial nerve injury in CBT
变量 回归参数 统计校验 偏回归系数 标准误 标准回归系数 t P 常数 -0.889 0.392 -2.268 0.032 横径 -0.108 0.161 -0.143 -.676 0.505 纵径 0.177 0.190 0.239 0.931 0.361 供血动脉数量 0.709 0.226 0.538 3.140 0.004 Shamblin分型 0.229 0.273 0.206 0.838 0.410
下载: 导出CSV
表 5 供血动脉数量与影像特征及手术结果分析(
$\bar x \pm s $ )Table 5 Analysis of the number of feeding arteries, imaging characteristics and surgical results
$(\bar x \pm s) $ 变量 1支/% 2支/% 3支及以上/% P Shamblin分型 横径/cm 2.27±1.00 3.66±1.19a 4.20±1.05b 0.001 纵径/cm 2.61±1.40 3.81±0.81a 4.16±1.23b 0.019 Ⅰ型 10(33.33) 3(10.00) 0 0.005 Ⅱ型 3(10.00) 3(10.00) 1(3.33) Ⅲ 型 2(6.67) 4(13.33) 4(13.33) 术中出血量/mL 56.00±35.01 178.00±121.36a 420.00±495.72b 0.001 颅神经损伤/支 6(20.69) 12(41.38)a 11(37.93)b 0.000 GAPP评分 4.27±1.10 5.10±0.57a 4.20±0.84 0.073 注:供血动脉数量1支与2支相比,a:P<0.05;1支与3支及以上相比,b:P<0.05。
下载: 导出CSV
表 6 各组图像CT值、噪声、SNR及CNR比较(
$\bar x \pm s $ )Table 6 Comparison of the CT values, noise, SNR and CNR of each group
$(\bar x \pm s )$ 项目 组别 统计检验 40 keV组 60 keV组 120 kVp like组 F P CT供血动脉/HU 679.17±216.65 337.28±96.82c 228.54±60.82d 129.64 0.000 SD脂肪/HU 23.11±4.83 13.10±2.73c 9.78±2.17d 143.091 0.000 CNR 27.71±12.02 22.28±8.65c 18.84±7.82d 9.768 0.001 SNR 30.62±12.37 26.64±9.13c 24.39±8.60d 4.858 0.010 注:40 keV组与60 keV组比较,c:P<0.05;40 keV组与120 kVp like组比较,d:P<0.05。
下载: 导出CSV
表 7 颈动脉体瘤供血动脉主观评分(
$\bar x \pm s $ )Table 7 Subjective scores of the feeding artery of the carotid body tumor
$(\bar x \pm s) $ 评分者 组别 统计检验 40 keV组 60 keV组 120 kVp like组 H P 医师A 4.85±0.72 3.68±0.68 2.55±0.36 58.305 0.000 医师B 4.80±0.71 3.53±0.66 2.41±0.41 54.765 0.000
下载: 导出CSV
-
[1] 朱吉海, 杨佳, 马伟, 等. 高海拔地区颈动脉体瘤围术期颈动脉处理策略−单中心经验[J]. 中国普通外科杂志, 2020,29(12): 1521−1527. doi: 10.7659/j.issn.1005-6947.2020.12.015 [2] 医学会内分泌学分会. 嗜铬细胞瘤和副神经节瘤诊断治疗专家共识(2020版)[J]. 中华内分泌代谢杂志, 2020,36(9): 737−750. doi: 10.3760/cma.j.cn311282-20200629-00482 Endocrinology Branch of the Medical Association. Expert consensus on the diagnosis and treatment of pheochromocytoma and paraganglioma (2020)[J]. Chinese Journal of Endocrinology and Metabolism, 2020, 36(9): 737−750. (in Chinese). doi: 10.3760/cma.j.cn311282-20200629-00482
[3] SCHWARZE V, MARSCHNER C, de FIGUEIREDO G, et al. Single-center study: Dynamic contrast-enhanced ultrasound in the diagnostic assessment of carotid body tumors[J]. Quantitative Imaging in Medicine and Surgery, 2020, 10(9): 1739−1747. doi: 10.21037/qims-19-920
[4] KIMURA N, TAKAYANAGI R, TAKIZAWA N, et al. Pathological grading for predicting metastasis in phaeochromocytoma and paraganglioma[J]. Endocrine-Related Cancer, 2014, 21(3): 405−414. doi: 10.1530/ERC-13-0494
[5] ROBERTSON V, POLI F, HOBSON B, et al. A systematic review and meta-analysis of the presentation and surgical management of patients with carotid body tumours[J]. European Journal of Vascular and Endovascular Surgery, 2019, 57(4): 477−486. doi: 10.1016/j.ejvs.2018.10.038
[6] 顾光超, 郑月宏. 颈动脉体瘤的PUMCH分型[J]. 协和医学杂志, 2021,12(6): 825−828. GU G C, ZHENG Y H. The PUMCH classification of carotid body tumor[J]. Medical Journal of Peking Union Medical College Hospital, 2021, 12(6): 825−828. (in Chinese).
[7] 李展展, 梁琰, 张永强, 等. 头颈部CT血管成像对颈动脉体瘤术中出血量评估的临床应用价值[J]. 中国医学科学院学报, 2020,42(4): 491−496. LI Z Z, LIANG Y, ZHANG Y Q, et al. Value of head and neck CT angiography in the clinical evaluation of intraoperative bleeding volume of carotid body tumours[J]. Acta Academiae Medicinae Sinicae, 2020, 42(4): 491−496. (in Chinese).
[8] HOANG V T, TRINH C T, LAI T A K, et al. Carotid body tumor: A case report and literature review[J]. Journal of Radiology Case Reports, 2019, 13(8): 19−30.
[9] 中华放射学杂志双层探测器光谱CT临床应用协作组. 双层探测器光谱CT临床应用中国专家共识(第一版)[J]. 中华放射学杂志, 2020,54(7): 635−643. doi: 10.3760/cma.j.cn112149-20200513-00679 Chinese Journal of Radiology Cooperative Group of Clinical Application of Dual-layer Spectral Detector CT. China expert consensus on clinical application of dual-layer spectral detector CT[J]. Chinese Journal of Radiology, 2020, 54(7): 635−643. (in Chinese). doi: 10.3760/cma.j.cn112149-20200513-00679
[10] LUNA-ORTIZ K, RASCON-ORTIZ M, VILLAVICENCIO-VALENCIA V, et al. Does Shamblin's classification predict postoperative morbidity in carotid body tumors? A proposal to modify Shamblin's classification[J]. European Archives of Oto-rhino-laryngologyl, 2006, 263(2): 171−175. doi: 10.1007/s00405-005-0968-4
[11] LI N, ZENG N, WAN Y, et al. The earlier, the better: The beneficial effect of different timepoints of the preoperative transarterial embolization on ameliorating operative blood loss and operative time for carotid body tumor[J]. Surgery, 2021, 170(5): 1581-1585.
[12] 东强, 曲丽洁, 张宏, 等. 双能量CT碘值及增强值与进展期胃腺癌病理分化程度的相关性[J]. 临床放射学杂志, 2020,39(5): 931−935. DONG Q, QU L J, ZHANG H, et al. Correlations between the iodine value and CT enhancement value of dual-energy CT and the pathological differentiation degree of advanced gastric adenocarcinoma[J]. Journal of Clinical Radiology, 2020, 39(5): 931−935. (in Chinese).
[13] 曹云太, 鲍海华, 张国晋, 等. 颈动脉体瘤术前影像学特征与手术并发症的相关性研究[J]. 临床放射学杂志, 2021,40(2): 220−224. CAO Y T, BAO H H, ZHANG G J, et al. Correlation between preoperative imaging features and operative complications of carotid body tumors[J]. Journal of Clinical Radiology, 2021, 40(2): 220−224. (in Chinese).
[14] 中华医学会放射学分会. 头颈部CT血管成像扫描方案与注射方案专家共识[J]. 中华放射学杂志, 2019,53(2): 81−87. doi: 10.3760/cma.j.issn.1005-1201.2019.02.001 Chinese Society of Radiology, Chinese Medical Association. Expert consensus of the head and neck CT angiography scanning and injection protocols[J]. Chinese Journal of Radiology, 2019, 53(2): 81−87. (in Chinese). doi: 10.3760/cma.j.issn.1005-1201.2019.02.001
[15] 马光明, 于勇, 陈静, 等. 能谱CT单能量技术优化头颈CTA图像质量研究[J]. 中国医疗设备, 2021,36(8): 86−89. doi: 10.3969/j.issn.1674-1633.2021.08.021 MA G M, YU Y, CHEN J, et al. Research on optimization of head and neck CTA image qualityby spectrum CT optimal monochromatic image technique[J]. China Medical Devices, 2021, 36(8): 86−89. (in Chinese). doi: 10.3969/j.issn.1674-1633.2021.08.021
[16] 邓小林, 谢惠, 屈亚林, 等. 能谱CT最佳单能量技术优化头颈部CTA图像质量的研究[J]. CT理论与应用研究, 2018,27(6): 719−726. DOI: 10.15953/j.1004-4140.2018.27.06.05. DENG X L, XIE H, QU Y L, et al. Spectral CT with optimal monochromatic energy to improve CTA image quality of head and neck[J]. Computerized Tomography Theory and Applications, 2018, 27(6): 719−726. DOI: 10.15953/j.1004-4140.2018.27.06.05. (in Chinese).
[17] MCCOLLOUGH C H, YU L, KOFLER J M, et al. Degradation of CT low-contrast spatial resolution due to the use of iterative reconstruction and reduced dose levels[J]. Radiology, 2015, 276(2): 499−506. doi: 10.1148/radiol.15142047
[18] 严福华, 金征宇. 开辟双能量CT临床应用的新时代[J]. 中华放射学杂志, 2020,54(6): 505−507. doi: 10.3760/cma.j.cn112149-20200324-00450 YAN F H, JIN Z Y. Open up a new era about the clinical application of dual-energy CT[J]. Chinese Journal of Radiology, 2020, 54(6): 505−507. (in Chinese). doi: 10.3760/cma.j.cn112149-20200324-00450
[19] 冯瑶杰, 吕艳娥, 瞿姣, 等. 双能CT评估喉部鳞癌分化程度[J]. 中国医学影像技术, 2021,37(7): 1002−1006. FENG Y J, LU Y E, QU J, et al. Dual-energy CT for evaluation on differentiation degrees of laryngeal squamous cell carcinoma[J]. Chinese Journal of Medical Imaging Technology, 2021, 37(7): 1002−1006. (in Chinese).











计量
- 文章访问数: 385
- HTML全文浏览量: 173
- PDF下载量: 23


