
The Value of Dual-energy CT Virtual Calcium Subtraction Technique in the Diagnosis of Fresh Sacrococcygeal Fractures in the “Sitting Position”
-
摘要:
目的:使用双能CT虚拟去钙技术评估不同经验医师诊断“臀坐式”骶尾椎急性损伤的诊断效能。方法:前瞻性纳入2021年11月至2024年1月因急性外伤导致骶尾部疼痛的29例患者,共174块椎体(145块骶椎、29块尾椎),获取其MRI及DECT数据;以MRI结果为参考,3名放射科医师(诊断经验分别为1、4和10年)分别使用常规CT和VNCa彩色编码图进行分析。结果:使用VNCa技术后,3名医师诊断一致性Kappa值显著提升,分别从0.452、0.615、0.735提升至0.775、0.825、0.897,诊断正确率显著提高,分别为92.5%、94.3%和96.6%,3名医师差异无统计学意义;定量分析表明,正常骨髓的平均VNCa CT值为(-84.2±20.3) HU,骨髓水肿(BME)为(-37.4±18.8) HU,两者有显著差异;以MRI为标准,VNCa CT值区分正常骨髓和BME的AUC为0.962,最佳截断值为 -57.1 HU,对应敏感性和特异性分别为91.9% 和90.2%。结论:DECT VNCa技术显著提高了不同经验医师诊断骶尾椎急性损伤的效能,尤其对经验不足的医师,VNCa CT值有助于诊断。
Abstract:Purpose: The aim of this study was to evaluate the diagnostic performance of virtual non-calcium imaging using dual-energy computed tomography (CT) for acute sacrococcygeal injuries diagnosed by radiologists with varying levels of experience. Methods: A prospective study was employed and 29 patients presenting with acute coccygeal pain due to trauma between November 2021 and January 2024, involving a total of 174 vertebrae (145 sacral, 29 coccygeal), were enrolled. Both magnetic resonance imaging (MRI) and DECT data were acquired. Three radiologists with 1, 4, and 10 years of experience analyzed conventional CT and VNCa color-coded images, using MRI as the reference standard. Results: Following the application of VNCa imaging, the inter-rater agreement among the three radiologists significantly improved, with Kappa values increasing from 0.452, 0.615, and 0.735 to 0.775, 0.825, and 0.897, respectively. Diagnostic accuracy also notably increased to 92.5%, 94.3%, and 96.6% for the three radiologists, with no statistically significant differences observed among them. Quantitative analysis revealed an average VNCa CT value of (−84.2±20.3) HU for normal bone marrow and (−37.4±18.8) HU for bone marrow edema, showing a significant difference between the two. Using MRI as the reference standard, the area under the curve for distinguishing normal bone marrow from BME based on VNCa CT values was 0.962, with an optimal cutoff of −57.1 HU, yielding a sensitivity and specificity of 91.9% and 90.2%, respectively. Conclusion: DECT VNCa imaging significantly enhances the diagnostic efficacy of radiologists with varying levels of experience in acute coccygeal injury assessment, particularly benefiting less-experienced physicians. VNCa CT values contribute substantially to diagnostic accuracy in this context.
-
常规CT图像实际上是在混合能量X线束的基础上成像,低能X线束易被人体组织吸收,而透过的高能X线束容易产生射线束硬化伪影,现在通常的做法是采用特定的算法对射线束硬化伪影进行校正。但是由于常规CT本身的缺陷,这种校正常常不能充分对其进行抵消,随之产生的非线性伪影会造成疾病的误诊和漏诊[1-2]。同时,由于光电效应和康普顿散射的存在,拥有不同原子序数的物质会呈现出相似的表现,使得CT的密度分辨率不佳[3]。此外,如果采用低电压扫描图像噪声会增加,但图像的对比度分辨率更好。而采用高电压方案则图像的噪声得到抑制,但对比度分辨率进一步下降,且同等情况下的辐射剂量增加。
双能CT利用高低两种能量进行成像,在此基础上通过物质分离算法,重建的虚拟单能图像可以进一步模拟各级能量下不同物质的衰减[4-5]。既往研究表明,双能CT虚拟单能成像相比传统CT可以降低图像噪声,提升图像质量[6-10]。但是,相关研究大多都是临床研究,受限于辐射剂量,不能做到同一个研究对象的自身对照,患者差异会是影响研究结果的潜在重要影响因素。
因此,本研究旨在运用体模,对比双源双能CT低、中、高3档虚拟单能能级图像和两种常规CT图像的图像质量,探讨虚拟单能图像的临床可行性。
1. 资料与方法
1.1 体模
采用CT图像质量控制体模Catphan 500中的高对比度分辨率CTP 528和低对比度分辨率CTP 515两个组间。CTP 528(图1(a))由21组高密度线对(呈放射状分布)的结构,分辨率为1~21 lp/cm。CTP 515(图1(b))由内外两层低密度孔阵(呈放射状分布)的结构构成,内层孔阵的对比度分别为0.3%、0.5%和1.0%,直径分别为3、5、7和9 mm;外层孔阵的对比度分别为0.3%、0.5%和1.0%,直径分别为2、3、4、5、6、7、8、9和15 mm。
1.2 仪器与方法
通过西门子SOMATOM Force双源双能CT分别扫描Catphan 500的CTP 528和CTP 515组件(图1),分别采用双球管双能模式扫描与单球管单能模式扫描。所有扫描方案固定剂量20 mGy,螺距1.0,机架旋转速度为1 s/r。其中双能模式扫描参数为双球管电压对100/150 Sn kVp,电流294 mAs/147 mAs;单能扫描方案采用120 kVp,电流分别为299 mAs和205 mAs。
所有图像重建层厚5 mm,标准滤波函数Qr40(双能模式)或Br40(单能模式)和中等迭代重建算法ADMIRE 2。双能扫描重建3档虚拟单能图像:A组40 keV,B组70 keV,C组100 keV;单能混合能量扫描图像为:D组120 kVp。
1.3 图像质量评估
评估CT图像质量的几个主要参数分别为:高对比度分辨率、低对比度分辨率、图像噪声、信噪比(signal-to-noise ratio,SNR)和对比噪声比(contrast-to-noise ratio,CNR)。
所有图像由两名具有5年以上阅片经验的放射科医生采用独立盲法测量并分别进行主观与客观评价。主观评价记录包含高对比度分辨率组件CTP 528的最佳线对(1~2 lp/cm)以及低对比度分辨率组件CTP 515所能分辨的外层1% 浓度下的最小孔径(直径2~15 mm,要求分辨80% 以上有效面积),比较两名医生的主观评价结果,如有分歧则由另一名高年资医生做最终评判。
客观测量选取两个面积均为100 mm2的圆形感兴趣区域(region of interest,ROI)分别测量CTP 515组件中1% 浓度中直径最大(15 mm)孔径和邻近固态水背景的CT值(CTm和CTw,单位HU),将15 mm孔径ROI标准差(SD)定义为噪声(单位HU),随后计算各组图像SNR=CTm/SD和CNR=(CTm- CTw)/SD。所有主观及客观评价指标均在各组件中心的连续3个层面上进行测量;主观指标取3个层面的最佳值。
1.4 统计学分析
运用SPSS 23.0统计分析软件进行分析。连续性变量数据以
$\bar{x}\pm s $ 表示。两名医生的主观一致性评价采用统计分析Cohen's Kappa检验,客观一致性评价采用Spearman相关性分析。5组图像的高对比度分辨率和低对比度分辨率采用秩和检验;5组图像的SD、SNR及CNR的比较采用单因素方差分析。双能模式虚拟能级图像的组内比较采用Bonferroni矫正,以P<0.05认为差异具有统计学意义。
2. 结果
2.1 一致性评价
两名医生对各组图像的高对比度分辨率和低对比度分辨率的主观及客观一致性评价良好,Kappa系数为0.667,Spearman相关系数r=0.920,差异均具有统计学意义。
2.2 四组图像对比度分辨率比较
D组图像具有最佳的高对比度分辨率(线对6 lp/cm),A组~C组图像的最佳线对数均为5 lp/cm。对于低对比度分辨率,A组和B组图像表现最佳(均为4 mm孔径),其余两组图像的最小孔径为5 mm(表1)。3档虚拟单能图像对比见图2。
表 1 四组图像高对比度分辨率和低对比度分辨率比较Table 1. Comparison of high-contrast resolution and low-contrast resolution of four groups of images对比度分辨率 A组
(40 keV)B组
(70 keV)C组
(100 keV)D组
(120 kVp)高对比对分辨率(线对/(lp/cm)) 5 5 5 6 低对比度分辨率(孔径直径/mm) 4 4 5 5 ![]() 图 2 三档虚拟单能图像的示例图(a)~(c)分别代表40、70和100 keV图像;(a1)、(b1)和(c1)分别代表相同窗宽窗位下(400,0)40、70和100 keV的图像对比;(a2)和(a3)、(b2)和(b3)、(c2)和(c3)分别代表相应虚拟单能图像的CTP 515低对比度分辨率和CTP 528高对比度分辨率模块图像。Figure 2. Schematic diagram for the three series of virtual monochromatic images
图 2 三档虚拟单能图像的示例图(a)~(c)分别代表40、70和100 keV图像;(a1)、(b1)和(c1)分别代表相同窗宽窗位下(400,0)40、70和100 keV的图像对比;(a2)和(a3)、(b2)和(b3)、(c2)和(c3)分别代表相应虚拟单能图像的CTP 515低对比度分辨率和CTP 528高对比度分辨率模块图像。Figure 2. Schematic diagram for the three series of virtual monochromatic images2.3 四组图像噪声、SNR和CNR比较
各组图像间噪声差异有统计学意义,其中A组图像噪声最大(4.167±0.289),C组图像噪声最小(2.333±0.289);噪声在虚拟单能组内(A组~C组)差异有统计学意义。各组图像间SNR差异有统计学意义,C组图像SNR最高(37.944±3.949);SNR随着虚拟单能能级的升高而增加,SNR在虚拟单能组内(A组~C组)间差异有统计学意义。B组图像的CNR最高(3.361±0.875),但各组图像CNR差异无统计学意义;组内比较方面,虚拟单能组(A组~C组)的CNR差异也无统计学意义(表2)。
表 2 四组图像图噪声参数评价结果比较Table 2. Comparison of the evaluation results of the noise parameters of the five groups of images组别 SD/HU SNR CNR A组(40 keV) 4.167±0.289 10.942±0.465 2.383±0.336 B组(70 keV) 2.500±0.500 24.028±5.000 3.361±0.875 C组(100 keV) 2.333±0.289 37.944±3.949 3.139±0.337 D组(120 kVp) 2.500±0.000 30.806±1.398 2.778±0.241 $P $ <0.001 <0.001 0.179 3. 讨论
CT在临床诊疗中扮演着重要的作用,但常规CT在选择最优管电压方面具有一定的妥协性。选择低电压代表更低的辐射剂量,虽然其具有更高的图像对比度,在常规低剂量肺筛的作用显著,但是也在一定程度上牺牲了图像质量,增加了图像噪声,因此在其他领域的作用受限;而选择高电压方案则与此相反,虽能获得更佳的图像质量,但其图像对比度下降且会增加病人的受照辐射剂量。
由于常规CT扫描采用的是混合能量X射线谱,以120 kVp为例,低能的X射线被组织吸收,导致其平均能量大约在90 keV左右,在这种能量下,钙与碘具有相似的衰减系数,因此两种物质在常规CT上具有相似的高密度,这不利于钙化斑块的检出[11]。双能CT在不增加患者辐射剂量的基础上,可以重建不同虚拟单能能级的图像,利用不同物质/组织在不同X线束下的衰减系数不同,以此获得不同对比度的CT图像,并且可以通过“动态”观察不同物质随着能级变化的特点,实现常规CT上不能实现的微小病灶的检出和病灶成分的鉴别。目前有研究证明其在心血管疾病、肿瘤检出、颅内出血、炎症性肠病等领域的效果显著[12-16]。
本研究分别研究低、中、高3档虚拟单能能级图像的图像质量,3档能级图像具有相似的高/低对比度分辨率,100 keV低对比度分辨率稍有下降。既往研究表明,低keV下图像的低对比度分辨率(即密度分辨率)较高,图像对不同软组织的分辨较好,但是同时伴随着一定的伪影,而高keV下图像的伪影得到抑制,但图像的密度分辨率下降。因此,低keV虚拟单能图像有助于CT静脉造影及软组织肿块等的检出,而高keV则有助于抑制如心脏支架、人工髋关节伪影等对图像质量的影响[4,11]。
图像噪声方面,随着能级的增加,图像平均噪声降低,而70 keV的CNR更高,100 keV的SNR最高。总体来看,本体模研究表明,70 keV是比较均衡的虚拟单能能级;不同研究也表明,70 keV有助于冠状动脉、肺血管、胰腺癌、小肠梗阻等的显示或检出[17-20]。目前最常用的3档双能成像模式(双源双能量、快速kVp切换以及双层探测器模式),与常规120 kVp图像等效的虚拟单能图像的能级均在70 keV左右。同等条件下,70 keV图像往往具有更低的辐射剂量,更佳的图像质量。本研究中,70 keV图像的平均噪声比常规120 kVp图像更低,而CNR更高,两者的高/低对比度分辨率相近,提示70 keV图像具有更高的图像质量,这与前人的研究结果相一致[21-22]。
本研究也存在一定的局限性。①本研究只对比了低、中、高3档虚拟单能能级,在全面对比虚拟单能图像之间的差异方面还显不足;②本研究用的体模为研究对象,且只选取了其中两个模块进行评价,对图像质量的全面评价略显不足,例如对比虚拟单能图像和常规CT图像的CT值准确性等方面还有待进一步研究;③本模型研究在临床方面的指导作用还有待进一步阐明。
总之,能谱CT虚拟单能图像相比传统混合能量CT图像可以降低图像噪声并提升图像质量。
-
![]()
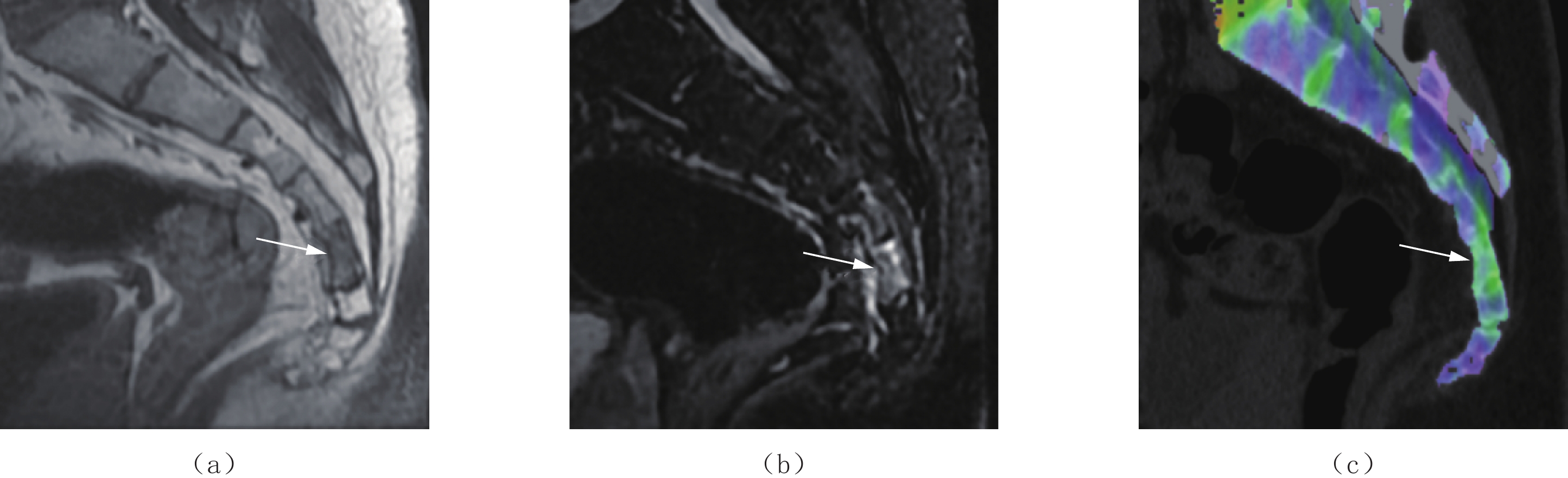
图 1 骶尾椎外伤致骶5椎体骨髓水肿的图像(白箭)
注:(a)矢状位T1WI显示第5骶椎片状低信号(白箭);(b)矢状位STIR序列显示第5骶椎片状高信号(白箭);(c)矢状位VNCa彩色编码成像显示第5骶椎片状绿色信号(白箭),提示第5骶椎隐匿性骨折。
Figure 1. Image of bone marrow edema at the S5 vertebral body due to coccygeal trauma (white arrow).
![]()
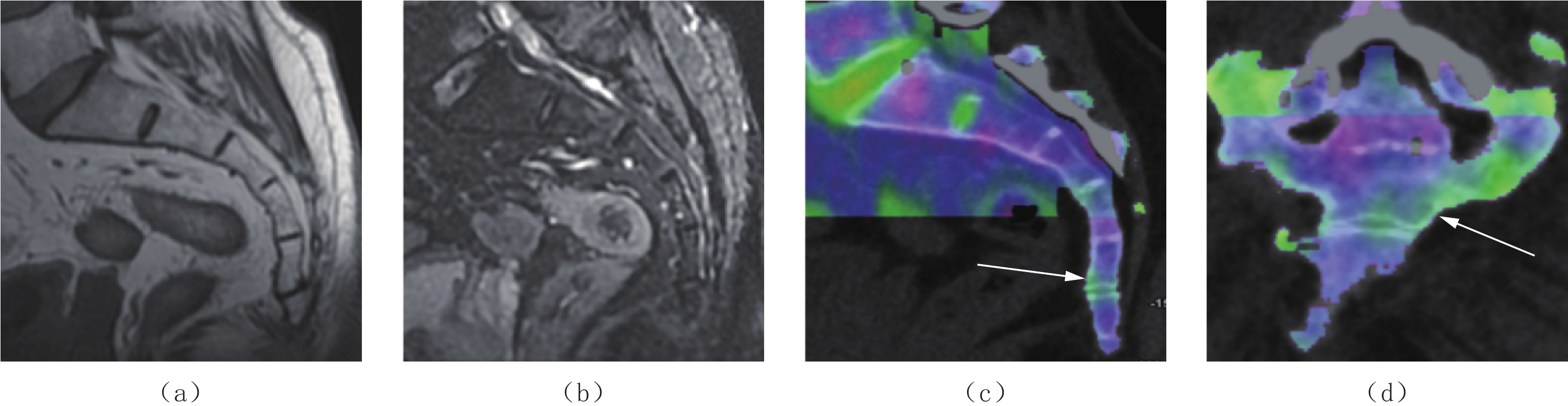
图 2 3名医师的假阳性结果
注:1名62岁男性骶尾椎外伤的图像(a)、(b)矢状位T1WI和STIR序列未见明显异常低或高信号;(c)、(d)矢状位和冠状位VNCa彩色编码成像显示第5骶椎下缘片状绿色信号(白箭)。
Figure 2. False-positive results from three physicians
![]()
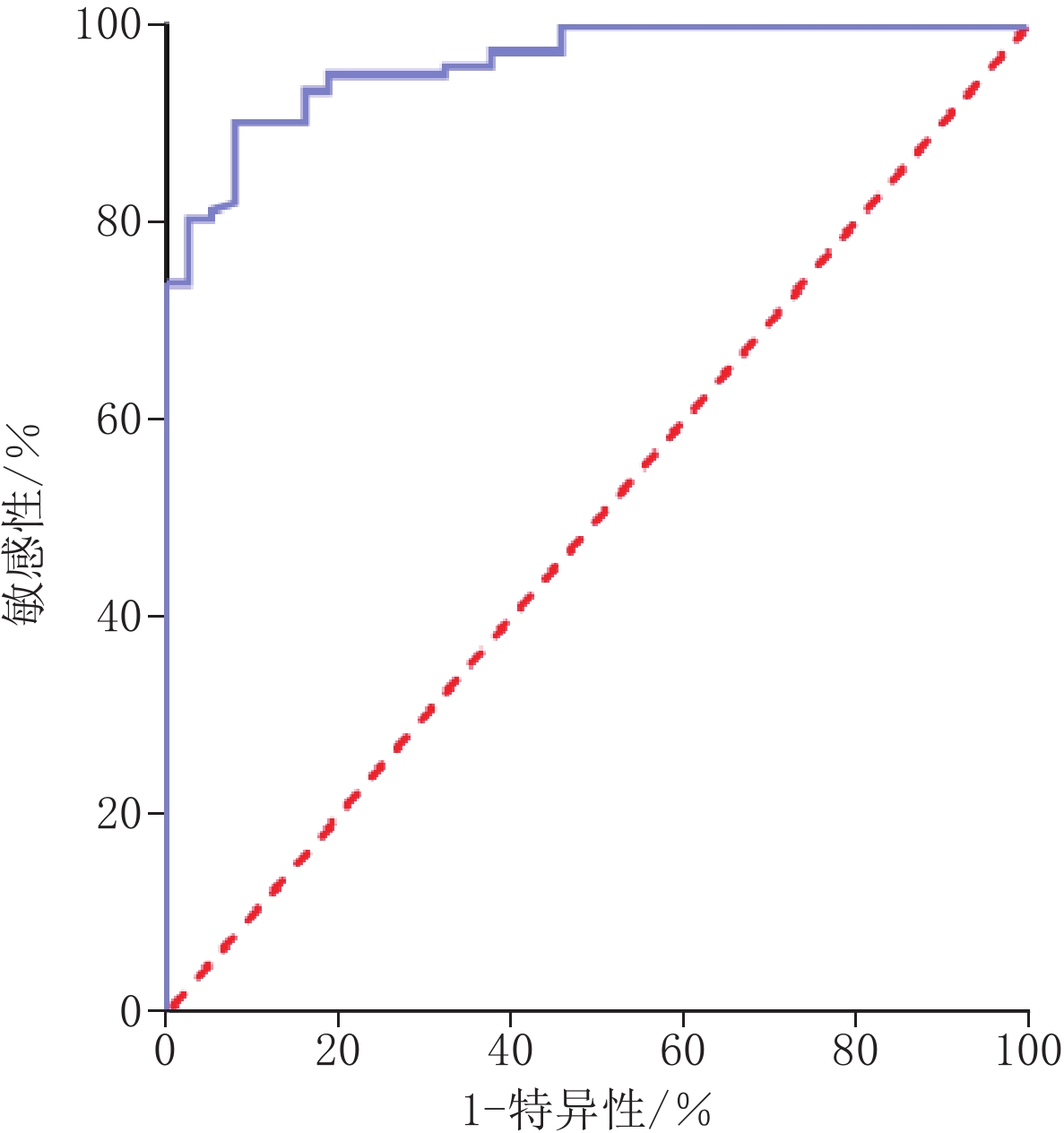
图 3 基于VNCa CT值区分正常骨髓和BME的ROC曲线
Figure 3. ROC curve for discriminating normal bone marrow from BME based on VNCa CT values
表 1 3名医师使用常规CT及DECT诊断椎体急性损伤结果
Table 1 Results of routine CT and DECT diagnosis of acute vertebral injuries by three physicians
医师 常规CT MRI 合计 VNCa MRI 合计 1 0 1 0 A医师 1 20 14 34 1 30 6 36 0 17 123 140 0 7 131 138 B医师 1 25 10 35 1 31 4 35 0 12 127 139 0 6 133 139 C医师 1 28 6 34 1 34 3 37 0 9 131 140 0 3 134 137 注: 0为正常骨髓;1为骨髓水肿。  下载: 导出CSV
下载: 导出CSV
表 2 3名医师使用常规CT及DECT诊断效能结果(%)
Table 2 Diagnostic performance of routine CT and DECT by three physicians (%)
医师 项目 敏感度 特异度 误诊率 漏诊率 PPV NPV 正确率 Youden A医师 常规CT 54.1(37.1, 70.2) 89.8(83.1, 94.1) 10.2 45.9 58.8 87.9 82.1 0.439 VNCa 81.1(64.3, 91.4) 95.6(90.3, 98.2) 4.4 18.9 83.3 94.9 92.5 0.767 B医师 常规CT 67.6(50.1, 81.4) 92.7(86.6, 96.2) 7.3 32.4 71.4 91.4 87.4 0.603 VNCa 83.8(67.3, 93.2) 97.1(92.2, 99.1) 2.9 16.2 88.6 95.7 94.3 0.809 C医师 常规CT 75.7(58.4, 87.6) 95.6(90.3, 98.2) 4.4 24.3 82.4 93.6 91.4 0.713 VNCa 91.9(77.0, 97.9) 97.8(93.2, 99.4) 2.2 8.1 91.9 97.8 96.6 0.897 注:PPV为阳性预测值;NPV为阴性预测值;括号中的数值表示 95% 置信区间。
下载: 导出CSV
表 3 正常骨髓和BME的VNCa CT值的比较
Table 3 VNCa CT numbers for normal bone marrow and BME
项目 分级 统计检验 MRI grade 0 MRI grade 1 t P VNCa CT 值/HU -84.2±20.3 -37.4±18.8 12.506 <0.001 范围/HU -150~39.8 -70.6~15.5 注: 0为正常骨髓; 1为骨髓水肿。P<0.05表示有统计学差异。
下载: 导出CSV
-
[1] 陈子锴, 袁荣霞, 方锐洁, 等. 郑氏提顶理筋手法结合润肠通便方对臀坐式骶尾椎骨折患者的临床疗效观察[J]. 中华中医药杂志, 2023, 38(10): 5087−5090. CHEN Z K, YUAN R X, FANG R J, et al. Clinical efficacy observation of ZHENGs’ manipulation of lifting the top and regulating the tendons combined with Runchang Tongbian Recipe in patients with buttock sitting sacrococcygeal fracture[J]. China Journal of Traditional Chinese Medicine and Pharmacy, 2023, 38(10): 5087−5090. (in Chinese).
[2] BARBER L A, KATSUURA Y, QURESHI S. Sacral fractures: A review[J]. HSS Journal, 2023, 19(2): 234-246. DOI: 10.1177/15563316221129607.
[3] BURGHARDT A J, LINK T M, MAJUMDAR S. High-resolution computed tomography for clinical imaging of bone microarchitecture[J]. Clinical Orthopaedics and Related Research, 2011, 469(8): 2179−2193. DOI: 10.1007/s11999-010-1766-x.
[4] BOOZ C, NÖSKE J, ALBRECHT M H, et al. Diagnostic accuracy of color-coded virtual noncalcium dual-energy CT for the assessment of bone marrow edema in sacral insufficiency fracture in comparison to MRI[J]. European Journal of Radiology, 2020, 129: 109046. DOI: 10.1016/j.ejrad.2020.109046.
[5] HAN I H, CHIN D K, KUH S U, et al. Magnetic resonance imaging findings of subsequent fractures after vertebroplasty[J]. Neurosurgery, 2009, 64(4): 740-744. DOI: 10.1227/01.NEU.0000339120.41053.F1.
[6] KAZAWA N. T2WI MRI and MRI-MDCT correlations of the osteoporotic vertebral compressive fractures[J]. European Journal of Radiology, 2012, 81(7): 1630−1636. DOI: 10.1016/j.ejrad.2011.04.052.
[7] AKISATO K, NISHIHARA R, OKAZAKI H, et al. Dual-energy CT of material decomposition analysis for detection with bone marrow edema in patients with vertebral compression fractures[J]. Academic radiology, 2020, 27(2): 227−232. DOI: 10.1016/j.acra.2019.02.015.
[8] PACHE G, KRAUSS B, STROHM P, et al. Dual-energy CT virtual noncalcium technique: Detecting posttraumatic bone marrow lesions—feasibility study[J]. Radiology, 2010, 256(2): 617-624. DOI: 10.1148/radiol.10091230.
[9] GOSANGI B, MANDELL J C, WEAVER M J, et al. Bone marrow edema at dual-energy CT: A game changer in the emergency department[J]. Radiographics, 2020, 40(3): 859−874. DOI: 10.1148/rg.2020190173.
[10] TIVNAN P, KALIAEV A, ANDERSON S W, et al. Utilization of a two-material decomposition from a single-source, dual-energy CT in acute traumatic vertebral fractures[J]. Frontiers in Radiology, 2023, 3: 1187449. DOI: 10.3389/fradi.2023.1187449.
[11] LI Z, CHEN X, FANG H, et al. Diagnostic accuracy of dual-energy CT for bone marrow edema in patients with acute knee injury: A systematic review and meta-analysis[J]. Journal of Orthopaedic Surgery and Research, 2023, 18(1): 826. DOI: 10.1186/s13018-023-04151-3.
[12] WALSTRA F E, HICKLE J, DUGGAN P, et al. Top-ten tips for dual-energy CT in MSK Radiology[J]. Seminars in Musculoskeletal Radiology, 2019, 23(4): 392−404. DOI: 10.1055/s-0039-1694756.
[13] 梁建超, 方义杰, 李文娟, 等. 双能量CT虚拟去骨图不同对比物质相对比值对膝关节创伤性骨髓水肿的诊断价值[J]. 中华放射学杂志, 2018, 52(1): 41−45. DOI: 10.3760/cma.j.issn.1005-1201.2018.01.009. LIANG J C, FANG Y J, LI W J, et al. Diagnostic value of different related contrast material in dual-energy CT virtual noncalcium for detecting traumatic bone marrow edema in knee joint[J]. Chinese Journal of Radiology, 2018, 52(1): 41−45. DOI: 10.3760/cma.j.issn.1005-1201.2018.01.009. (in Chinese).
[14] 孔玲玲, 徐驰杰, 赵旻月, 等. 双能量CT虚拟单能量成像在鉴别脊柱急慢性压缩骨折中的应用价值[J]. CT理论与应用研究(中英文), 2021, 30(2): 209−216. DOI: 10.15953/j.1004-4140.2021.30.02.08. KONG L L, XU C J, ZHAO M Y, et al. The application value of dual-energy CT virtual monoenergetic imaging in the differential diagnosis of acute and chronic spinal compression fractures[J]. CT Theory and Applications, 2021, 30(2): 209−216. DOI: 10.15953/j.1004-4140.2021.30.02.08. (in Chinese).
[15] MENNEN A H M, BLOKLAND A S, MAAS M, et al. Imaging of pelvic ring fractures in older adults and its clinical implications-a systematic review[J]. Osteoporosis International, 2023, 34(9): 1549−1559. DOI: 10.1007/s00198-023-06812-9.
[16] GRUNZ J P, SAILER L, LANG P, et al. Dual-energy CT in sacral fragility fractures: Defining a cut-off Hounsfield unit value for the presence of traumatic bone marrow edema in patients with osteoporosis[J]. BMC Musculoskeletal Disorders, 2022, 23(1): 724. DOI: 10.1186/s12891-022-05690-2.
[17] PALM H G, LANG P, HACKENBROCH C, et al. Dual-energy CT as an innovative method for diagnosing fragility fractures of the pelvic ring: A retrospective comparison with MRI as the gold standard[J]. Archives of Orthopaedic and Trauma Surgery, 2020, 140(4): 473−480. DOI: 10.1007/s00402-019-03283-8.
[18] 中华医学会放射学分会, 中国医师协会放射医师分会, 安徽省影像临床医学研究中心. 能量CT临床应用中国专家共识[J]. 中华放射学杂志, 2022, 56(5): 476−487. DOI: 10.3760/cma.j.cn112149-20220118-00051. Chinese Society of Radiology of Chinese Medical Association, Chinese Radiologist Association, Research Center of Clinical Medical Imaging of Anhui Province. China expert consensus on clinical application of multi-energy CT[J]. Chinese Journal of Radiology, 2022, 56(5): 476−487. DOI: 10.3760/cma.j.cn112149-20220118-00051. (in Chinese).
[19] MAŁKIEWICZ A, DZIEDZIC M. Bone marrow reconversion: Imaging of physiological changes in bone marrow[J]. Polish Journal of Radiology, 2012, 77(4): 45−50. DOI: 10.12659/pjr.883628.
[20] KELLOCK T T, NICOLAOU S, KIM S S Y, et al. Detection of bone marrow edema in nondisplaced hip fractures: Utility of a virtual noncalcium dual-energy CT application[J]. Radiology, 2017, 284(3): 922. DOI: 10.1148/radiol.2017161063.
[21] SON W, PARK C, JEONG H S, et al. Bone marrow edema in non-traumatic hip: High accuracy of dual-energy CT with water-hydroxyapatite decomposition imaging[J]. European Radiology, 2020, 30(4): 2191−2198. DOI: 10.1007/s00330-019-06519-8.
[22] CAVALLARO M, D'ANGELO T, ALBRECHT M H, et al. Comprehensive comparison of dual-energy computed tomography and magnetic resonance imaging for the assessment of bone marrow edema and fracture lines in acute vertebral fractures[J]. European Radiology, 2022, 32(1): 561−571. DOI: 10.1007/s00330-021-08081-8.
[23] 左天姿, 陈英敏, 贾秀川, 等. 双能CT虚拟去钙技术显示非创伤性股骨头坏死骨髓水肿的研究[J]. 实用放射学杂志, 2021, 37(4): 624−627, 632. DOI: 10.3969/j.issn.1002-1671.2021.04.027. ZUO T Z, CHEN Y M, JIA X C, et al. Study on bone marrow edema of non-traumatic femoral head necrosis via dual-energy CT virtual noncalcium[J]. Journal of Practical Radiology, 2021, 37(4): 624−627, 632. DOI: 10.3969/j.issn.1002-1671.2021.04.027. (in Chinese).
[24] JANG S W, CHUNG B M, KIM W T, et al. Nondisplaced fractures on hip CT: Added value of dual-energy CT virtual non-calcium imaging for detection of bone marrow edema using visual and quantitative analyses[J]. Acta Radiologica, 2019, 60(11): 1465−1473. DOI: 10.1177/0284185119831690.
[25] LI M, QU Y, SONG B. Meta-analysis of dual-energy computed tomography virtual non-calcium imaging to detect bone marrow edema[J]. European Journal of Radiology, 2017, 95: 124−129. DOI: 10.1016/j.ejrad.2017.08.005.
-
期刊类型引用(3)
1. 刘海燕,邱晓晖,章辉庆,锁咏梅,王超,王亚丽. 能谱CT单能量成像对结直肠癌供血动脉图像质量及辐射剂量的影响. 中国CT和MRI杂志. 2025(01): 159-161 .  百度学术
百度学术
2. 叶雄鑫,刘元芬,汤博荣,陈依林,郑莞怡,薛莉薇,张孝勇. 深度学习图像重建和能谱成像在低对比剂流速胸主动脉CTA中的价值. CT理论与应用研究. 2024(06): 683-691 . 本站查看
3. 何亮,唐彩银,张继,田为中,朱鹏飞. 能谱CT金属伪影抑制算法在胸部穿刺活检中的应用价值. 中国CT和MRI杂志. 2023(11): 50-52 . 百度学术
其他类型引用(2)



计量
- 文章访问数: 130
- HTML全文浏览量: 38
- PDF下载量: 15
- 被引次数: 5
