
CT Radiomics Nomogram Prediction for Tumor Deposits and Prognosis in Colorectal Cancer
-
摘要:
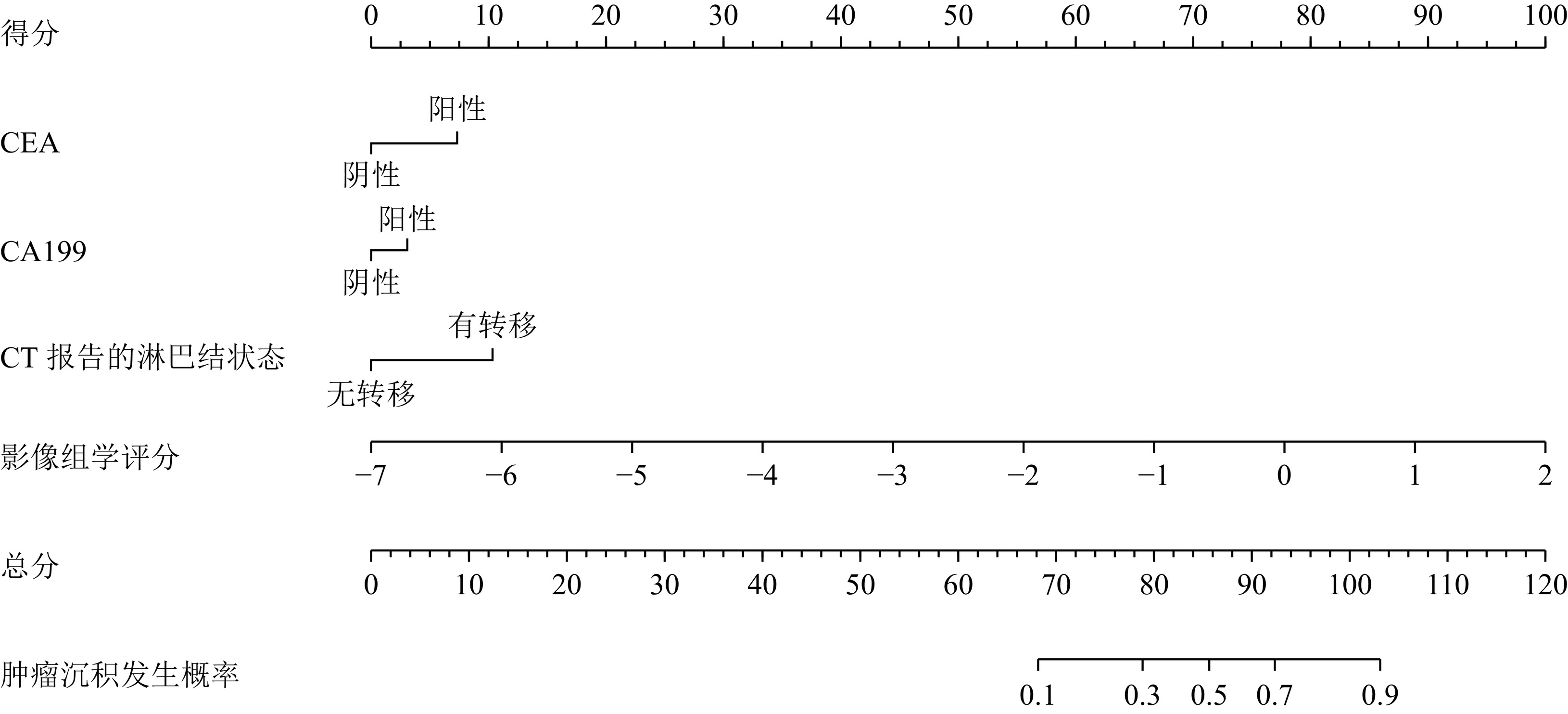
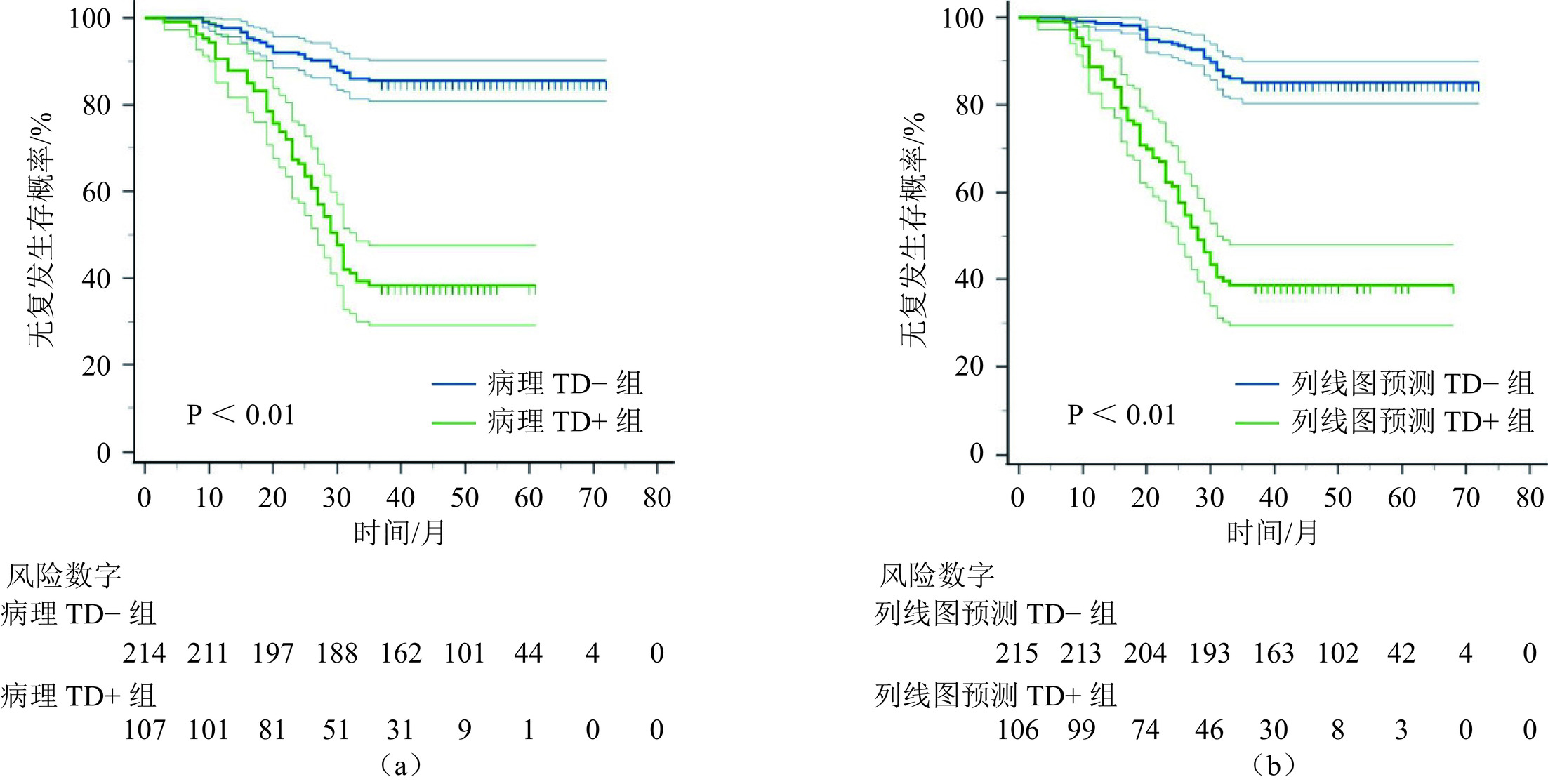
目的:建立CT影像组学列线图术前预测结直肠癌(CRC)患者肿瘤沉积(TD)和无复发生存(RFS)。方法:回顾性研究321例经手术病理证实的CRC患者,患者以6∶4分为训练集和验证集。从门静脉CT图像中提取基于肿瘤原发灶的影像组学特征,使用最小绝对收缩选择算子(LASSO)筛选与TD相关的影像组学特征。临床−影像组学列线图是根据筛选的影像组学特征和最具预测性的临床因素开发的。采用单、多因素Cox回归分析筛选3年无复发生存(RFS)的独立危险因素。结果:在训练集和验证集中,影像组学模型的曲线下面积(AUC)分别为0.80和0.79。结合影像组学特征和临床预测因子(CEA,CA199,CT报告的淋巴结状态)构建列线图以术前预测TD,列线图在训练集和验证集AUC分别为0.85和0.85。此外,列线图预测的TD是RFS的独立危险因素,TD阳性组的RFS差于TD阴性组。结论:CT影像组学列线图能够有效术前预测CRC患者TD和预后。
Abstract:Objective: To establish computed tomography (CT) radiomics nomogram for preoperative prediction of tumor deposits (TD) and recurrence-free survival (RFS) in patients with colorectal cancer (CRC). Methods: A retrospective study was conducted on 321 CRC patients confirmed by surgical pathology. The patients’ data were divided were divided into a training set and a validation set at a ratio of 6:4, respectively. Radiomics features based on the primary tumor site were extracted from portal venous phase CT images, and the least absolute shrinkage and selection operator (LASSO) algorithm was employed to select radiomics features associated with tumor deposits (TD). The LASSO regression algorithm was applied to choose radiomics features related to TD. A clinical-radiomics nomogram was developed based on the selected radiomics features and the most predictive clinical factors. Univariate and multivariate Cox regression analyses identified independent risk factors for a 3-year relapse free survive (RFS). Results: The radiomics model achieved an area under the curve (AUC) of 0.80 in the training set and 0.79 in the validation set. By integrating radiomics features with clinical predictors (CEA, CA199, and CT-reported lymph node status), a nomogram was developed for the preoperative prediction of TD. The nomogram achieved an AUC of 0.85 in the training and validation sets. Furthermore, TD predicted by the nomogram was an independent risk factor for RFS, with poorer RFS observed in the TD-positive group compared to the TD-negative group. Conclusion: CT radiomics nomogram can effectively preoperatively predict TD and prognosis in CRC patients.
-
Keywords:
- tomography /
- X-ray computed /
- radiomics /
- colorectal neoplasms /
- tumor deposits
-
-
![]()
图 2 预测CRC患者TD的影像组学列线图
Figure 2. The radiomics nomogram for predicting TD in patients with CRC
![]()
图 3 临床模型、影像组学模型及列线图预测CRC患者TD的ROC曲线
Figure 3. The ROC curves for predicting CRC patients TD using the clinical model, radiomics model, and nomogram
![]()
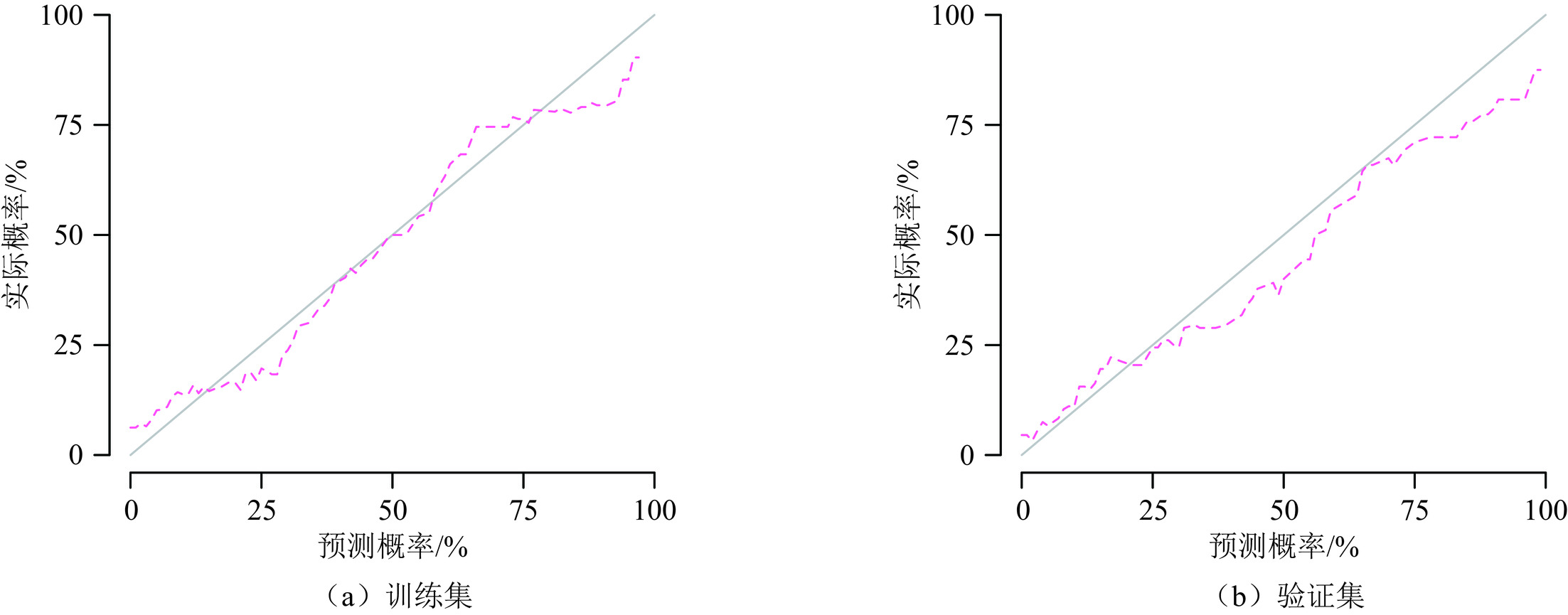
图 4 列线图预测CRC患者TD的校准曲线
Figure 4. Calibration curve for predicting TD in CRC patients using the nomogram
![]()
图 5 不同模型预测CRC患者TD的决策曲线
Figure 5. Decision curve analysis for predicting TD in CRC patients using different models
![]()
图 6 TD阳性和TD阴性CRC患者示例
注:(a)69岁男性右侧结肠癌患者,CT图像(左)、结肠癌HE染色图像,X20(中)、TD HE染色图像,X20(右);(b)52岁女性乙状结肠癌患者,CT图像(左)、乙状结肠癌HE染色图像,X20(中)、TD HE染色图像,X20(右);(c)76岁男性乙状结肠癌患者,CT图像(左)、乙状结肠癌HE染色图像,X20(中)、正常淋巴结HE染色图像,X20(右)。
Figure 6. Representative examples of TD-positive and TD-negative CRC patients
![]()
图 7 根据病理TD状态(a)和列线图预测TD状态(b)绘制RFS曲线
Figure 7. RFS curves based on pathological TD status (a) and nomogram-predicted TD status (b)
表 1 321例CRC患者基线资料比较
Table 1 Comparison of baseline data of 321 patients with CRC
临床资料 TD阴性(n=214例) TD阳性(n=107例) $\chi^2 $/Z P 性别 0.41 0.52 女 90 49 男 124 58 年龄 67 (60,74) 68 (62,74) −0.35 0.72 CEA (阳性>5 ng/mL) 19.55 <0.01 阴性 128 36 阳性 86 71 CA199 (阳性>30 U/mL) 22.63 <0.01 阴性 181 65 阳性 33 42 白蛋白/球蛋白比值
(阳性<1.5 or >2.5)2.25 0.13 阴性 117 49 阳性 97 58 乳酸脱氢酶 2.62 0.11 阴性 185 85 阳性 29 22 肿瘤位置 4.70 0.10 右侧结肠 63 36 左侧结肠 110 42 直肠 41 29 CT报告的淋巴结状态 22.21 <0.01 无转移 143 42 有转移 71 65 肿瘤大小/cm 4.20(3.50,5.50) 4.50(3.00,5.90) −1.05 0.29 病理T分期 9.40 0.02 1 7 0 2 20 5 3 74 29 4 113 73 病理N分期 49.20 <0.01 0 130 25 1 63 44 2 21 38 病理M分期 22.14 <0.01 0 208 88 1 6 19 肿瘤分级 9.72 <0.01 Ⅰ 13 1 Ⅱ 171 79 Ⅲ 30 27  下载: 导出CSV
下载: 导出CSV
表 2 影像组学模型、临床模型及列线图预测CRC患者TD的效能
Table 2 The efficacy of radiomics model, clinical model and nomogram in predicting TD in patients with CRC
模型 AUC 准确率 敏感度 特异度 影像组学模型 训练集 0.80 0.75 0.72 0.77 验证集 0.79 0.70 0.67 0.72 临床模型 训练集 0.72 0.68 0.55 0.74 验证集 0.71 0.69 0.45 0.80 列线图 训练集 0.85 0.82 0.71 0.88 验证集 0.85 0.77 0.64 0.84
下载: 导出CSV
-
[1] SIEGEL R L, MILLER K D, FUCHS H E, et al. Cancer statistics, 2022[J]. CA: A Cancer Journal for Clinicians, 2022, 72(1): 7-33. DOI: 10.3322/caac.21708.
[2] RYU H S, KIM J, PARK Y R, et al. Recurrence patterns and risk factors after curative resection for colorectal cancer: Insights for postoperative surveillance strategies[J]. Cancers (Basel), 2023, 15(24): 5791. DOI: 10.3390/cancers15245791.
[3] DELATTRE J F, SELCEN OGUZ ERDOGAN A, COHEN R, et al. A comprehensive overview of tumour deposits in colorectal cancer: Towards a next TNM classification[J]. Cancer Treatment Reviews, 2022, 103: 102325. DOI: 10.1016/j.ctrv.2021.102325.
[4] MOON J Y, LEE M R, HA G W. Prognostic value of tumor deposits for long-term oncologic outcomes in patients with stage III colorectal cancer: A systematic review and meta-analysis[J]. International Journal of Colorectal Disease, 2022, 37(1): 141-151. DOI: 10.1007/s00384-021-04036-z.
[5] PRICOLO V E, STEINGRIMSSON J, MCDUFFIE T J, et al. Tumor deposits in stage III colon cancer: Correlation with other histopathologic variables, prognostic value, and risk stratification-time to consider “N2c”[J]. American Journal of Clinical Oncology, 2020, 43(2): 133-138. DOI: 10.1097/COC.0000000000000645.
[6] AMIN M B, GREENE F L, EDGE S B, et al. The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging[J]. CA: A Cancer Journal for Clinicians, 2017, 67(2): 93-99. DOI: 10.3322/caac.21388.
[7] RATTO C, RICCI R, ROSSI C, et al. Mesorectal microfoci adversely affect the prognosis of patients with rectal cancer[J]. Diseases of the Colon and Rectum, 2002, 45(6): 733-743. DOI: 10.1007/s10350-004-6288-8.
[8] ZHANG L N, XIAO W W, XI S Y, et al. Tumor deposits: Markers of poor prognosis in patients with locally advanced rectal cancer following neoadjuvant chemoradiotherapy[J]. Oncotarget, 2016, 7(5): 6335-6344. DOI: 10.18632/oncotarget.6656.
[9] SHI M, ZHANG H, YAO G, et al. The role of tumor deposits in predicting the efficacy of chemotherapy in stage III colon cancer[J]. Frontiers in Oncology, 2020, 10: 586603.
[10] ROLLVEN E, ABRAHAM-NORDLING M, HOLM T, et al. Assessment and diagnostic accuracy of lymph node status to predict stage III colon cancer using computed tomography[J]. Cancer Imaging, 2017, 17(1): 3. DOI: 10.1186/s40644-016-0104-2.
[11] ROLLVEN E, BLOMQVIST L, OISTAMO E, et al. Morphological predictors for lymph node metastases on computed tomography in colon cancer[J]. Abdominal Radiology (NY), 2019, 44(5): 1712-1721. DOI: 10.1007/s00261-019-01900-z.
[12] CHEN L D, LI W, XIAN M F, et al. Preoperative prediction of tumour deposits in rectal cancer by an artificial neural network-based US radiomics model[J]. European Radiology, 2020, 30(4): 1969-1979. DOI: 10.1007/s00330-019-06558-1.
[13] YANG Y S, FENG F, QIU Y J, et al. High-resolution MRI-based radiomics analysis to predict lymph node metastasis and tumor deposits respectively in rectal cancer[J]. Abdominal Radiology, 2021, 46(3): 873-884. DOI: 10.1007/s00261-020-02733-x.
[14] MIZUNO H, MIYAKE H, NAGAI H, et al. Optimal cutoff value of preoperative CEA and CA19-9 for prognostic significance in patients with stage II/III colon cancer[J]. Langenbeck’s Archives of Surgery, 2021, 406(6): 1987-1997. DOI: 10.1007/s00423-021-02236-3.
[15] SHAN J, GU B, SHI L, et al. Prognostic value of CEA and CA19-9 in patients with local advanced rectal cancer receiving neoadjuvant chemoradiotherapy, radical surgery and postoperative chemotherapy[J]. Translational Cancer Research, 2021, 10(1): 88-98. DOI: 10.21037/tcr-20-2269.
[16] LONG Q, XU Y, MA G, et al. Prognostic value of tumor deposit counts in patients with stage III colorectal cancer: A population-based study[J]. Journal of Investigative Surgery, 2022, 35(7): 1502-1509. DOI: 10.1080/08941939.2022.2069306.




计量
- 文章访问数: 203
- HTML全文浏览量: 64
- PDF下载量: 42


