
Correlation Between MRI Changes and Bone Mineral Density in Patients with Knee Osteoarthritis
-
摘要:
目的:分析探讨膝骨关节炎(KOA)患者软骨损伤、骨髓水肿分别与全身骨密度的关系。方法:选取2023年1月至2023年10月四川省骨科医院收治膝骨关节炎患者90例,均行膝关节MRI及胸部QCT检查。根据QTC结果将患者分为3组:骨密度正常组、骨量减少组、骨质疏松组;同时采集他们的性别、年龄、身体质量指数(BMI)、病程等一般信息。按照Recht关节软骨缺损评分系统、全膝关节磁共振成像评分系统(WORMS)评分分别在膝关节MR上评分,同时收集病例骨密度(BMD),将BMD值与MR软骨缺损评分、骨髓水肿评分做统计学分析。结果:3组的性别、BMI、病程无统计学差异,年龄有统计学差异;3组间的软骨缺损评分及骨髓水肿评分均显示骨量正常组与骨量减少组、骨量正常组与骨质疏松组有统计学意义,骨量减少组与骨质疏松组无统计学意义;KOA软骨损伤与骨密度相关,相关系数r=-0.412;KOA骨髓水肿与骨密度相关,相关系数r=-0.254。结论:KOA患者的全身骨密度值与膝关节软骨损伤、骨髓水肿相关,且全身骨密度减少时,可能提示膝关节软骨损伤程度加重或骨髓水肿程度加重。
Abstract:Objective: To determine the relationship between cartilage injury, bone marrow edema, and total bone mineral density in patients with knee osteoarthritis (KOA). Methods: Ninety patients with KOA admitted to the Sichuan Province Orthopedic Hospital between March 2023 and October 2023 were selected, all of whom underwent knee joint MRI and chest QCT examinations. The patients were divided into three groups according to the QTC results: normal bone density, reduced bone mass, and osteoporosis. Patient information, such as sex, age, body mass index (BMI), and course of illness, was also obtained. MRIs of the knee joints were scored separately according to the Recht grading and Whole-organ Magnetic Resonance Imaging Score (WORMS). The bone mineral density (BMD) of the patients was calculated and the BMD values were statistically analyzed using the MR score. Results: No statistically significant differences were observed in sex, BMI, or disease duration among the three groups; however, a statistically significant difference was observed in age. The Recht and WORMS scores among the three groups showed statistical significance between the normal bone density group and the reduced bone mass and osteoporosis groups; however, no statistical significance was observed between the reduced bone mass and osteoporosis groups. KOA cartilage injury was negatively correlated with bone density with a correlation coefficient of r=−0.412, while KOA bone marrow edema was negatively correlated with bone density with a correlation coefficient of r=−0.254. Conclusion: The total bone density in patients with KOA is related to knee joint cartilage injury and bone marrow edema. A decrease in total bone density may indicate the severity of knee cartilage injury or bone marrow edema.
-
Keywords:
- knee osteoarthritis /
- bone mineral density /
- cartilage injury /
- bone marrow edema /
- osteoporosis
-
皮肌炎(dermatomyositis,DM)和多发性肌炎(polymyositis,PM)是一组以侵犯横纹肌为主的系统性自身免疫性疾病,其特征性表现为对称性四肢近端肌无力。该病的具体病因及发病机制尚未明确,除肌肉和皮肤受累外,还可累及心、肺、关节等全身多脏器与系统,其中肺部受累主要表现为间质性肺疾病(interstitial lung disease,ILD),是DM/PM常见且严重的并发症[1-2]。
文献报道DM/PM相关间质性肺病(DM/PM-ILD)的发病率高达19.9%~78%,且部分患者可以肺部表现为首发症状,DM/PM-ILD对疾病的预后有着重要的影响,同时也是导致患者死亡的重要原因之一[1-4]。ILD是一组导致肺实质炎症或纤维化的疾病[5],高分辨率CT(high-resolution computed tomography,HRCT)具有良好的空间分辨率,能够清晰显示弥漫性肺间质异常的形态学特征,在ILD的诊断中具有十分重要的价值。
本研究旨在探讨DM/PM-ILD的HRCT特征,以期提高对该病的早期识别和及时诊治。
1. 资料与方法
1.1 一般资料
回顾性纳入2014年1月至2019年12月在西安交通大学第一附属医院确诊,且临床与HRCT资料完整的DM/PM-ILD患者。
纳入标准:①年龄>18岁;②DM/PM诊断依据Bohan等[6]1975年提出的分类标准诊断;③间质性肺病及相关影像分型的诊断参考 2013美国胸科学会/欧洲呼吸协会制定的特发性间质性肺炎分类标准[7]。排除标准:①重叠性肌炎;②合并肿瘤;③合并有其他可能引起肺间质性病变的疾病;④具有环境和职业暴露史;⑤合并心、肾疾病。
本研究经西安交通大学第一附属医院医学伦理委员会批准(批件号:KYLLSL201312202),并免去患者签署知情同意书。
1.2 CT检查方法
CT扫描采用64层及以上CT扫描仪,患者均取仰卧位,于最大吸气末屏气扫描,扫描范围包括肺尖至肺底。扫描参数:管电压120 kV,自动管电流,矩阵512 mm×512 mm(54例)或1 024 mm×1 024 mm(87例),采用骨算法重建图像,重建层厚1 mm、层间距1 mm。
所有图像传输至影像工作站,分别在肺窗(窗宽/窗位=1 500 HU/-600 HU)及纵隔窗(窗宽/窗位=400 HU/50 HU)观察。
1.3 CT图像评估
采集所有患者确诊DM/PM-ILD后首次胸部CT检查,CT图像评估由两名分别具有高年资工作经验的胸部影像医生独立完成,结论有分歧时,经双方讨论达成一致意见。图像评价内容包括:
(1)记录以下基本征象是否存在:磨玻璃影(ground-glass opacity,GGO),实变,小叶间隔增厚,小叶内间质增厚,胸膜下线,牵拉性支气管扩张,蜂窝影;记录伴随征象如胸腔积液、心包积液、纵隔气肿等;征象评估参照Fleischer协会胸部术语[8]。
(2)记录病灶分布位置:在轴向上病灶主体位于肺野内2/3称为中央分布,在肺野外带1/3称为周边分布,其他为弥漫或随机分布;在纵向上:分布定义为上肺野(病灶主体位于气管隆突以上)、下肺野(病灶主体位于气管隆突以下)及弥漫或随机分布。
(3)记录HRCT上间质性肺炎的影像分型,包括:非特异性间质性肺炎(non-specific interstitial pneumonia,NSIP),机化性肺炎(organized pneumonia,OP),NSIP叠加OP(NSIP with OP overlap,NSIP+OP),弥漫性肺泡损伤(diffuse alveolar damage,DAD)以及普通型间质性肺炎(usual interstitial pneumonia,UIP)或可能普通型间质性肺炎。
2. 结果
2.1 一般情况
本研究共纳入DM/PM-ILD患者141例,平均年龄(52.2±11.5)岁。其中男性32例(22.7%),平均年龄(54.3±11.2)岁;女性109例(77.3%),平均年龄(51.6±11.6)岁。
141例患者中,DM患者114例(80.9%),PM患者27例(19.1%)。
2.2 胸部HRCT表现
2.2.1 影像征象
141例DM/PM-ILD患者影像表现见表1,磨玻璃影123例(87.2%)、小叶间隔增厚110例(78.0%)、小叶内间质增厚90例(63.8%)、实变41例(29.1%)、胸膜下线37例(26.2%)、牵拉性支气管扩张28例(19.9%)、蜂窝征5例(3.5%)。
表 1 DM/PM-ILD患者HRCT基本特征Table 1. The basic HRCT features of DM/PM-ILD patients项目 HRCT特征 例数 占比/% 总例数 141 100.0 基本特征 GGO 123 87.2 实变 41 29.1 小叶间隔增厚 110 78.0 小叶内间质增厚 90 63.8 胸膜下线 37 26.2 牵拉性支气管扩张 28 19.9 蜂窝影 5 3.5 伴随征象 纵隔气肿 3 2.1 胸腔积液 15 10.6 心包积液 18 12.8 病灶轴向分布 中央分布 0 0.0 周围分布 108 76.6 弥漫或随机分布 33 23.4 病灶纵向分布 上肺 0 0.0 下肺 52 36.9 弥漫或随机分布 89 63.1 所有患者均表现为两肺同时受累,病灶在纵向上主要分布在两肺下野(52例,36.9%)或呈弥漫分布(89例,63.1%),两肺上野鲜有受累;在轴向分布上,病灶呈明显的周边分布趋势(108例,76.6%),其次呈弥漫分布(33例,23.4%)。
2.2.2 影像分型
141例DM/PM-ILD患者影像分型见表2。表现为NSIP型者最多见,共53例(37.6%),其次为OP型,共39例(27.7%),NSIP叠加OP型共32例(22.7%),UIP/可能UIP共9例(6.4%),DAD 8例(5.7%),最为少见。典型病例见图1所示。
表 2 DM/PM-ILD患者HRCT影像分型Table 2. The radiological pattern of DM/PM-ILD patients on HRCT影像分型 例数 占比/% 总例数 141 100.0 NSIP 53 37.6 OP 39 27.7 NSIP+OP 32 22.7 DAD 8 5.7 UIP/可能UIP 5/4 3.5/2.8 ![]() 图 1 皮肌炎/多发性肌炎相关间质性肺病(DM/PM-ILD)患者代表性胸部HRCT表现Figure 1. Representative HRCT images of DM/PM-ILD patients
图 1 皮肌炎/多发性肌炎相关间质性肺病(DM/PM-ILD)患者代表性胸部HRCT表现Figure 1. Representative HRCT images of DM/PM-ILD patients3. 结论
本研究发现DM/PM-ILD在HRCT上的表现主要以GGO,小叶间隔增厚,小叶内间质增厚为主,实变、胸膜下线、牵拉性支气管扩张次之,蜂窝较为少见。病变在分布上主要以两肺下野、肺野外周带分布为主,主要的影像分型表现为NSIP、OP以及NSIP叠加OP型。
在以间质受累为主的疾病中,磨玻璃影是间质纤维化形成肺泡炎的过程,其病理基础为间质性肺泡壁炎,即肺泡间隔有不同程度的炎细胞浸润,肺泡腔内有蛋白性物质和细胞增生,肺泡间隔内有网状蛋白增生,但基本没有胶原组织形成间质纤维化,肺泡组织结构保持完整[8-9]。本组病例中,两肺下叶周边分布的GGO是DM/PM-ILD患者最常见表现,141例患者中有123例(87.2%)患者出现磨玻璃影,与Egashira等[10]报道的一致。在没有牵拉性支扩的情况下,磨玻璃影是肺泡纤维化的可靠征象,而磨玻璃影不仅仅是纤维化在影像上的早期的表现,这一征象也往往提示疾病的活动期,此时积极的治疗可能有效[11-12]。
小叶间隔为肺脏表面的间质伸入肺内将肺组织分隔成次级肺小叶的纤维结缔组织,内含肺静脉和肺淋巴管。小叶内间质主要是指肺泡间隔内的细纤维网;小叶内间质增厚与小叶间隔增厚的病理改变主要是由于液体、纤维组织、细胞或其他物质在肺间质内浸润所致,HRCT上多表现为网影及细网影。小叶间隔增厚与小叶内间质增厚常见于ILD的早期改变中,本研究中小叶间隔增厚与小叶内间质增厚为DM/PM-ILD的第二大常见征象,分别为78.0% 和63.8%。当小叶内间质增厚合并牵拉性支扩或蜂窝时,肺间质纤维化程度一般会进行性加重,小叶内间质增厚合并不规则小叶间隔增厚时,小叶内间质增厚可以部分吸收或残留[9]。
肺纤维化是间质性肺病的重要结局事件,CT上可出现肺结构扭曲,如肺体积减小、牵拉性支气管扩张和蜂窝征[13-14],牵拉性支气管扩张通常是由于肺纤维化牵拉支气管导致支气管不规则扩张。本组病例共有28例患者出现牵拉性支扩征象,其中有5例患者合并出现蜂窝征象,提示DM/PM-ILD出现纤维化几率较低,且主要表现为牵拉性支气管扩张,这与Palmucci等[2]和Hayashi等[15]的研究结果一致。Hayashi等[15]根据HRCT结果将DM-ILD患者分为3组:A组,实变为主型;B组,磨玻璃影/网格影为主型,不伴有慢性纤维化;C组,磨玻璃影/网格影为主伴有慢性肺纤维化组。3组发生致死性疾病的概率分别为0%、83%和20%。由此可见,当DM-ILD患者肺部出现以磨玻璃影或网格影为主要表现但不伴有慢性纤维化时应当积极治疗。
有关纵隔气肿发生的机制尚不明确,Singh等[16]认为可能是肺泡过度充气致肺泡破裂,气体溢出至周围的支气管血管间隙,后经肺间质播散到纵隔,空气可从纵隔进入颈部、面部、腹部和四肢,导致皮下气肿。既往文献报道纵隔气肿是DM/PM-ILD罕见但严重的并发症,与不良预后高度相关[17-18],本研究共3例患者合并纵隔气肿,均发生在DM-ILD患者中,发生率为2.1%,与既往文献报道一致,HRCT上表现为纵隔内多发散在气体影,其与DM/PM-ILD患者的预后相关性有待进一步大数据的验证。
ILD组织学分型[7,19]包括普通型间质性肺炎(UIP)、非特异进性间质性肺炎(NSIP)、机化性肺炎(OP)、弥漫性肺泡损伤(DAD)、呼吸性细支气管炎(RB)、脱屑间质性肺炎(DIP)和淋巴细胞间质性肺炎(LIP)。由于临床实践中仅少数患者可经病理活检证实,因此基于HRCT征象的影像分型广泛应用于ILD疾病诊疗随访中。既往文献中报道DM/PM-ILD最常见影像模式依次为NSIP、OP,UIP相对较少,少部分患者还可以表现为DAD[19-21]。本研究发现109(77.3%)例患者影像学表现为单一模式,以NSIP(37.6%)与OP(27.7%)最常见,UIP相对少见(9例)。32例(22.7%)患者可见多模式并存,表现为NSIP叠加OP。NSIP叠加OP模式通常预示肺部病变炎症居多、纤维化较少,一般而言对治疗反应良好。此外,少部分患者可表现为DAD,通常预示着呼吸窘迫综合征(ARDS)可能及患者预后不良。
本研究具有一定的局限性。①本研究为回顾性、单中心研究,样本量有限,难以避免选择偏倚;②本研究探讨了DM/PM-ILD的基本影像特征及其影像表现模式,未能进一步探讨在疾病发展过程中,影像征象及其模式的动态演变;③DM/PM是一组异质性非常强的自身免疫性疾病,患者可表达不同的自身抗体,不同抗体的DM/PM患者在ILD的影像表现上是否有所不同,有待进一步的探究。
总而言之,DM/PM-ILD的HRCT表现具有一定的特征性,影像征象以磨玻璃影、小叶间隔增厚及小叶内间质增厚为主,病灶主要分布两肺下野及肺野外周带,NSIP、OP、NSIP+OP是最常见的3种影像分型。在实际临床实践中当遇到征象、分布不符合或者不典型的患者,需要综合临床、实验室各项指标考虑是否合并感染;而当影像模式为DAD的患者,则需及早提示临床警惕ARDS的发生,酌情采取更加激进的治疗方法以挽救患者生命。
-
![]()
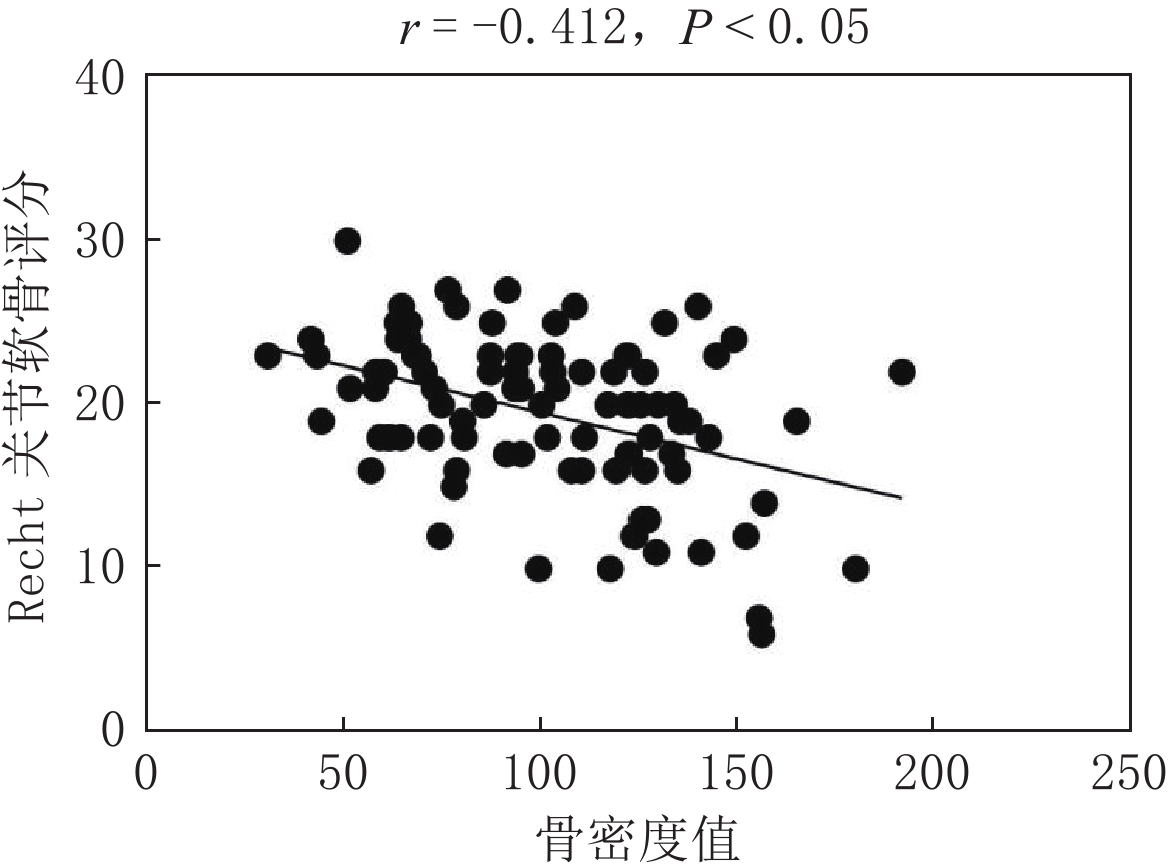
图 1 Recht关节软骨评分与QCT骨密度值的相关性
Figure 1. Correlation between the Recht score and QCT bone mineral density
![]()
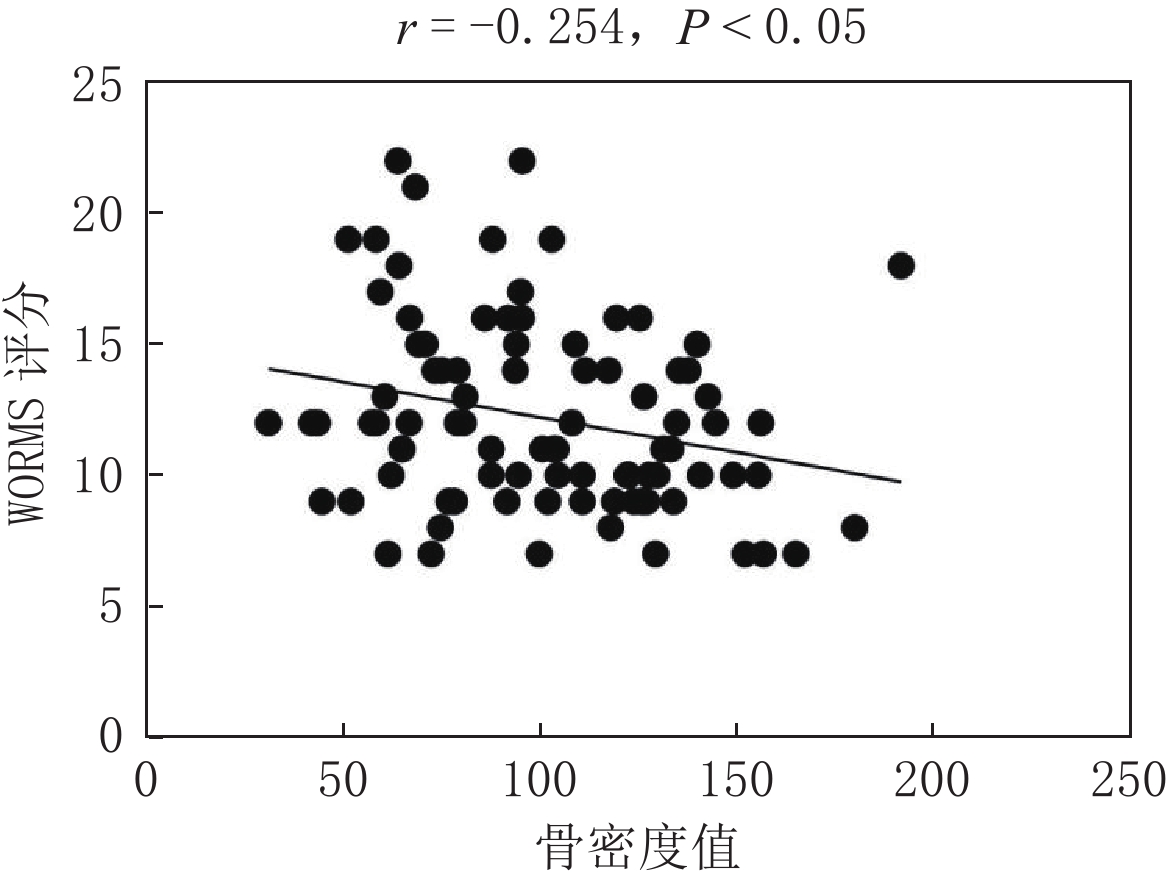
图 2 WORMS骨髓水肿评分与QCT骨密度值的相关性
Figure 2. Correlation between WORMS and QCT bone mineral density
![]()
图 3 三组患者膝关节核磁共振成像
注:(a)骨密度正常组,左膝关节软骨完整,无骨髓水肿; (b)骨量减少组,左膝关节股骨内侧髁、胫骨平台内侧软骨损伤、骨髓水肿; (c)骨质疏松组,右膝关节股骨内侧髁、胫骨平台内侧、胫骨平台外侧软骨损伤、骨髓水肿。
Figure 3. MRI of the knee joint of patients in the three groups
表 1 三组骨关节炎患者一般资料比较
Table 1 Comparison of the general data of patients with osteoarthritis in the three groups
组别 年龄$ \left(\overline{x}\pm s\right) $/岁 性别/例 BMI$ \left(\overline{x}\pm s\right) $/kg·m-2 病程$ \left(\overline{x}\pm s\right) $/月 男 女 骨量正常组(n=30) 55.03±7.42 7 23 26.20±3.68 44.23±71.20 骨量减少组(n=30) 62.30±10.11 8 22 26.03±3.92 61.47±72.39 骨质疏松组(n=30) 68.80±6.69 3 27 25.65±3.29 50.83±55.45 检验值 F=21.139 $\chi^2 $=2.917 F=0.184 F=0.508 P 0.000 0.233 0.832 0.603  下载: 导出CSV
下载: 导出CSV
表 2 三组骨关节炎患者软骨评分比较
Table 2 Comparison of the cartilage scores of patients with osteoarthritis in the three groups
组别 项目 统计检验 骨量正常组(n=30) 骨量减少组(n=30) 骨质疏松组(n=30) F P 得分$ \left(\overline{x}\pm s\right) $ 17.10±5.25 20.10±4.04 21.33±3.98 7.143 0.01
下载: 导出CSV
表 3 三组骨关节炎患者骨髓水肿评分比较
Table 3 Comparison of the bone marrow edema scores of patients with osteoarthritis in the three groups
项目 组别 统计检验 骨量正常组(n=30) 骨量减少组(n=30) 骨质疏松组(n=30) F P 得分$ \left(\overline{x}\pm s\right) $ 10.73±2.74 12.83±3.67 13.03±3.99 3.941 0.023
下载: 导出CSV
-
[1] 王斌, 邢丹, 董圣杰, 等. 中国膝骨关节炎流行病学和疾病负担的系统评价[J]. 中国循证医学杂志, 2018, 18(2): 134−142. WANG B, XING D, DONG S J, et al. Prevalence and disease burden of knee osteoarthritis in China: A systematic review[J]. Chinese Journal of Evidence-based Medicine, 2018, 18(2): 134−142. (in Chinese).
[2] HARRELL C R, MARKOVIC B S, FELLABAUM C, et al. Mesenchymal stem cell-based therapy of osteoarthritis: Current knowledge and future perspectives[J]. Biomedicine Pharmacotherapy, 2019, 109: 2318−2326. DOI: 10.1016/j.biopha.2018.11.099.
[3] MESSENT E A, WARD R J, TONKIN C J, et al. Differences in trabecular structure between knees with and without osteoarthritis quantified by macro and standard radiography, respectively[J]. Osteoarthritis Cartilage, 2006, 14(12): 1302−1305. DOI: 10.1016/j.joca.2006.07.012.
[4] BUCKLAND-WRIGHT C. Subchondral bone changes in hand and knee osteoarthritis detected by radiography[J]. Osteoarthritis Cartilage, 2004, 12(S)A: S10-S19.
[5] DEDRICK D K, GOLDSTEIN S A, BRANDT K D, et al. A longitudinal study of subchondral plate and trabecular bone in cruciate-deficient dogs with osteoarthritis followed up for 54 months[J]. Arthritis Rheumatic, 1993, 36(10): 1460−1467. DOI: 10.1002/art.1780361019.
[6] 张程, 吴忠书, 李子祺, 等. 膝骨关节炎与骨质疏松症的相关性研究进展[J]. 中国骨质疏松杂志, 2021, 27(4): 618−624. DOI: 10.3969/j.issn.1006-7108.2021.04.028. ZHANG C, WU Z S, LI Z Q, et al. Research progress on the correlation between knee osteoarthritis and osteoporosis[J]. Chinese Journal of Osteoporosis, 2021, 27(4): 618−624. DOI: 10.3969/j.issn.1006-7108.2021.04.028. (in Chinese).
[7] BENNELL K L, CREABY M W, WRIGLEY T V, et al. Bone marrow lesions are related to dynamic knee loading in medial knee osteoarthritis[J]. Annals of the Rheumatic Diseases, 2010, 69(6): 1151−1154. DOI: 10.1136/ard.2009.118182.
[8] 王勇朋, 阳琰, 何生生, 等. 低剂量胸部CT与QCT椎体骨密度测量一站式扫描可行性研究[J]. 放射学实践, 2018, 33(11): 1194−1197. WANG Y P, YANG Y, HE S S, et al. Low-dose chest CT and QCT “one-stop-shop” scan technology: A feasibility study[J]. Radiologic Practice, 2018, 33(11): 1194−1197. (in Chinese).
[9] 中华医学会骨科学分会关节外科学组. 骨关节炎诊疗指南(2018年版)[J]. 中华骨科杂志, 2018, 38(12): 705−715. DOI: 10.3760/cma.j.issn.0253-2352.2018.12.001. Osteoporosis Group of Chinese Orthopaedic Associationg. Chinese guideline for diagnosis and management of osteoarthritis (2018 edition)[J]. Chinese Journal of Orthopaedics, 2018, 38(12): 705−715. DOI: 10.3760/cma.j.issn.0253-2352.2018.12.001. (in Chinese).
[10] RECHT M P, KRAMER J, MARCELIS S, et al. Abnormalities of articular cartilage in the knee: Analysis of available MR techniques[J]. Radiology, 1993, 187(2): 473−478. DOI: 10.1148/radiology.187.2.8475293.
[11] PETERFY C G, GUERMAZI A, ZAIM S, et al. Whole-organ magnetic resonance imaging score (WORMS) of the knee in osteoarthritis[J]. Osteoarthritis Cartilage, 2004, 12(3): 177−190. DOI: 10.1016/j.joca.2003.11.003.
[12] 李凯, 陈捷, 赵林芬, 等. 中国人群定量CT(QCT)脊柱骨密度正常参考值的建立和骨质疏松症QCT诊断标准的验证[J]. 中国骨质疏松杂志, 2019, 25(9): 1257−1262. DOI: 10.3969/j.issn.1006-7108.2019.09.011. LI K, CHEN J, ZHAO L F, et al. The establishment of QCT spinal vBMD re ference database and the validation of the diagnosis criteria of oste oporosis with QCT for Chinese[J]. Chinese Journal of Osteoporosis, 2019, 25(9): 1257−1262. DOI: 10.3969/j.issn.1006-7108.2019.09.011. (in Chinese).
[13] 舒意, 杨沛, 廖紫祾, 等. 一站式低剂量扫描在胸部及腰椎QCT体检人群中的应用[J]. CT理论与应用研究, 2022, 31(2): 244−250. DOI: 10.15953/j.1004-4140.2022.31.02.12. SHU Y, YANG P, LIAO Z L, et al. To explore the low-dose CT and QCT “one-stop-shop” scan technology for physical examination crowd[J]. CT Theory and Applications, 2022, 31(2): 244−250. DOI: 10.15953/j.1004-4140.2022.31.02.12. (in Chinese).
[14] 赵敏, 刘鸿雁, 王国华, 等. 膝关节骨关节炎半月板损伤程度与关节软骨T1 rho、T2 mapping相关性研究[J]. 中国临床医学影像杂志, 2019, 30(11): 812−816. ZHAO M, LIU H Y, WANG G H, et al. The correlation between the degree of meniscus injury of knee osteoarthritis and T1 rho, T2 mapping of the articular cartilage[J]. Journal of China Clinic Medical Imaging, 2019, 30(11): 812−816. (in Chinese).
[15] 王佳, 朱吉云, 茅博伟, 等. 膝关节骨性关节炎软骨损伤的MRI形态评分及T2值变化与临床表现的相关性[J]. 影像研究与医学应用, 2021, 5(21): 26−27. DOI: 10.3969/j.issn.2096-3807.2021.21.012. WANG J, ZHU J Y, MAO B W, et al. MRI morphological scores of cartilage injury in knee joint osteoarthritis and correlation between changes of T2 value and clinical features[J]. Journal of Imaging Research and Medical, 2021, 5(21): 26−27. DOI: 10.3969/j.issn.2096-3807.2021.21.012. (in Chinese).
[16] 刘艳平, 廖忠剑, 李正南. 磁共振成像检查在评估膝关节退行性骨关节炎患者关节损伤程度中的价值[J]. 中国当代医药, 2021, 28(34): 158−161. DOI: 10.3969/j.issn.1674-4721.2021.34.043. LIU Y P, LIAO Z J, LI Z N. The value of magnetic resonance imaging in assessing the degree of joint damage in patients with knee degenerative osteoarthritis[J]. China Modern Medicine, 2021, 28(34): 158−161. DOI: 10.3969/j.issn.1674-4721.2021.34.043. (in Chinese).
[17] 韩雪莉. 迭代模型重建技术在低剂量胸部CT联合腰椎QCT扫描中的研究[D]. 郑州: 郑州大学, 2018. HAN X L. The study of iterative model reconstruction technique on the low dose chest CT combined with lumbar vertebrae quantitative CT[D]. Zhengzhou: Zhengzhou University, 2018. (in Chinese).
[18] LEE J Y, HARVEY W F, PRICE L L, et al. Relationship of bone mineral density to progression of knee osteoarthritis[J]. Arthritis Rheumatic, 2013, 65(6): 1541−1546. DOI: 10.1002/art.37926.
[19] BOBINAC D, SPANJOL J, ZORICIC S, et al. Changes in articular cartilage and subchondral bone histomorphometry in osteoarthritic knee joints in humans[J]. Bone, 2003, 32(3): 284−290. DOI: 10.1016/S8756-3282(02)00982-1.
[20] KAMIBAYASHI L, WYSS U P, COOKE T D, et al. Trabecular microstructure in the medial condyle of the proximal tibia of patients with knee osteoarthritis[J]. Bone, 1995, 17(1): 27−35. DOI: 10.1016/8756-3282(95)00137-3.
[21] LI B, ASPDEN R M. Composition and mechanical properties of cancellous bone from the femoral head of patients with osteoporosis or osteoarthritis[J]. Journal of Bone and Mineral Research, 1997, 12(4): 641−651. DOI: 10.1359/jbmr.1997.12.4.641.
[22] TOKGÖZ M A, ATIK O Ş, ESENDAĞLI G, et al. Is it possible that the pathogenesis of osteoarthritis could start with subchondral trabecular bone loss like osteoporosis?[J]. Eklem Hastalik Cerrahisi, 2018, 29(3): 152−158. DOI: 10.5606/ehc.2018.007.
[23] MARCUCCI G, BRANDI M L. Rare causes of osteoporosis[J]. Clinical Cases in Mineral and Bone Metabolism, 2015, 12(2): 151−156.
[24] RYD L, BRITTBERG M, ERIKSSON K, et al. Pre-osteoarthritis: Definition and diagnosis of an elusive clinical entity[J]. Cartilage, 2015, 6(3): 156−165. DOI: 10.1177/1947603515586048.
[25] WEN L, SHIN M H, KANG J H, et al. The relationships between bone mineral density and radiographic features of hand or knee osteoarthritis in older adults: Data from the Dong-gu study[J]. Rheumatology (Oxford), 2016, 55(3): 495−503.
[26] ROEMER F W, NEOGI T, NEVITT M C, et al. Subchondral bone marrow lesions are highly associated with, and predict subchondral bone attrition longitudinally: The MOST study[J]. Osteoarthritis Cartilage, 2010, 18(1): 47−53. DOI: 10.1016/j.joca.2009.08.018.
[27] DORE D, MARTENS A, QUINN S, et al. Bone marrow lesions predict site-specific cartilage defect development and volume loss: A prospective study in older adults[J]. Arthritis Research Therapy, 2010, 12(6): R222. DOI: 10.1186/ar3209.
[28] de SÁ G A, DOS S A, NOGUEIRA J M, et al. Angiotensin II triggers knee joint lesions in experimental osteoarthritis[J]. Bone, 2021, 145: 115842. DOI: 10.1016/j.bone.2021.115842.
[29] HEILMEIER U, WAMBA J M, JOSEPH G B, et al. Baseline knee joint effusion and medial femoral bone marrow edema, in addition to MRI-based T2 relaxation time and texture measurements of knee cartilage, can help predict incident total knee arthroplasty 4~7 years later: Data from the Osteoarthritis Initiative[J]. Skeletal Radiology, 2019, 48(1): 89−101. DOI: 10.1007/s00256-018-2995-4.
[30] 曾国庆, 董铿, 黄建军. 膝骨关节炎与骨质疏松症的相关性分析[J]. 中国卫生标准管理, 2023, 14(18): 94−97. DOI: 10.3969/j.issn.1674-9316.2023.18.022. ZENG G Q, DONG K, HUANG J J. Analysis of the correlation between knee osteoarthritis and osteoporosis[J]. China Health Standard Management, 2023, 14(18): 94−97. DOI: 10.3969/j.issn.1674-9316.2023.18.022. (in Chinese).
[31] 周自明, 常时新, 田芳, 等. 膝骨关节炎软骨下骨髓水肿样及囊样病变与软骨病损的相关性研究[J]. 中国医学计算机成像杂志, 2012, 18(3): 243−248. DOI: 10.3969/j.issn.1006-5741.2012.03.012. ZHOU Z M, CHANG S X, TIAN F, et al. Relationship between subchondral bone marrow edema-like or cyst-like lesions and cartilage loss in patients with knee osteoarthritis[J]. Chinese Computed Medical Imaging, 2012, 18(3): 243−248. DOI: 10.3969/j.issn.1006-5741.2012.03.012. (in Chinese).
[32] 何勇, 张乾, 高华利, 等. 类风湿关节炎膝关节骨髓水肿病变的影像学研究[J]. 中国矫形外科杂志, 2019, 27(5): 421−425. HE Y, ZHANG Q, GAO H L, et al. Bone marrow edema in rheumatoid arthritis knee: A study based on MRI[J]. Orthopedic Journal of China, 2019, 27(5): 421−425. (in Chinese).
[33] 肖龙文, 桑志成. 重度膝骨关节炎患者骨髓水肿与骨质疏松的相关性研究[J]. 中国骨伤, 2023, 36(4): 371−375. XIAO L W, SANG Z C. Study on correlation between bone marrow edema and osteoporosis in patients with severe knee osteoarthritis[J]. China Journal of Orthopaedics and Traumatology, 2023, 36(4): 371−375. (in Chinese).
[34] 郭子瑊, 毛兴佳, 高英杰, 等. 膝骨关节炎与膝关节周围骨密度的相关性研究进展[J]. 中华关节外科杂志(电子版), 2021, 15(5): 586−595. GUO Z J, MAO X J, GAO Y J, et al. Research progress on relationship between knee osteoarthritis and bone mineral density around knee joint[J]. Chinese Journal of Joint Surgery (Electronic Edition), 2021, 15(5): 586−595. (in Chinese).
[35] 程晓光, 王亮, 曾强, 等. 中国定量CT(QCT)骨质疏松症诊断指南(2018)[J]. 中国骨质疏松杂志, 2019, 25(6): 733−737. CHENG X G, WANG L, ZENG Q, et al. The China guideline for the diagnosis criteria of osteoporosis with quantitative computed tomography (QCT) (2018)[J]. Chinese Journal of Osteoporosis, 2019, 25(6): 733−737. (in Chinese).
[36] ENGELKE K, ADAMS J E, ARMBRECHT G, et al. Clinical use of quantitative computed tomography and peripheral quantitative computed tomography in the management of osteoporosis in adults: The 2007 ISCD official positions[J]. Journal of Clinical Densitometry, 2008, 11(1): 123−162. DOI: 10.1016/j.jocd.2007.12.010.


计量
- 文章访问数: 209
- HTML全文浏览量: 38
- PDF下载量: 23


