
Applicability of Different Iterative Reconstruction Algorithms in Orbital Computed Tomography
-
摘要:
目的:探讨不同迭代重建算法在眼眶CT中的应用价值。方法:回顾性收集2024年1月至2024年3月首都医科大学附属北京同仁医院行眼眶CT检查的31例患者,分别使用混合迭代重建算法(iDose4)和全模型迭代重建算法(IMR)技术对图像进行标准算法和骨算法重建,对比分析不同重建算法图像的平均CT值、噪声(SD)、信噪比(SNR)、对比度噪声比(CNR)以及图像质量主观评分;采用随机区组方差分析比较不同算法重建图像间的客观指标差异;采用多个相关样本的秩和检验比较不同算法重建图像的主观评分差异。结果:不同标准算法重建图像的CT值、噪声、SNR、CNR差异均有统计学意义,与iDose4相比,IMR标准算法重建图像噪声降幅达25%~67%,SNR增加1.3~1.5倍,CNR增加2~3倍;与iDose4相比,IMR骨算法重建图像噪声降幅达70%~96%,SNR增加5~15倍,CNR增加4~31倍;不同骨算法及标准算法的图像质量评分差异均有统计学意义,标准算法IMR1-Brain Routine组评分最高5(4,5),骨算法iDose43 YD组评分最高5(5,5);两名观察者评分的一致性较强,加权Kappa系数0.644~1。结论:眼眶CT中推荐使用混合迭代重建技术iDose4 Level 3重建骨算法图像,使用全模型迭代重建技术IMR Level1重建标准算法图像。
Abstract:Objective: This study aimed to investigate the value of different iterative reconstruction algorithms for orbital computed tomography (CT). Methods: Orbital CT data from 31 patients were retrospectively collected from January to March 2024 at Beijing Tongren Hospital Capital Medical University. The images were reconstructed using both the Hybrid Iterative Reconstruction Algorithm (iDose4) and Iterative Model Reconstruction (IMR) techniques for the bone and standard algorithms. The average CT number, standard deviation (SD) of noise , signal-to-noise ratio (SNR), contrast-to-noise ratio (CNR), and image quality scores of different reconstruction algorithms were compared. Randomized block variance analysis was used to compare differences in objective indicators, and the Wilcoxon signed-rank test for related samples was used to compare differences in subjective scores. Results: The differences in the CT number, noise, SNR, and CNR of images reconstructed using different standard algorithms were statistically significant. Compared with iDose4, the noise reduction of the IMR standard algorithm-reconstructed images ranged from 25% to 67%, with an SNR increase of 1.3~1.5 times, and a CNR increase of 2 to 3 times. Compared with iDose4, the noise reduction of the IMR bone algorithm-reconstructed images ranged from 70% to 96%, with an SNR increase of 5~15 times and a CNR increase of 4~31 times. The differences in the image quality scores of the images reconstructed using different bone and standard algorithms were statistically significant. The highest scores were 5 (5, 5) for the iDose4 Level 3 Y-Detail (YD) bone algorithm group and 5 (4, 5) for the IMR Level 1 Brain Routine standard algorithm group. The consistency of the scores evaluated by the two observers was strong, with weighted kappa coefficients ranging from 0.644 to 1. Conclusion: In orbital CT, we recommend using a hybrid iterative reconstruction technique (iDose4 Level 3) to reconstruct bone algorithm images and the iterative model reconstruction technique (IMR-Level 1) to reconstruct standard algorithm images.
-
Keywords:
- tomography /
- X-ray computed /
- iterative model reconstruction (IMR) /
- orbital /
- noise
-
滤泡性淋巴瘤(follicular lymphoma,FL)是非霍奇金淋巴瘤(non-Hodgkin’s lymphoma,NHL)的常见类型之一,多发生于淋巴结,也可见于胃肠道、皮肤等结外器官或部位,罕见发生于骨骼肌。结外病灶的诊断对评估FL患者预后具有重要价值。能谱增强CT成像能够通过分析不同组织的能谱曲线确定其同质性,因此能帮助诊断继发性结外淋巴瘤。
本文报告我院收治的1例以能谱增强CT扫描诊断骨骼肌继发性结外FL的病例。
1. 病历资料
1.1 临床病史及诊疗经过
患者,男,52岁,因发现左侧腹股沟区一枚硬币大小的肿物2月余于2021年9月于外院就诊。2021年9月6日行腹股沟彩超检查示双侧腹股沟淋巴结肿大,行穿刺活检术,10月11日病理报告示倾向为低级别滤泡性淋巴瘤。同时患者自觉消瘦明显,1月内体重下降5 kg,伴夜间出汗明显,肢软乏力。
于10月13日行正电子发射计算机断层显像(position emission tomography,PET)/计算机断层扫描(computed tomography,CT)检查发现:①全身多区域淋巴结肿大、脾肿大伴氟代脱氧葡萄糖(fluoro deoxy glucose,FDG)代谢增高,全身多发骨骼FDG代谢增高,均考虑淋巴瘤累及;②肝肿大,肝内稍低密度灶伴边缘FDG代谢轻度增高,淋巴瘤累及不除外。
10月18日患者于外院住院治疗,并于全麻下行功能性颈部淋巴结清除术,术后予谷胱甘肽、兰索拉唑、盐酸左西替利嗪、氟比洛芬酯综合治疗。术后病理免疫组化:CD3(背景T细胞+),CD20(+),CD19(+),CD10(+),cD21(树突细胞+),CD23(树突细胞+),CD5(背景T细胞+),CyclinD1( − ),Bc12(生发中心41),Bc16(生发中心+),Ki67(生发中心15%),PD-1(散在+),结合苏木精-伊红染色法(hematoxylin-eosin stain, HE stain)可符合为滤泡性淋巴瘤I级。
2021年11月9日,患者因肢麻乏力于我院住院治疗,行上、下腹部CT平扫示:右侧心膈角、肝门区、腹膜后、腹腔、盆壁多发肿大淋巴结,部分融合;脾脏肿大(图1)。行骨髓穿刺+活检示:骨髓增生极度活跃,骨小梁20%,纤维脂肪5%,造血主质75%,三系均见,以中晚幼成熟为主,B淋巴细胞相对明显增生,呈实性、滤泡状生长,表达BCL-2,全片见巨核细胞10个,网状纤维重度增生(MF-3),结合临床所供病史及实验室检查,倾向滤泡性淋巴瘤累及骨髓。
![]() 图 1 上腹部CT平扫:双侧腰大肌形态、密度无明显差异;腹膜后多发肿大淋巴结;脾肿大Figure 1. Computed tomography (CT) scan of the upper abdomen
图 1 上腹部CT平扫:双侧腰大肌形态、密度无明显差异;腹膜后多发肿大淋巴结;脾肿大Figure 1. Computed tomography (CT) scan of the upper abdomen患者临床诊断为滤泡性淋巴瘤Ann Arbor IV期,FL国际预后指数(FL international prognosticindex,FLIPI)3分(高危)。目前IV期FL普遍认为不可治愈,且FL为惰性淋巴瘤,大部分患者病变进展缓慢,相当长时间不接受治疗仍可保持良好的生活质量,故该患者未行放、化疗治疗,在患者要求下于我院行中医保守治疗。
2022年4月患者因腰痛进行性加重2月,妨碍行走就诊我院。血液检查结果:血红蛋白106 g/L,白细胞计数2.75×109/L(正常范围3.50~9.50×109/L),血小板178×109/L,乳酸脱氢酶205.8 U/L,尿β2-微球蛋白2.32 mg/L(正常范围 0.00~0.30 mg/L)。乙型和丙型肝炎病毒以及人类免疫缺陷病毒血清学检测呈阴性。
2022年4月19日行腰椎磁共振(magnetic resonance imaging,MRI)平扫(图2),因幽闭恐惧症发作无法耐受长时间扫描,且患者拒绝行PET/CT检查及穿刺活检和手术。为明确诊断和病变范围遂于次日行腰椎能谱增强CT检查。
![]() 图 2 腰椎MRI平扫(a)和(b)L1-L2水平右侧腰大肌见一肿块,呈T1WI低、T2WI稍高信号。Figure 2. Lumbar spine MRI plain scan
图 2 腰椎MRI平扫(a)和(b)L1-L2水平右侧腰大肌见一肿块,呈T1WI低、T2WI稍高信号。Figure 2. Lumbar spine MRI plain scan1.2 腰椎能谱增强CT
1.2.1 仪器与扫描方法
采用256排CT扫描仪(Revolution CT,GE healthcare)行平扫及增强扫描。采用宝石能谱成像(gemstone spectral imaging,GSI)扫描模式,扫描参数如表1所示。所用对比剂为非离子型碘对比剂(博莱科信宜,国药准字H20053385),浓度370 mg/mL,用量1 mL/kg,流率2 mL/s,生理盐水20 mL,流率3 mL/s。数据采集完成后,重建带能谱数据信息(GSI DATA)序列,层厚0.625 mm,并将所有序列传入工作站进行后处理分析。
表 1 能谱增强CT扫描方式及参数Table 1. Spectral computed tomography (CT) scan modes and parameters扫描方式及参数名 具体扫描方式及参数值 扫描方式及参数名 具体扫描方式及参数值 采集体位 仰卧位,头先进 层间距 0.625 mm 扫描方向、范围 自胸椎下缘向下扫描至骶椎 管电压 GSI模式(瞬时切换80 kVp、140 kVp) 探测器宽度 64×0.625 mm 管电流 自动毫安模式(200~650 mA,NI:9) 扫描方法 经验法 矩阵 512×512 层厚 0.625 mm 机架旋转时间 0.6 s/r 1.2.2 图像后处理及数据测量
将重建后的薄层图像传送到 GE AW4.7工作站,利用GSI Volume Viewer软件进行能谱的多参数分析。在动脉晚期,右侧腰大肌病变强化程度最适宜观察,且受到的血管影干扰最小,因此选择此期进行后处理分析。于右侧肿大腰大肌、对侧镜面位置正常腰大肌及腹膜后肿大淋巴结区域选取合适的感兴趣区(region of interest,ROI)。ROI面积应尽量一致,且均不大于50 mm2,应避开坏死、钙化、囊变、血管影及边缘区。
利用能谱曲线工具获取ROI能谱曲线,分别计算动脉期3组能谱曲线斜率K。计算公式:
$K=({\rm{CT}} $ 值40 keV$-\,{\rm{CT}}$ 值XkeV$)/(X-40)$ ,其中X分别为70、100及140 keV。1.2.3 能谱增强CT结果
腹膜后见多发肿大淋巴结,邻近的右侧L1-2水平腰大肌较对侧正常腰大肌增厚。GSI分析:右侧L1-2水平腰大肌能谱曲线走形与腹膜后肿大淋巴结能谱曲线走形接近,与对侧正常形态腰大肌能谱曲线走形差异较大(图3(a))。根据能谱曲线分别计算3条曲线的斜率K:右侧腰大肌KVP40-70=2.38、KVP40-100=1.5及KVP40-140=0.99;左侧腰大肌KVP40-70=1.41、KVP40-100=0.89及KVP40-140=0.6;腹膜后肿大淋巴结KVP40-70=2.76、KVP40-100=1.76及KVP40-140=1.135(表2)。右侧腰大肌的曲线斜率与腹膜后淋巴结斜率接近,与正常腰大肌斜率差异较大,提示右侧腰大肌被淋巴瘤浸润可能性大。
![]() 图 3 腰椎能谱CT增强图像(a)动脉晚期 ROI对应能谱曲线(蓝线代表右侧肿大腰大肌,绿线代表左侧正常腰大肌,紫线代表腹膜后肿大淋巴结)。(b)腰椎 CT平扫:腹膜后多发肿大淋巴结;右侧腰大肌较对侧明显肿胀。(c)和(d)腰椎能谱增强 CT动脉晚期轴位图像:双侧腰大肌及腹膜后肿大淋巴结ROI对应的CT值;右侧肿大腰大肌增强后强化程度略高于左侧正常腰大肌,密度均匀。Figure 3. Lumbar spine spectral computed tomography (CT) image表 2 双侧腰大肌及腹膜后肿大淋巴结的KVP40-70、KVP40-100及KVP40-140Table 2. KVP40-70, KVP40-100 and KVP40-140 of the bilateral psoas major muscle and enlarged retroperitoneal lymph nodes
图 3 腰椎能谱CT增强图像(a)动脉晚期 ROI对应能谱曲线(蓝线代表右侧肿大腰大肌,绿线代表左侧正常腰大肌,紫线代表腹膜后肿大淋巴结)。(b)腰椎 CT平扫:腹膜后多发肿大淋巴结;右侧腰大肌较对侧明显肿胀。(c)和(d)腰椎能谱增强 CT动脉晚期轴位图像:双侧腰大肌及腹膜后肿大淋巴结ROI对应的CT值;右侧肿大腰大肌增强后强化程度略高于左侧正常腰大肌,密度均匀。Figure 3. Lumbar spine spectral computed tomography (CT) image表 2 双侧腰大肌及腹膜后肿大淋巴结的KVP40-70、KVP40-100及KVP40-140Table 2. KVP40-70, KVP40-100 and KVP40-140 of the bilateral psoas major muscle and enlarged retroperitoneal lymph nodes项目 KVP40-70 KVP40-100 KVP40-140 右侧肿大腰大肌 2.38 1.50 0.99 左侧正常腰大肌 1.41 0.89 0.60 后腹膜肿大淋巴结 2.76 1.76 1.14 1.3 后续治疗与随访
考虑到中医保守治疗效果不佳,为进一步治疗,患者目前于外院诊疗,病情稳定。
2. 讨论
FL是NHL中的一种常见类型,是淋巴滤泡生发中心B细胞来源的一种惰性B细胞淋巴增殖性疾病,以弥漫性淋巴结肿大、骨髓受累和脾肿大为特征,常见于中、老年人,女性稍多于男性。WHO统计FL约占NHL的22.1%,但在中国人群中发生率较低,只占NHL的10% 左右。
FL主要累及淋巴结,结外受累较少见。肿瘤区域个数的增加可提高FL患者的FLIPI指数进而增加患者的危险度分级,因此结外淋巴瘤的诊断对评估FL患者的病情及预后具有重要价值。累及骨骼肌的淋巴瘤非常少见,仅占霍奇金淋巴瘤(Hodgkin lymphoma,HL)病例的 0.3%、NHL病例的1.5%[1],多数病理类型为弥漫大B细胞性淋巴瘤(diffuse large B cell lymphoma,DLBCL),而原发性骨骼肌FL的报道极为罕见,且没有关于其发病率的流行病学数据[2]。
2.1 病因及发病机制
骨骼肌淋巴瘤通常通过3种途径发生:①作为一种原发性结外疾病发生;②通过血源性或淋巴途径传播;③通过邻近器官浸润,如骨骼或淋巴结。原发性骨骼肌淋巴瘤发生在腿部损伤后、靠近针注射部位和同性恋男性直肠已有报道[3]。
由于下肢易受损伤,这可能提示原发性骨骼肌淋巴瘤可能和机械刺激有关。继发性骨骼肌淋巴瘤最常见的原因是从邻近淋巴结或其他原发病灶(如骨)扩散或转移而来[1],这与本病例的影像表现相符。
2.2 临床特征
FL临床表现多为受累肌肉出现进行性增大的软组织肿块、肿胀、疼痛、发热、出汗和体重减轻,最常见于下肢,占所有报告病例的50%[3]。本病例在确诊半年余后出现进行性加重的腰痛,严重影响生活质量,影像学检查提示右侧腰大肌新发的软组织肿块。
2.3 骨骼肌淋巴瘤能谱增强CT表现
能谱增强CT已广泛应用于淋巴瘤的诊断中,目前研究多集中于与鼻咽癌、纵膈胸腺瘤、结节病、肠道肿瘤和转移性淋巴结等疾病的鉴别[4-9]。鉴于骨骼肌淋巴瘤发生的罕见性,通过能谱增强CT诊断的经验较缺乏,只在超声、平扫CT、MRI及PET/CT的相关研究中有零星报道[2,10-15]。
CT可通过病灶的形态、大小、边界、密度及强化方式来诊断骨骼肌淋巴瘤,表现为受累肌肉肿胀,边界清晰或不清晰,与正常肌肉相比呈均质的等或高或低密度,增强后病变肌肉呈轻微至明显不同程度的强化。作为混合能量图像,普通CT的CT值不能准确反映病灶实际的CT值大小。能谱增强CT成像通过快速切换能量并进行数据采集,可获得不同组织在40~140 keV各单能量图像下的CT值[16]。通过对比能谱曲线的形态及斜率可确定病灶的来源、鉴别良恶性。
本例患者患有幽闭恐惧症并拒绝再次穿刺、手术及PET/CT检查,遂行能谱增强CT示右侧腰大肌与腹膜后肿大淋巴结能谱曲线走行及形态相近,虽未取得腰大肌病理结果验证,结合既往病史、病理与影像学检查考虑为骨骼肌淋巴瘤浸润的可能性最大。
2.4 治疗及转归
迄今为止,大多数FL患者仍然不可治愈。FL的治疗应充分考虑患者耐受情况、肿瘤负荷及复发风险而采取个体化治疗。目前各指南推荐的一线治疗方案均为CD20单抗+化疗;对于晚期(Ⅲ 期、Ⅳ期)患者根据美国国立综合癌症网络(national comprehensive cancer nelwork,NCCN)指南推荐如果低肿瘤负荷且没有症状,可采取观察和等待策略;若存在肿瘤高负荷表现、肿瘤进展、受累器官功能受损等治疗指征时,建议开始治疗[17]。
本病例为 Ⅳ 期,FLIPI 3分(高危)患者,前期临床症状轻微,要求中医保守治疗;后期出现严重腰痛,考虑淋巴瘤浸润骨骼肌可能大,提示病变进展,遂于外院就诊进一步治疗。
2.5 诊断与鉴别诊断
骨骼肌淋巴瘤的诊断需结合临床病史、实验室检查、影像学检查及病理组织学检查结果。当骨骼肌出现进行性增大的软组织肿块,伴疼痛、发热、短期内消瘦,应怀疑本病,尤其在淋巴瘤患者中,应怀疑继发性骨骼肌淋巴瘤。影像学特征具非特异性,需与其他疾病(如原发性软组织肉瘤、其他原发软组织恶性肿瘤、创伤或肌炎等)鉴别。
(1)软组织肉瘤:包括平滑肌肉瘤、横纹肌肉瘤、脂肪肉瘤、滑膜肉瘤等,表现为受累肌肉的形态和轮廓改变伴不规则软组织肿块,肿块平扫及增强的密度和信号不均匀,实性部分大多强化明显,易出现坏死、液化,瘤周水肿较淋巴瘤明显。
(2)外周型原始神经外胚瘤:与骨骼肌淋巴瘤同属小细胞肿瘤,好发部位相似,但外周型原始神经外胚瘤多见于10~20岁儿童或青少年,临床发病率低,相对罕见,恶性程度高,易复发转移,预后相对较差,对放化疗敏感。在影像学上肿瘤表现为大软组织肿块,浸润性、跨越性、快速生长,血供丰富,明显不均匀强化,其形态较淋巴瘤更不规则,边界更不清楚,囊变坏死更显著,强化更明显且不均匀。
(3)神经纤维瘤病:是一类常染色体显性遗传性疾病,可分为3型:Ⅰ型神经纤维瘤病、Ⅱ型神经纤维瘤病和 Ⅲ 型施万细胞瘤病。此类疾病表型差异性大,以皮肤病变、周围神经系统病变和中枢神经系统肿瘤为主,引起多发的、渐进性的损害。神经纤维瘤多发生于肌间隙,与肌肉分界清,邻近肌肉受压变形但密度、信号大多正常;少部分发生于肌肉内,病灶形态不规则,受累肌肉多失去正常形态,多肌肉受累时,肌间隙模糊。
(4)炎症:起病急,临床症状明显,表现为局部红肿热痛,部分患者全身症状明显,抗炎治疗有效。CT或MRI表现为受累肌肉明显肿胀,肌间隙模糊,筋膜及皮下水肿较明显。
3. 总结
本文报道了1例以能谱增强CT成像帮助诊断继发性骨骼肌FL的病例,在MRI、PET/CT及穿刺活检无法进行时,能谱增强CT可作为辅助诊断的潜在新方法。通过重建及比较不同组织的能谱衰减曲线,可初步确定病变来源,为广大医师在临床诊疗过程中提供诊断新思路、新方法。
-
![]()
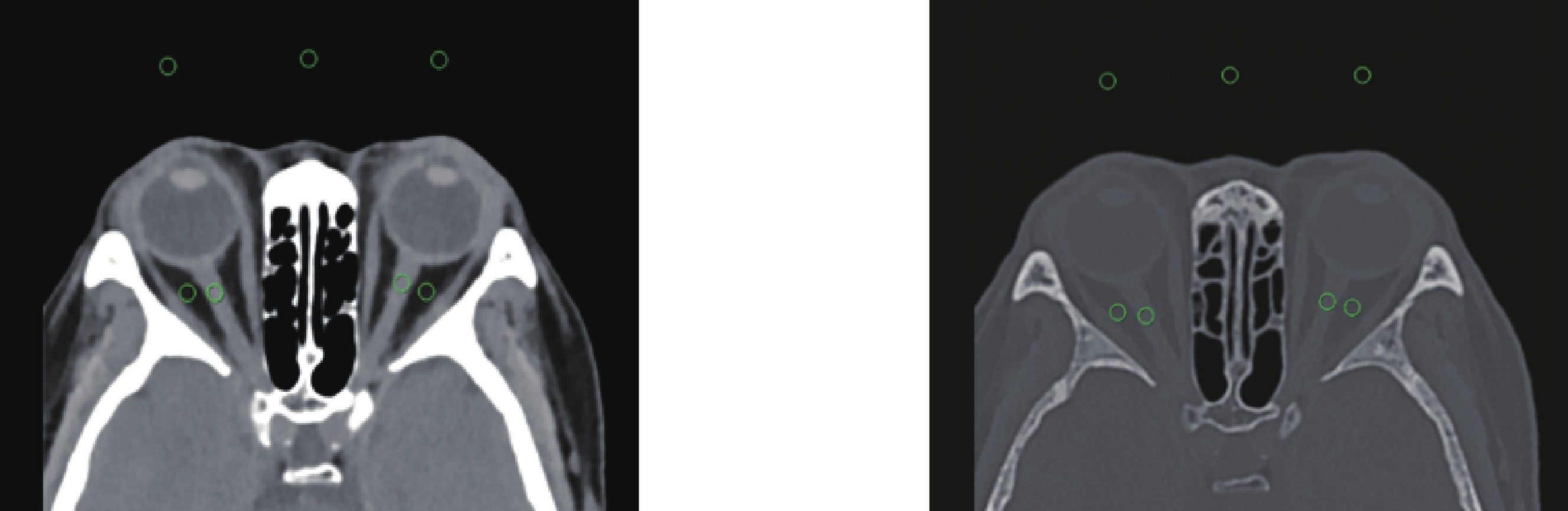
图 1 标准算法及骨算法重建横断图像的客观评价测量示意图
Figure 1. Objective evaluation measurement of standard algorithm and bone algorithm for reconstructing cross-sectional images
![]()
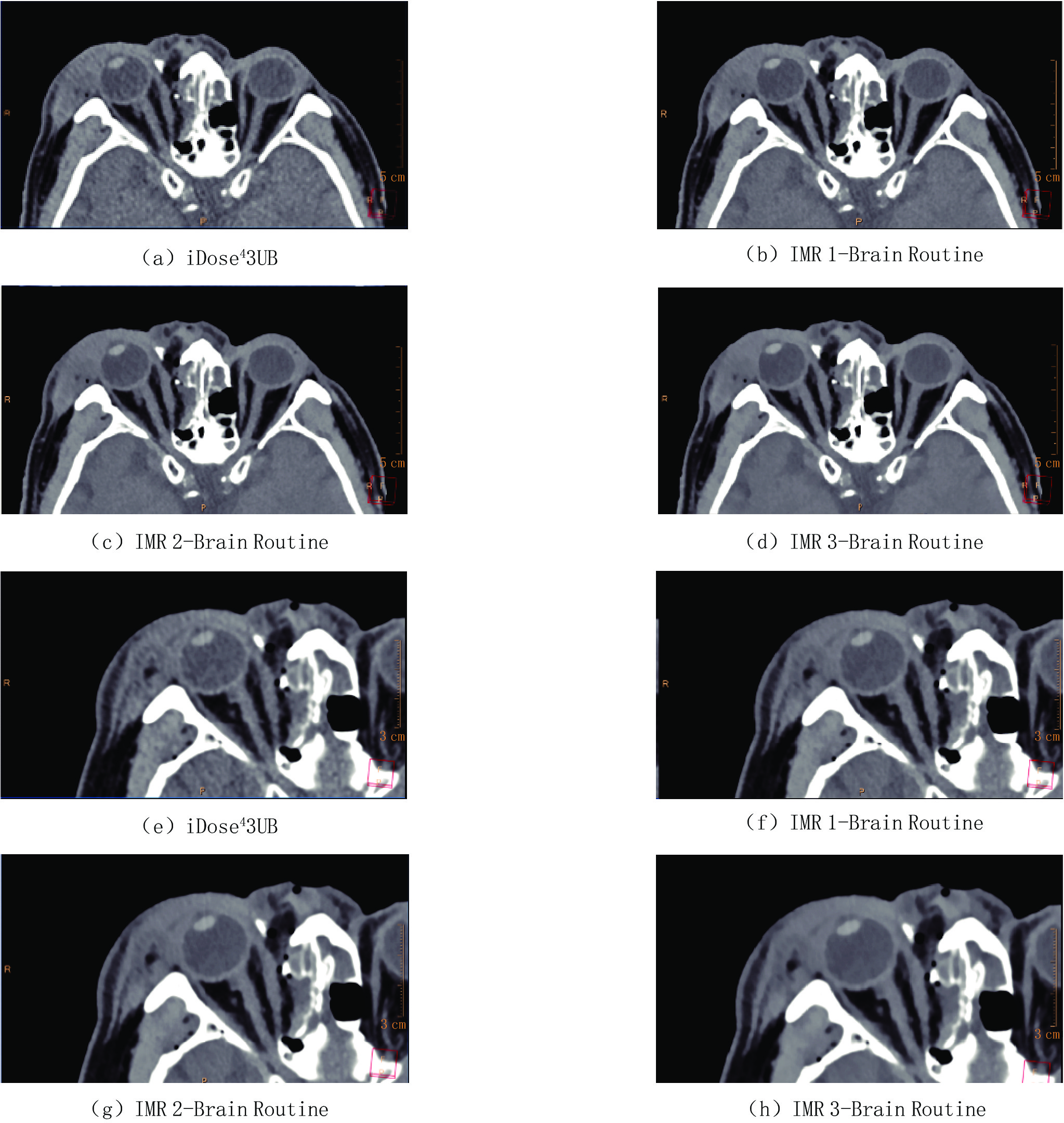
图 2 不同标准算法重建横断图像
注:患者,男55岁,右侧眼眶眶壁多发骨折,眼睑、泪腺及泪囊区软组织肿胀、积气并血肿形成。(a)和(e)为iDose4 技术、迭代水平Level 3、滤过核Brain Standard(UB)重建横断面图像;(b)~(d)、(f)~(h)为IMR技术、迭代水平Level 1~3、滤过核Brain Routine重建横断面图像。IMR 技术重建图像的SNR,CNR均优于iDose4,并随着迭代等级的提高而增加,但IMR Level 1(b)和(f)的图像质量评分最高5(4,5),细节显示最优。
Figure 2. Cross-sectional images reconstructed with different standard algorithms
![]()
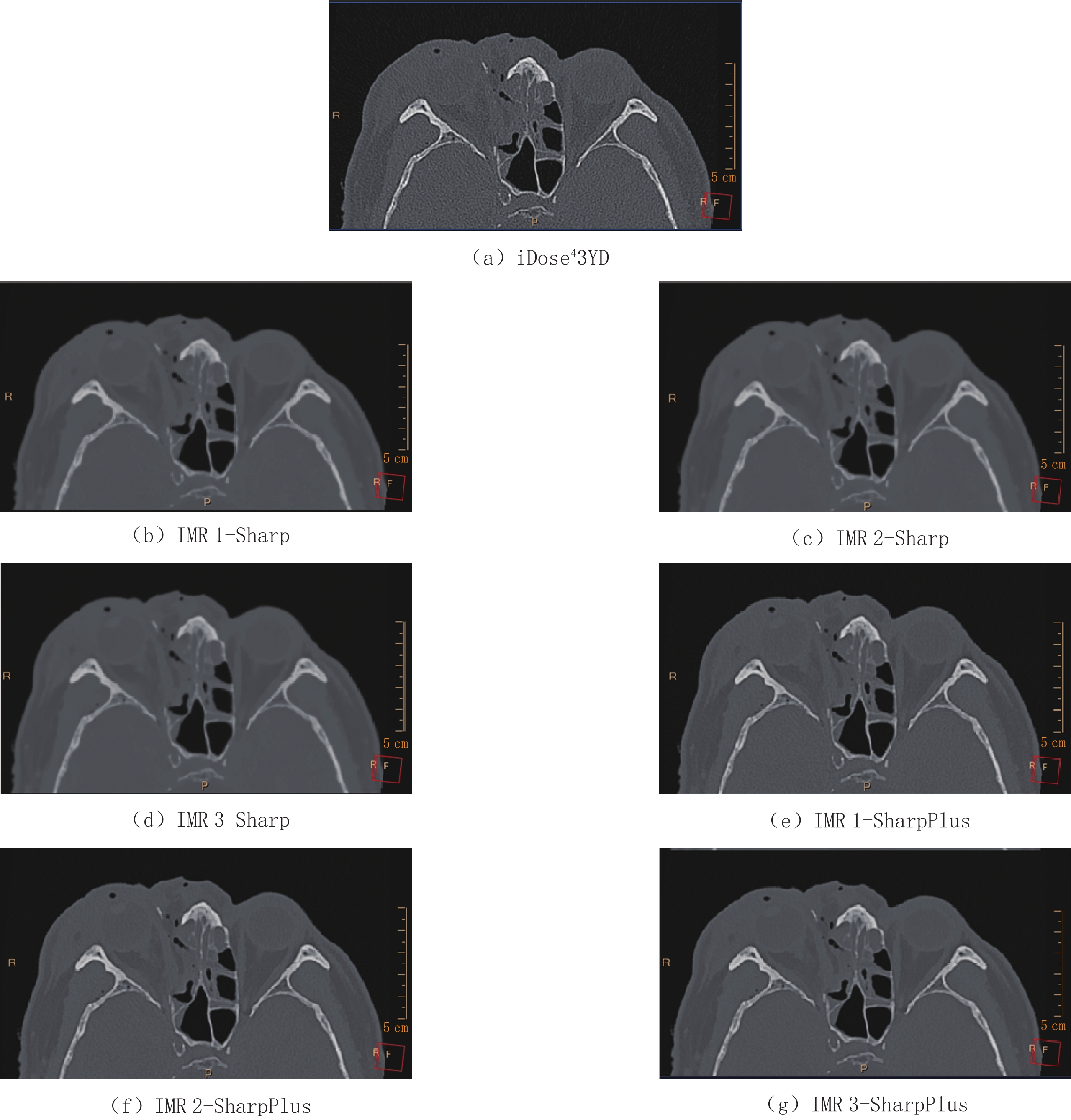
图 3 不同骨算法重建横断图像
注:患者,男55岁,右侧眼眶眶壁多发骨折。(a)为iDose4技术、迭代水平Level 3、滤过Y-Detail(YD)重建横断面图像;(b)~(d)为IMR技术、迭代水平Level 1~3、滤过核Sharp重建横断面图像;(e)~(g)为IMR技术、迭代水平Level 1~3、滤过核SharpPlus重建横断面图像。与iDose4相比,IMR重建图像的噪声随着滤过核及等级的变化大幅降低,SNR、CNR大幅增高;iDose4重建图像虽然噪声最大,SNR与CNR最低,但图像质量评分最高5(5,5),显示骨质最优。
Figure 3. Cross-sectional images reconstructed with different bone algorithms
表 1 不同标准算法重建图像平均CT值与SD值比较(HU,
$ (\bar{{x}}\pm {s}) $ )Table 1 Comparison of the average CT number and SD of image reconstruction with different standard algorithms
重建方法 CT值/HU SD/HU 视神经 眶内脂肪 背景空气 视神经 眶内脂肪 背景空气 iDose4 3 UB 32.27±5.76 -91.74±7.41 -1001.19±2.28 10.49±2.41 8.87±2.67 6.10±1.04 IMR 1-Brain Routine 33.43±5.30 -93.41±6.62 -1001.93±1.67 8.61±2.30 6.47±2.62 2.93±0.52 IMR 2-Brain Routine 33.59±5.27 -93.63±6.55 -1002.01±1.64 8.36±2.35 5.97±2.50 2.57±0.46 IMR 3-Brain Routine 33.48±5.15 -93.67±6.37 -1001.99±1.57 7.81±2.47 5.26±2.68 1.97±0.43 F 32.44 40.33 12.75 152.37 222.86 806.68 P <0.001 <0.001 <0.001 <0.001 <0.001 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 不同骨算法重建图像平均CT值与SD值比较(HU,
$ (\bar{{x}}\pm {s}) $ )Table 2 Comparison of the average CT number and SD of image reconstruction with different bone algorithms
重建方法 CT值/HU SD/HU 视神经 眶内脂肪 背景空气 视神经 眶内脂肪 背景空气 iDose4 3 YD 30.31±7.75 -97.03±8.62 -968.50±5.82 110.87±19.83 104.46±20.52 55.56±10.75 IMR 1-Sharp 32.94±4.83 -95.78±5.53 -1002.39±2.57 10.89±5.75 4.32±1.24 2.32±0.35 IMR 2-Sharp 33.17±4.86 -96.10±5.54 -1002.61±1.87 10.85±5.74 4.08±1.16 2.18±0.31 IMR 3-Sharp 33.17±4.86 -97.95±5.72 -1002.62±1.86 10.67±5.84 3.60±1.22 1.79±0.34 IMR 1-SharpPlus 38.85±6.05 -97.02±5.64 -1000.81±2.07 29.01±5.78 26.29±4.47 14.66±1.88 IMR 2-SharpPlus 38.86±5.83 -97.13±5.62 -1001.47±2.06 25.35±5.60 22.28±3.79 12.95±1.62 IMR 3-SharpPlus 38.86±5.58 -96.59±6.05 -1002.16±2.84 20.69±5.62 17.01±2.88 10.52±1.28 F 61.02 0.92 820.68 797.60 731.02 761.87 P <0.001 0.483 <0.001 <0.001 <0.001 <0.001
下载: 导出CSV
表 3 不同标准算法重建图像SNR与CNR值比较(
$ (\bar{{x}}\pm {s}) $ )Table 3 Comparison of SNR and CNR of image reconstruction with different standard algorithms
重建方法 SNR CNR iDose4 3 UB 3.26±1.04 21.00±4.30 IMR 1-Brain Routine 4.24±1.58 44.65±8.54 IMR 2-Brain Routine 4.44±1.73 51.07±9.79 IMR 3-Brain Routine 4.91±2.30 67.10±13.68 F 43.25 544.40 P <0.001 <0.001
下载: 导出CSV
表 4 不同骨算法重建图像SNR与CNR值比较(
$ (\overline{\mathit{x}}\pm \mathit{s}) $ )Table 4 Comparison of SNR and CNR of image reconstruction with different bone algorithms
重建方法 SNR CNR iDose4 3 YD 0.28±0.07 2.36±0.47 IMR 1-Sharp 3.99±2.28 56.67±9.06 IMR 2-Sharp 4.04±2.32 60.33±9.24 IMR 3-Sharp 4.22±2.60 74.67±14.32 IMR 1-SharpPlus 1.39±0.33 9.38±1.16 IMR 2-SharpPlus 1.60±0.39 10.62±1.26 IMR 3-SharpPlus 1.99±0.55 13.08±1.51 F 54.99 766.85 P <0.001 <0.001
下载: 导出CSV
表 5 不同标准算法重建图像质量评分比较[分,M(Q1,Q3)]
Table 5 Comparison of the image quality scores of image reconstruction with different standard algorithms
重建方法 图像质量评分 iDose4 3 UB 3(3,4) IMR 1-Brain Routine 5(4,5) IMR 2-Brain Routine 4(4,5) IMR 3-Brain Routine 4(3,4) $\chi^2 $ 144.22 P <0.001
下载: 导出CSV
表 6 不同骨算法重建图像质量评分比较[分,M(Q1,Q3)]
Table 6 Comparison of the image quality scores of image reconstruction with different bone algorithms
重建方法 图像质量评分 iDose4 3 YD 5(5,5) IMR 1-Sharp 3(3,3) IMR 2-Sharp 3(2,3) IMR 3-Sharp 3(3,3) IMR 1-SharpPlus 4(4,4) IMR 2-SharpPlus 4(4,4) IMR 3-SharpPlus 4(4,4) $\chi^2 $ 318.82 P < 0.001
下载: 导出CSV
-
[1] WIDMANN G, JURANEK D, WALDENBERGER F, et al. Influence of ultra-low-dose and iterative reconstructions on the visualization of orbital soft tissues on maxillofacial CT[J]. American Journal of Neuroradiology, 2017, 38(8): 1630−1635. DOI: 10.3174/ajnr.A5239.
[2] GREFFIER J, FRANDON J, LARBI A, et al. CT iterative reconstruction algorithms: A task-based image quality assessment[J]. European Radiology, 2020, 30(1): 487−500. DOI: 10.1007/s00330-019-06359-6.
[3] 曾宪春, 何波, 康绍磊, 等. 基于原始数据的迭代重建技术在眼眶CT平扫中的应用[J]. 中国医学影像技术, 2013, 29(6): 4. CENG X C, HE B, KANG S L, et al. Application of sinogram affirmed iterative reconstruction technique in orbital CT scan[J]. Chinese Journal of Medical Imaging Technology, 2013, 29(6): 4. (in Chinese).
[4] KLINK T, OBMANN V, HEVERHAGEN J, et al. Reducing CT radiation dose with iterative reconstruction algorithms: The influence of scan and reconstruction parameters on image quality and CTDIvol[J]. European Journal of Radiology, 2014, 83(9): 1645−1654. DOI: 10.1016/j.ejrad.2014.05.033.
[5] KONDRATYEV E, KARMAZANOVSKY G. Low radiation dose 256-MDCT angiography of the carotid arteries: Effect of hybrid iterative reconstruction technique on noise, artifacts, and image quality[J]. European Journal of Radiology, 2013, 82(12): 2233−2239. DOI: 10.1016/j.ejrad.2013.08.053.
[6] SMITH E A, DILLMAN J R, GOODSITT M M, et al. Model-based iterative reconstruction: Effect on patient radiation dose and image quality in pediatric body CT[J]. Radiology, 2014, 270(2): 526−534. DOI: 10.1148/radiol.13130362.
[7] 李昂, 沈君姝, 曹新志, 等. 原始数据迭代重建和70kV CT扫描对图像质量和辐射剂量的影响[J]. 医疗卫生装备, 2015, 36(3): 99−102. LI A, SHEN J S, CAO X Z, et al. Effects of sinogram-affirmed iterative reconstruction and 70kV CT scanning on image quality and radiation dose[J]. Chinese Medical Equipment Journal, 2015, 36(3): 99−102. (in Chinese).
[8] 潘丹, 陈鑫, 姜彦, 等. 迭代模型重组设置对不同辐射剂量下肝脏增强CT图像噪声及质量的影响[J]. 中华放射学杂志, 2015, (3): 173−178. PAN D, CHEN X, JIANG Y, et al. Knowledge-based iterative reconstruction technique: Effect of different reconstruction settings on image quality in hepatic contrast-enhanced CT at different radiation dose levels[J]. Chinese Journal of Radiology, 2015, (3): 173−178. (in Chinese).
[9] Von FALCK C, BRATANOVA V, RODT T, et al. Influence of sinogram affirmed iterative reconstruction of CT data on image noise characteristics and low-contrast detectability: An objective approach[J]. PLoS One, 2013, 8(2): e56875. DOI: 10.1371/journal.pone.0056875.
[10] MEHTA D, THOMPSON R, MORTON T, et al. Iterative model reconstruction: simultaneously lowered computed tomography radiation dose and improved image quality[J]. Medical Physics International Journal, 2013, 1: 147−155.
[11] 谭晶, 侯阳, 郭文力, 等. 全模型迭代重建技术在冠状动脉钙化模体扫描中的应用价值研究[J]. 中国临床医学影像杂志, 2016, 27(12): 867−870. DOI: 10.3969/j.issn.1008-1062.2016.12.009. TAN J, HOU Y, GUO W L, et al. A study of iterative model reconstruction technology in a cardiac coronary calcium anthropomorphic phantom[J]. Journal of China Clinic Medical Imaging, 2016, 27(12): 867−870. DOI: 10.3969/j.issn.1008-1062.2016.12.009. (in Chinese).
[12] JIA Y, ZHAI B, HE T, et al. The application of a new model-based iterative reconstruction in low-dose upper abdominal CT[J]. Academic Radiology, 2019, 26(10): e275−e283. DOI: 10.1016/j.acra.2018.11.020.
[13] TANG S, LIU Y, WANG Z, et al. Study on model iterative reconstruction algorithm vs. filter back projection algorithm for diagnosis of acute cerebral infarction using CT images[J]. Journal of Healthcare Engineering, 2021: 20215000102. DOI: 10.1155/2021/5000102.
[14] PAPROTTKA K J, KUPFER K, RIEDERER I, et al. Impact of dose reduction and iterative model reconstruction on multi-detector CT imaging of the brain in patients with suspected ischemic stroke[J]. Scientific Reports, 2021, 11(1): 22271. DOI: 10.1038/s41598-021-01162-0.
[15] IPPOLITO D, MAINO C, PECORELLI A, et al. Application of low-dose CT combined with model-based iterative reconstruction algorithm in oncologic patients during follow-up: Dose reduction and image quality[J]. The British Journal of Radiology, 2021, 94(1124): 20201223. DOI: 10.1259/bjr.20201223.
[16] TSAI M Y, LIANG H L, CHUO C C, et al. A novel protocol for abdominal low-dose CT scans adapted with a model-based iterative reconstruction method[J]. Journal of X-ray Science and Technology, 2023, 31(3): 453−461. DOI: 10.3233/XST-221325.
[17] LI T, TANG T, YANG L, et al. Coronary CT angiography with knowledge-based iterative model reconstruction for assessing coronary arteries and non-calcified predominant plaques[J]. Korean Journal of Radiology, 2019, 20(5): 729−738. DOI: 10.3348/kjr.2018.0435.
[18] SUN J, HU D, SHEN Y, et al. Improving image quality with model-based iterative reconstruction algorithm for chest CT in children with reduced contrast concentration[J]. La Radiologia Medica, 2019, 124(7): 595−601. DOI: 10.1007/s11547-019-00995-0.
[19] XU J, HU X, ZHANG Y, et al. Application of different levels of advanced modeling iterative reconstruction in brain CT scanning[J]. Current Medical Imaging, 2022, 18(13): 1362−1368. DOI:10.2174/ 1573405618666220516121722.
[20] IPPOLITO D, RIVA L, TALEI F C, et al. Diagnostic efficacy of model-based iterative reconstruction algorithm in an assessment of coronary artery in comparison with standard hybrid-Iterative reconstruction algorithm: Dose reduction and image quality[J]. La Radiologia Medica, 2019, 124(5): 350−359. DOI: 10.1007/s11547-018-0964-6.
[21] 袁姝娅. 极低剂量CT联合全模型迭代重建算法(IMR)评价胸部病变显示能力的模体和临床研究[D]. 苏州: 苏州大学: 2016. [22] HUSARIK D B, ALKADHI H, PUIPPE G D, et al. Model-based iterative reconstruction for improvement of low-contrast detectability in liver CT at reduced radiation dose: Ex-vivo experience[J]. Clinical Radiology, 2015, 70(4): 366−372. DOI: 10.1016/j.crad.2014.11.015.
[23] LEE H J, KIM J, KIM K W, et al. Feasibility of a low-dose orbital CT protocol with a knowledge-based iterative model reconstruction algorithm for evaluating Graves' orbitopathy[J]. Clinical Imaging, 2018: 51327-331.
[24] HOXWORTH J M, LAL D, FLETCHER G P, et al. Radiation dose reduction in paranasal sinus CT using model-based iterative reconstruction[J]. American Journal of Neuroradiology, 2014, 35(4): 644−649. DOI: 10.3174/ajnr.A3749.
[25] LAURENT G, VILLANI N, HOSSU G, et al. Full model-based iterative reconstruction (MBIR) in abdominal CT increases objective image quality, but decreases subjective acceptance[J]. European Radiology, 2019, 29(8): 4016−4025. DOI: 10.1007/s00330-018-5988-8.
[26] WIDMANN G, DALLA TORRE D, HOERMANN R, et al. Ultralow-dose computed tomography imaging for surgery of midfacial and orbital fractures using ASIR and MBIR[J]. International Journal of Oral and Maxillofacial Surgery, 2015, 44(4): 441−446. DOI: 10.1016/j.ijom.2015.01.011.
[27] 王天娇, 王沄, 马壮飞, 等. 全模型迭代算法(FIRST)在靶扫描靶重建颞骨CT成像的应用研究[J]. 中国医疗设备, 2021, 11: 76−80. WANG T J, WANG Y, MA Z F, et al. Forward projected model-based iterative reconstruction solution (FIRST) for target scan and target reconstruction in temporal bone CT image[J]. China Medical Devices, 2021, 11: 76−80. (in Chinese).
-
期刊类型引用(0)
其他类型引用(1)










计量
- 文章访问数: 218
- HTML全文浏览量: 45
- PDF下载量: 30
- 被引次数: 1


