
Study on the Nomogram Model Based on Dual-energy Computed Tomography for Predicting Lymph Node Metastasis in Papillary Thyroid Carcinoma
-
摘要:
目的:探讨基于双能CT定量参数结合淋巴结临床信息构建列线图模型对转移淋巴结与非转移淋巴结的鉴别作用。方法:回顾性收集2021年至2023年甲状腺乳头状癌的患者103例,术前患者均行颈部双能量增强CT,结合术后病理结果,将淋巴结分为转移淋巴结与非转移淋巴结两组,其中转移淋巴结105粒,非转移淋巴结136粒。分析两组淋巴结的动脉期碘浓度(IC)、形状、短径、边缘、强化程度、囊变、钙化、动脉期强化方式、甲状腺结节包膜完整度。经过单因素和多因素Logistic分析,得到判断淋巴结转移的独立风险因素,基于此结果构建模型,并绘制列线图及校准曲线。结果:多因素二元Logistic回归结果显示,淋巴结动脉期碘浓度≥2.6 mg/mL、动脉期强化程度明显、动脉期强化方式不均匀、短径≥10 mm、边缘不清楚、形状不规则、甲状腺结节包膜不完整为预测淋巴结是否为转移的淋巴结的独立危险因素。列线图AUC为 0.996(95% CI 0.993~0.996),截断值 0.09,灵敏度 99%,特异度95%。结论:基于双能CT构建的列线图,对术前评估甲状腺乳头状癌患者的淋巴结有无转移,可以辅助手术医生在术前制定手术方案。
Abstract:Objective: This study aimed to evaluate the effectiveness of a nomogram model based on dual-energy computed tomography (CT) quantitative parameters combined with clinical information for distinguishing metastatic from non-metastatic lymph nodes in patients with papillary thyroid carcinoma (PTC). Methods: This retrospective study was conducted in 103 patients with PTC from 2021 to 2023. Each patient underwent preoperative neck dual-energy-enhanced CT, and postoperative pathological results revealed 105 lymph nodes as metastatic and 136 as non-metastatic. Parameters, such as iodine concentration (IC), in the arterial phase, lymph node shape, short diameter, margin, degree of enhancement, cystic changes, calcification, arterial phase enhancement pattern, and thyroid nodule capsule integrity were analyzed. Univariate and multivariate logistic regression analyses identified independent risk factors for lymph node metastasis that were incorporated into the nomogram. The model performance was evaluated using a calibration curve. Results: Multivariate logistic regression analysis showed IC in the arterial phase ≥ 2.6 mg/mL, significant arterial phase enhancement, uneven arterial phase enhancement pattern, diameter ≥10 mm, unclear margins, irregular shape, and incomplete thyroid nodule capsule as independent risk factors for lymph node metastasis. The nomogram achieved an area under the curve of 0.996 (95% confidence interval (CI); 0.993~0.996) with a cutoff value of 0.09, sensitivity of 99%, and specificity of 95%. Conclusion: The dual-energy CT-based nomogram demonstrated a significant clinical value in the preoperative assessment of lymph node metastasis in patients with PTC, potentially assisting in the formulation of individualized surgical plans.
-
Keywords:
- dual-energy CT /
- thyroid tumors /
- nomogram /
- cervical lymph node metastasis
-
甲状腺乳头状癌(papillary thyroid carcinoma,PTC)的发病率在过去几十年中处于上升状态[1],其在早期就容易发生转移,以中央区淋巴结多见[2]。颈部淋巴结转移会影响医生手术方案的制定,对患者的预后产生影响[3]。中国临床肿瘤协会指南指出:细针穿刺(fine needle aspiration,FNA)证实有转移的淋巴结,则需进行侧颈淋巴结清扫[4]。因此术前无创、准确评估有无侧颈淋巴结转移对其临床医生选择手术方式非常重要。
对于临床怀疑淋巴结转移的患者,常规指南均推荐做甲状腺超声和颈部增强CT[4],颈部淋巴结体积大小不一,发生转移时其形态各有差异,常规CT图像特征对转移淋巴结的诊断准确度和敏感度较超声低[5-6]。双能CT(dual-energy CT,DECT)可以通过多种定量参数对转移淋巴结进行诊断[7-10],常见有通过测量转移淋巴结的碘浓度来对其进行区分[11]。
本研究中将常规CT图像特征与双能量CT定量参数结合建立诊断模型,提高模型的准确性,可辅助鉴别淋巴结的良恶性。
1. 资料与方法
1.1 研究对象
回顾性分析收集2021年至2023年甲状腺乳头状癌的患者103例,其中男40例,女63例;年龄19~68岁。术前患者均行颈部双能量增强CT,结合术后病理结果,将淋巴结分为转移淋巴结与非转移淋巴结两组,其中转移淋巴结105粒,非转移淋巴结136粒。
纳入标准:①术前一周行双能CT扫描;②图像无吞咽伪影;③术前超声怀疑有淋巴结转移。排除标准:①患有其它肿瘤;②图像有明显的吞咽伪影及对比剂伪影。
1.2 双能CT扫描方法
采用Siemens SOMATOM Force第3代双源CT。扫描参数:使用自动管电流调制技术,开启CareDose4D,参考管电流560 mAs,扫描层厚5 mm,螺距0.7,转速1 s/r,准直2 mm×192 mm×0.6 mm。A球管电压90 kV、B球管电压Sn 150 kV,双臂放于身体两侧,扫描范围自颅底到主动脉弓,通过右肘正中静脉注射对比剂50~60 mL,碘浓度370 mg/mL,流速3 mL/s,跟注30 mL生理盐水。
采用经验法动脉期延迟27 s,静脉期延迟35 s。
1.3 淋巴结病理对照
由两名高年资放射科医师根据Reza等[12]提出的淋巴结影像与病理亚区对照方法,对短径≥5 mm的淋巴结进行标记,记录淋巴结的位置。
术前由临床医生对清扫的淋巴结进行分区,术后参照病理结果记录淋巴结的病理类型[13]。
1.4 双能CT数据处理及淋巴结图像特征收集
将所有数据导入Siemens Syngovia工作站进行后处理,使用虚拟平扫后处理获得动脉期碘图。
选择淋巴结最大横截面的层面,在淋巴结明显强化的地方绘制(region of interest,ROI),尽量避开病灶坏死、钙化区,测量淋巴结的动脉期IC。测量3次取平均值。记录两组淋巴结的动脉期IC、形状、短径、边缘、强化程度、囊变、钙化、动脉期强化方式、甲状腺结节包膜完整度。
1.5 统计学方法预测模型的建立与验证
统计学方法:采用SPSS 26.0和R(version4.3.1)进行数据统计,GraphPadprism 10.0进行图像绘制。
使用独立样本t检验比较转移淋巴结组与非转移淋巴结组间的数据差异;采用K-S检验分析计量数据的分布,如不符合正态分布,则使用Mann-Whitney U检验比较两组间差异[14]。
以单因素分析中P<0.05的变量作为多因素Logistic回归的分析变量,将其纳入模型中并绘制列线图。绘制(receiver operating characteristic curve,ROC)曲线,计算列线图的截断值和曲线下面积(area under the curve,AUC)以确定列线图的诊断效能。通过校准曲线评估列线图的准确性。
模型验证:内部验证采用Bootstrap方法,从原始数据集中随机抽取样本大小与原数据集相同的数据,进行
1000 次Bootstrap重复,并进行决策曲线分析,来评估验证队列的列线图收益。2. 结果
2.1 双能CT图像特征
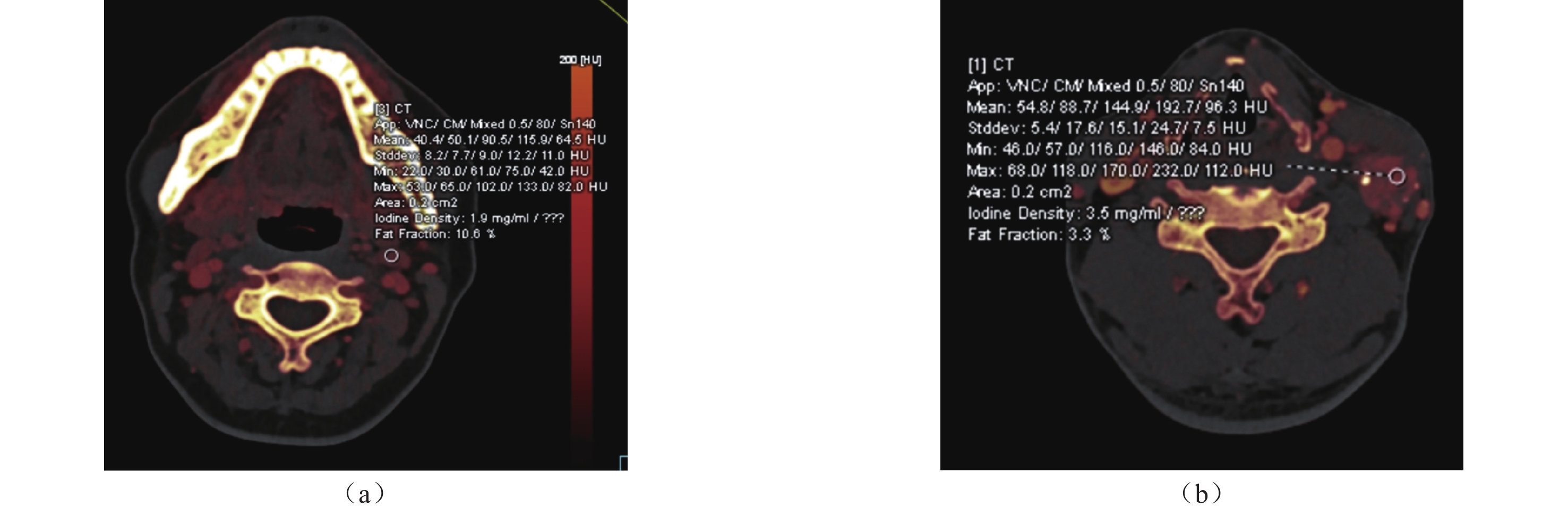
转移组与非转移组间的动脉期碘浓度、形状、短径、边缘、动脉期强化方式、强化程度,结节包膜完整度,囊变、钙化、差异有统计学意义(图1和表1)。
![]() 图 1 (a)患者女29岁,颈部非转移淋巴结,动脉期碘浓度1.9 mg/mL,形状规则,短径<10 mm ,边缘清楚,轻度均匀强化,甲状腺结节包膜完整;(b)患者女55岁,颈部转移淋巴结,动脉期碘浓度3.5 mg/mL,形状不规则,短径>10 mm,边缘不清楚,明显不均匀强化,甲状腺结节包膜不完整Figure 1. (a) A 29-year-old woman with non-metastatic cervical lymph nodes. The iodine concentration during the arterial phase is 1.9 mg/mL. The lymph nodes have a regular shape, axis<10 mm, clear margins, mild and homogeneous enhancement, and an intact thyroid nodule capsule. (b) A 55-year-old woman with metastatic cervical lymph nodes. The iodine concentration during the arterial phase is 3.5 mg/mL. The lymph nodes have an irregular shape, axis>10 mm, unclear margins, marked heterogeneous enhancement, and incomplete thyroid nodule capsule表 1 转移淋巴结与非转移淋巴结CT图像特征及DECT定量参数动脉期碘浓度的比较Table 1. Comparison of CT image features and DECT quantitative parameters (arterial phase iodine concentration) between metastatic and non-metastatic lymph nodes
图 1 (a)患者女29岁,颈部非转移淋巴结,动脉期碘浓度1.9 mg/mL,形状规则,短径<10 mm ,边缘清楚,轻度均匀强化,甲状腺结节包膜完整;(b)患者女55岁,颈部转移淋巴结,动脉期碘浓度3.5 mg/mL,形状不规则,短径>10 mm,边缘不清楚,明显不均匀强化,甲状腺结节包膜不完整Figure 1. (a) A 29-year-old woman with non-metastatic cervical lymph nodes. The iodine concentration during the arterial phase is 1.9 mg/mL. The lymph nodes have a regular shape, axis<10 mm, clear margins, mild and homogeneous enhancement, and an intact thyroid nodule capsule. (b) A 55-year-old woman with metastatic cervical lymph nodes. The iodine concentration during the arterial phase is 3.5 mg/mL. The lymph nodes have an irregular shape, axis>10 mm, unclear margins, marked heterogeneous enhancement, and incomplete thyroid nodule capsule表 1 转移淋巴结与非转移淋巴结CT图像特征及DECT定量参数动脉期碘浓度的比较Table 1. Comparison of CT image features and DECT quantitative parameters (arterial phase iodine concentration) between metastatic and non-metastatic lymph nodes分组 数量/个 动脉期碘浓度
/(mg/mL)形状 短径/mm 边缘 强化程度 强化方式 囊变 钙化 结节包膜完整度 ≥2.6 <2.6 规则 不规则 ≥10 <10 清楚 不清楚 轻中度 明显 不均匀 均匀 无 有 无 有 完整 不完整 转移 105 98 7 41 64 68 37 57 48 30 75 73 32 97 8 83 22 101 4 非转移 136 15 121 133 3 27 109 135 1 133 33 132 4 136 0 136 0 53 83 P <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 2.2 列线图的建立与评估
采用ROC曲线计算动脉期碘浓度IC的截断值为2.6 mg/mL,将其转换为二分类变量,经单因素逻辑回归分析,排除囊变,钙化,经多因素逻辑回归分析,动脉期碘浓度、形状、短径、边缘、动脉期强化方式、强化程度,结节包膜完整度是预测淋巴结是否为转移淋巴结的危险因素,其OR值分别为251.6、144.9、12.7、21.4、3.2、32.4和27.1(表2),方差膨胀因子均<10,相应的容差>0.1,表示变量之间共线性较小。
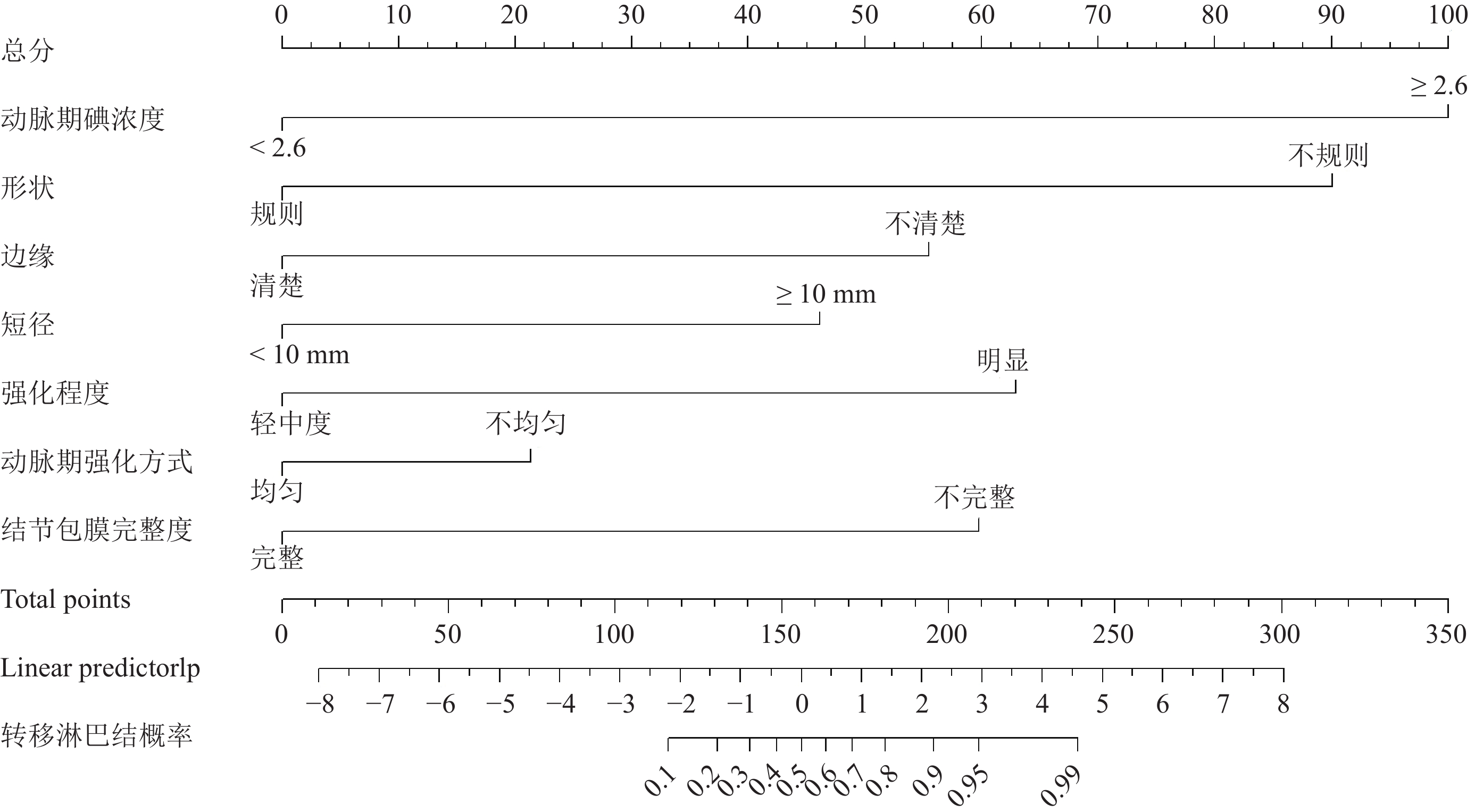
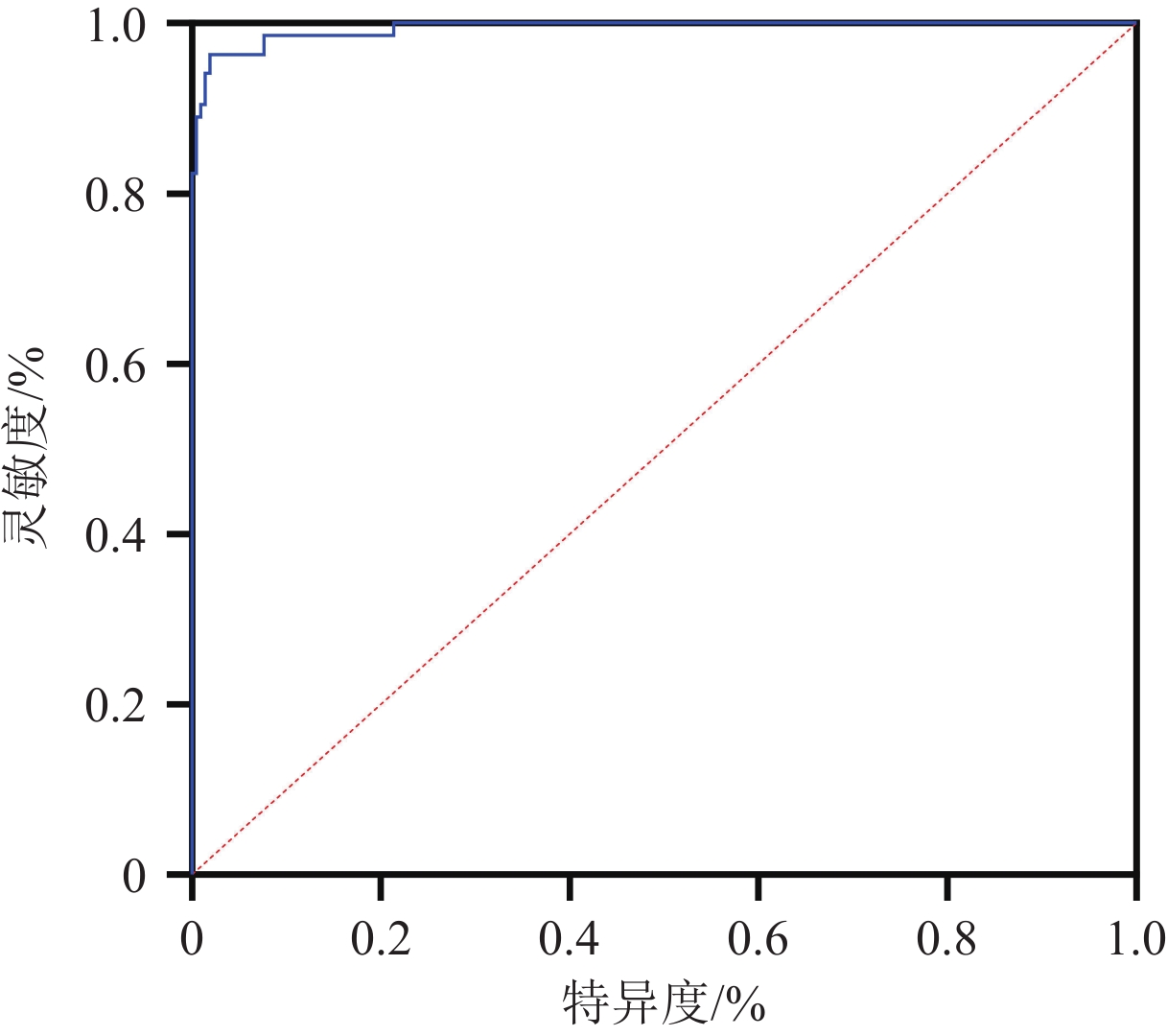
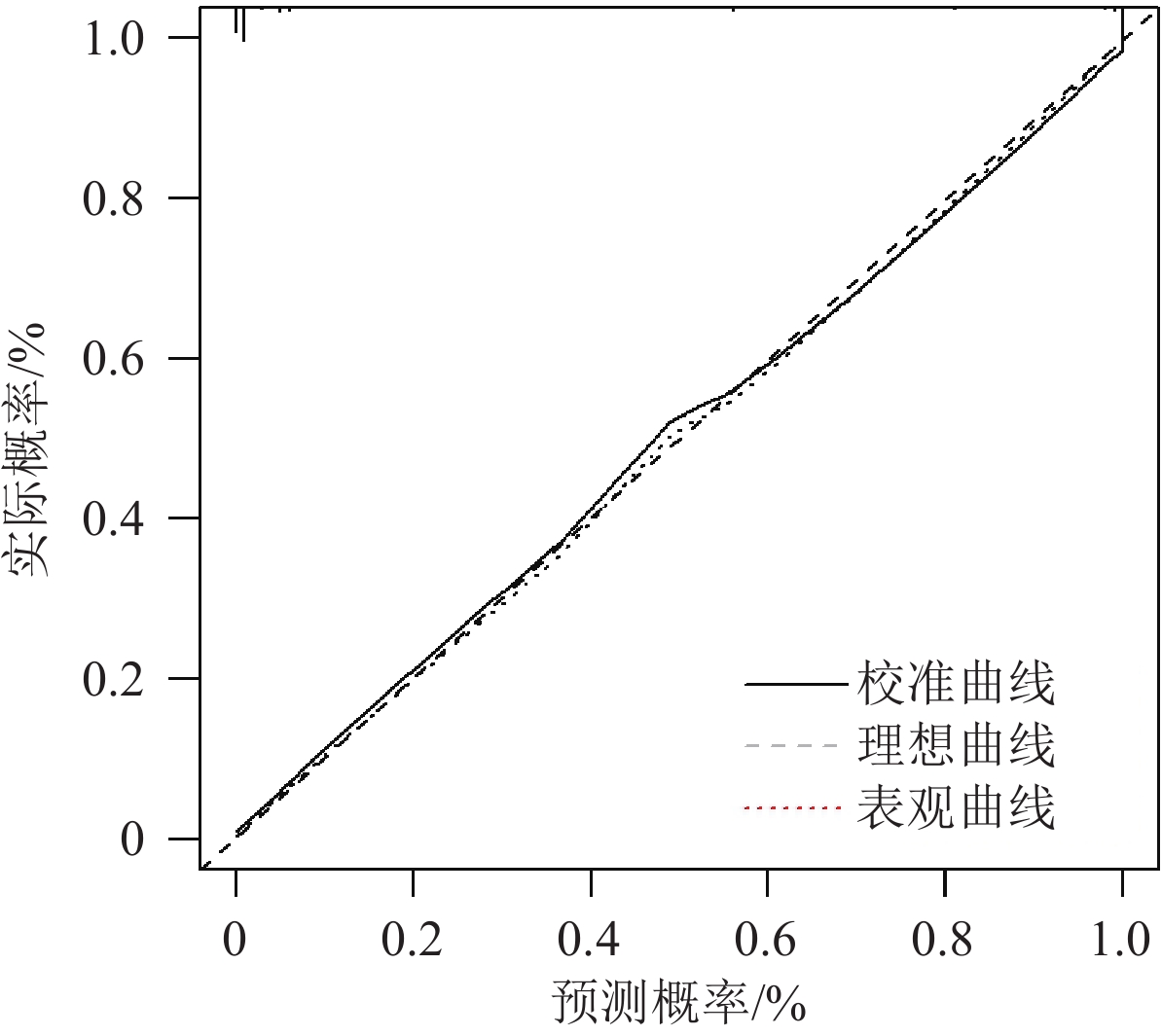
表 2 多因素logistic回归分析预测乳头状癌患者淋巴结转移的独立危险因素Table 2. Multivariate logistic regression analysis to predict independent risk factors for lymph node metastasis in patients with papillary thyroid carcinoma变量 回归系数 标准误 Waldχ值 方差膨胀因子 容差 P OR(95% CI) 动脉期碘浓度 5.528 1.023 12.636 2.176 0.460 <0.001 251.6(11.5~ 5491.6 )强化方式 4.157 1.314 10.016 2.175 0.460 <0.001 3.2(0.3~30.9) 强化程度 2.339 1.087 4.635 2.382 0.420 <0.001 32.4(2.0~511.7) 短径 1.867 1.278 2.132 1.439 0.695 0.052 12.7(0.6~240.5) 形状 4.976 2.281 2.184 2.139 0.451 0.039 144.9(0.4~ 50694.2 )结节包膜完整度 3.039 0.979 9.631 2.175 0.176 <0.001 27.1(3.0~240.2) 边缘 2.265 1.505 2.265 1.746 0.573 0.011 21.4(1.0~437.2) 由以上因素构建的列线图(图2),列线图AUC为 0.996(95% CI 0.993~0.996),截断值 0.09,灵敏度 99%,特异度95%(图3)。校准曲线表示淋巴结为转移的概率与实际接近,平均绝对误差0.011(图4)。H-L检验结果P=0.998,提示该模型不存在过度拟合[14]。
![]() 图 2 PTC患者淋巴结转移发生概率的列线图Figure 2. Nomogram predicting the probability of lymph node metastasis in patients with PTC
图 2 PTC患者淋巴结转移发生概率的列线图Figure 2. Nomogram predicting the probability of lymph node metastasis in patients with PTC![]() 图 3 PTC患者淋巴结转移发生概率的列线图的ROC曲线,曲线下面积为0.996Figure 3. ROC curve of the nomogram predicting the probability of lymph node metastasis in patients with PTC, with an AUC of 0.996
图 3 PTC患者淋巴结转移发生概率的列线图的ROC曲线,曲线下面积为0.996Figure 3. ROC curve of the nomogram predicting the probability of lymph node metastasis in patients with PTC, with an AUC of 0.9962.3 列线图的验证
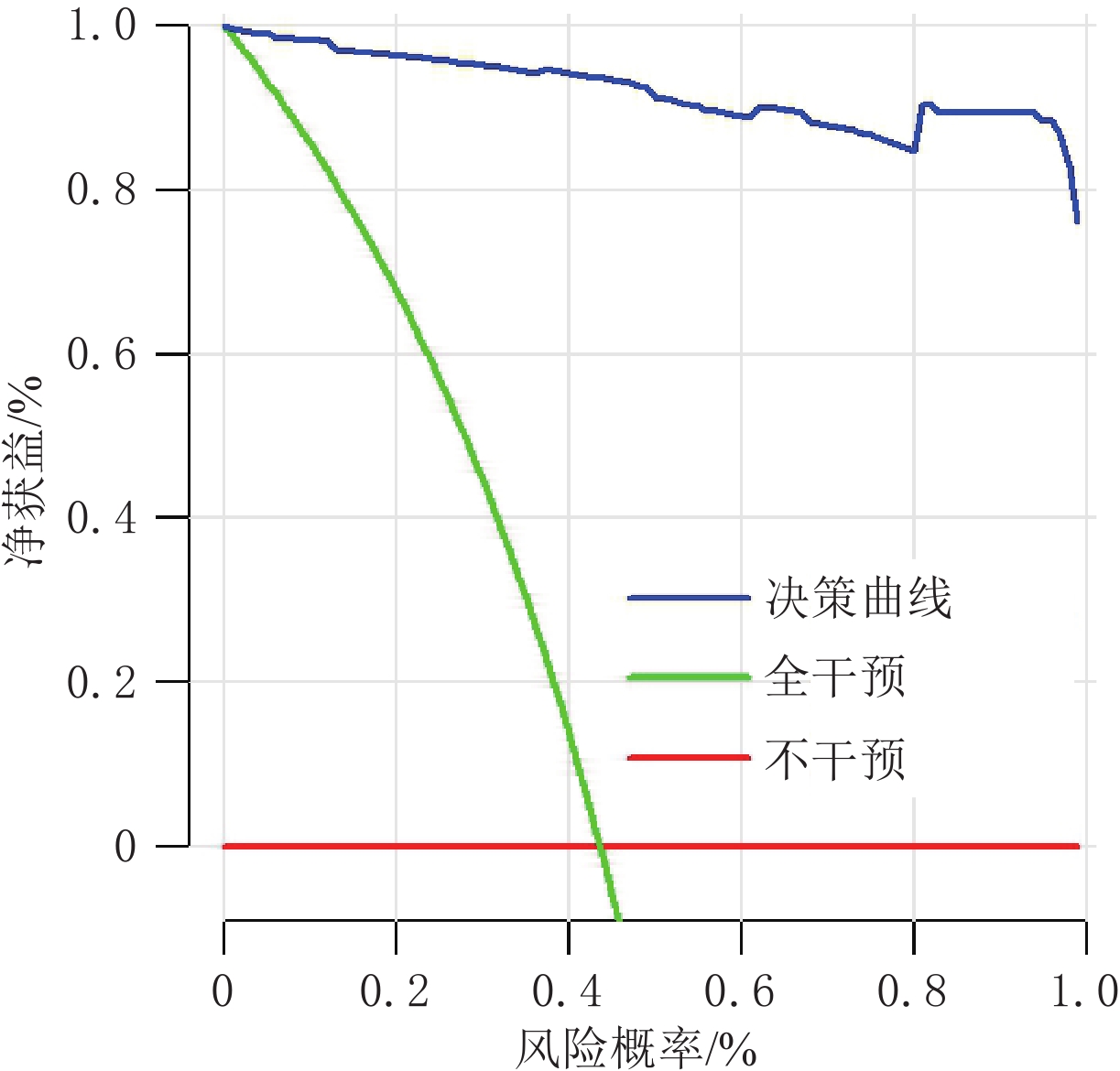
内部验证使用 Bootstrap 方法,进行
1000 次 Bootstrap,迭代之间的结果基本保持不变。该模型的决策曲线(图5)显示,如果术前评估怀疑是转移淋巴结,从而制定手术方案,比在术前没有进行淋巴结评估收益大。列线图截断值为0.09,将每个变量的得分相加,得到的列线图总分为287分。当阈值大于0.09时,该淋巴结为转移淋巴结的可能性大。
3. 讨论
本研究通过分析淋巴结的双能CT的图像特征及淋巴结动脉期碘浓度,预测淋巴结是否有转移,从而帮助临床医生制定手术方案。
本研究有3个主要发现。①双能CT图像特征:动脉期碘浓度、形状、短径、边缘、动脉期强化方式、强化程度,结节包膜完整度是预测转移淋巴结的独立风险因素。②基于以上7个特征构建的列线图AUC值为0.996,表明其预测能力较强。③列线图总分>287分的淋巴结为转移淋巴结的可能性大。
甲状腺乳头状癌被膜外侵犯,与PTC术后复发及区域淋巴结转移密切相关[15],CT图像上甲状腺结节包膜完整度与发生ETE有密切的相关性[16]。本研究显示PTC包膜不完整,其临近区域的淋巴结更容易发生转移。淋巴结CT图像特征形状、短径、边缘、动脉期强化方式、强化程度,囊变、钙化被广泛用于鉴别转移与非转移淋巴结[9]。本研究中转移淋巴结与非转移淋巴结在图像特征上有一定程度的差异,淋巴结形状不规则、边界不清楚、短径≥10 mm,则越倾向于转移淋巴结。转移淋巴结会出现不均匀明显强化,这与其内的血管床分布增多有关[17],其内的新生血管增多,从而导致转移淋巴结动脉期碘浓度增高[18]。
本研究中转移淋巴结的动脉期碘浓度高于非转移淋巴结,与闵蕊等[19]的研究一致。不同位置转移淋巴结的碘浓度不完全相同,我们推测这可能与肿瘤在淋巴结中的发育程度有关。
传统Logistic回归模型,可以预测疾病的危险因素,而列线图更加直观的展现出不同风险因素对结局的影响,目前国内所做的研究多是将淋巴结的影像组学特征加入列线图中,来提高其诊断效能[7]。相比于影像组学,常规CT图像特征更容易获取,结合双能量CT定量参数构建的模型诊断性更高,本研究构建的列线图训练组的AUC为0.996,因此可以辅助临床医生制定个性化手术方案,若所选择淋巴结的列线图得分小于287分,则不需要进行术中冰冻,从而减少患者的手术范围。
本研究的局限性。①本次研究为单中心研究,还需要对模型进行外部数据验证,由于纳入人数较少,存在潜在的选择偏倚;②本次研究未纳入5 mm以下的淋巴结,而实际工作中5 mm以下的淋巴结也有转移淋巴结,这会在以后的研究中进一步分析。
尽管存在以上局限性,但本研究选用参数容易获得,该列线图可以术前对淋巴结性质进行区分,对高风险淋巴结在术中进行冰冻诊断,从而减少转移淋巴结的漏诊。因此该列线图可以辅助临床医师制定个性化手术方案。
-
![]()
图 1 (a)患者女29岁,颈部非转移淋巴结,动脉期碘浓度1.9 mg/mL,形状规则,短径<10 mm ,边缘清楚,轻度均匀强化,甲状腺结节包膜完整;(b)患者女55岁,颈部转移淋巴结,动脉期碘浓度3.5 mg/mL,形状不规则,短径>10 mm,边缘不清楚,明显不均匀强化,甲状腺结节包膜不完整
Figure 1. (a) A 29-year-old woman with non-metastatic cervical lymph nodes. The iodine concentration during the arterial phase is 1.9 mg/mL. The lymph nodes have a regular shape, axis<10 mm, clear margins, mild and homogeneous enhancement, and an intact thyroid nodule capsule. (b) A 55-year-old woman with metastatic cervical lymph nodes. The iodine concentration during the arterial phase is 3.5 mg/mL. The lymph nodes have an irregular shape, axis>10 mm, unclear margins, marked heterogeneous enhancement, and incomplete thyroid nodule capsule
![]()
图 2 PTC患者淋巴结转移发生概率的列线图
Figure 2. Nomogram predicting the probability of lymph node metastasis in patients with PTC
![]()
图 3 PTC患者淋巴结转移发生概率的列线图的ROC曲线,曲线下面积为0.996
Figure 3. ROC curve of the nomogram predicting the probability of lymph node metastasis in patients with PTC, with an AUC of 0.996
表 1 转移淋巴结与非转移淋巴结CT图像特征及DECT定量参数动脉期碘浓度的比较
Table 1 Comparison of CT image features and DECT quantitative parameters (arterial phase iodine concentration) between metastatic and non-metastatic lymph nodes
分组 数量/个 动脉期碘浓度
/(mg/mL)形状 短径/mm 边缘 强化程度 强化方式 囊变 钙化 结节包膜完整度 ≥2.6 <2.6 规则 不规则 ≥10 <10 清楚 不清楚 轻中度 明显 不均匀 均匀 无 有 无 有 完整 不完整 转移 105 98 7 41 64 68 37 57 48 30 75 73 32 97 8 83 22 101 4 非转移 136 15 121 133 3 27 109 135 1 133 33 132 4 136 0 136 0 53 83 P <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 多因素logistic回归分析预测乳头状癌患者淋巴结转移的独立危险因素
Table 2 Multivariate logistic regression analysis to predict independent risk factors for lymph node metastasis in patients with papillary thyroid carcinoma
变量 回归系数 标准误 Waldχ值 方差膨胀因子 容差 P OR(95% CI) 动脉期碘浓度 5.528 1.023 12.636 2.176 0.460 <0.001 251.6(11.5~ 5491.6 )强化方式 4.157 1.314 10.016 2.175 0.460 <0.001 3.2(0.3~30.9) 强化程度 2.339 1.087 4.635 2.382 0.420 <0.001 32.4(2.0~511.7) 短径 1.867 1.278 2.132 1.439 0.695 0.052 12.7(0.6~240.5) 形状 4.976 2.281 2.184 2.139 0.451 0.039 144.9(0.4~ 50694.2 )结节包膜完整度 3.039 0.979 9.631 2.175 0.176 <0.001 27.1(3.0~240.2) 边缘 2.265 1.505 2.265 1.746 0.573 0.011 21.4(1.0~437.2)
下载: 导出CSV
-
[1] La VECCHIA C, NEGRI E. The thyroid cancer epidemic overdiagnosis or a real increase?[J]. Nature Reviews Endocrinology, 2017, 13(6): 318-319. DOI: 10.1038/nrendo.2017.53.
[2] 李治, 屈新才, 程波, 等. 乳头状甲状腺癌淋巴结转移特点与中央组淋巴结清扫的临床意义[J]. 中华外科杂志, 2008, 46 (18): 1407-1409. DOI: 10.3321/j.issn:0529-5815.2008.18.015. LI Z, QU X C, CHENG B, et al. The characteristics of papillary thyroid cancer lymph node metastasis and the clinical significance of central region cervical lymph node dissection[J]. Chinese Journal of Surgery 2008 SEP, 46(18): 1407-1409. DOI: 10.3321/j.issn:0529-5815.2008.18.015. (in Chinese).
[3] 蔡卉珠, 黄泽浩, 黄樱城, 等. 甲状腺乳头状癌侧颈淋巴结转移的诊疗现状[J]. 中华耳鼻咽喉头颈外科杂志, 2023, 58 (4): 398-402. DOI: 10.3760/cma.j.cn115330-20221018-00617. CAI H Z, HUANG Z H, HUANG Y C, et al. Update on diagnosis and treatment of lateral cervical lymph node metastasis in papillary thyroid carcinoma[J]. Chinese Journal of Otorhinolaryngology Head and Neck Surgery 2023, 58(4): 398-402. DOI: 10.3760/cma.j.cn115330-20221018-00617. (in Chinese).
[4] Chinese Society of Clinical Oncology (CSCO) diagnosis and treatment guidelines for persistent/recurrent and metastatic differentiated thyroid cancer 2018 (English version)[J]. Chinese Journal of Cancer Research, 2019, 31 (1): 99-116. DOI: 10.21147/j.issn.1000-9604.2019.01.06.
[5] 赵佳航, 张艳, 罗渝昆, 等. 超声与CT检查在诊断甲状腺乳头状癌颈部淋巴结转移中的对比分析[J]. 中国医学科学院学报, 2022, 44 (1): 65-71. DOI: 10.3881/j.issn.1000-503X.14135. ZHAO J H, ZHANG Y, LUO Y K, et al. Comparison between Ultra sonography and CT in Diagnosis of Cervical Lymph Node Metastasis of Papillary Thyroid Carcinoma[J]. Acta Academiae Medicinae Sinicae, 2022 Feb;44(1): 65-71. DOI: 10.3881/j.issn.1000-503X.14135. (in Chinese).
[6] 金弋人, 韩丹, 赵雯, 等. 双源CT平扫碘值联合TSH诊断良恶性甲状腺结节的价值[J]. 临床放射学杂志, 2018, 37(4): 591-595. [7] ZHOU Y, SU G Y, HU H, et al. Radiomics analysis of dual-energy CT-derived iodine maps for diagnosing metastatic cervical lymph nodes in patients with papillary thyroid cancer[J]. European Radiology, 2020, 30(11): 6251-6262. DOI: 10.1007/s00330-020-06866-x.
[8] LI F, HUANG F, LIU C, et al. Parameters of dual-energy CT for the differential diagnosis of thyroid nodules and the indirect prediction of lymph node metastasis in thyroid carcinoma: A retrospective diagnostic study[J]. Gland Surgery, 2022, 11(5): 913-926. DOI: 10.21037/gs-22-262.
[9] LIU X, OUYANG D, LI H, et al. Papillary thyroid cancer: Dual-energy spectral CT quantitative parameters for preoperative diagnosis of metastasis to the cervical lymph nodes[J]. Radiology, 2015, 275(1): 167-176. DOI: 10.1148/radiol.14140481.
[10] SEO D H, LEE S G, LEE H Y, et al. Lymph node metastasis-dependent molecular classification in papillary thyroid carcinoma defines aggressive metastatic outgrowth[J]. Clinical and Translational Medicine, 2023, 13(3): e1211. DOI: 10.1002/ctm2.1211.
[11] 黄益龙, 赵雯, 李浚利, 等. 双能CT碘图评估甲状腺微小乳头状癌颈淋巴结转移潜能的价值[J]. 中华放射学杂 志, 2019, 53 (8): 685-690. HUANG Y L, ZHAO W, LI J L, et al. Dual energy CT iodine image for evaluation of cervical lymph node metastatic potential in papillary thyroid microcarcinoma[J]. Chinese Journal of Radiology, 2019: 685-690. DOI: 10.3760/cma.j.issn.1005?1201.2019.08.005.(in Chinese).
[12] FORGHANI R, YU E, LEVENTAL M, et al. Imaging evaluation of lymphadenopathy and patterns of lymph node spread in head and neck cancer[J]. Expert Review of Anticancer Therapy, 2015, 15(2): 207-224. DOI: 10.1586/14737140.2015.978862.
[13] 高波, 孙海乔, 李晓会, 等. 双能CT对甲状腺乳头状癌颈部淋巴结转移的定量研究[J]. 中国CT和MRI杂志, 2023, 21 (3): 50-52. DOI: 10.3969/j.issn.1672-5131.2023.03.019. GAO B, SUN H Q, LI X H, et al. Quantitative research of dual-energy ct on cervical lymph node metastasis of thyroid papillary carcinoma[J]. Chinese Journal of CT and MRI, 2023, 21(03): 161. DOI: 10.3969/j.issn.1672-5131.2023.03.019.(in Chinese).
[14] 邹颖, 刘继华, 孙芳, 等. 基于双能CT的列线图预测cN1期甲状腺乳头状癌颈侧区淋巴结转移的可行性研究[J]. 中华放射学杂志, 2021, 55(7): 716-722. DOI: 10.3760/cma.j.cn112149-20200829-01039. ZOU Y, LIU J H, SUN F, et al. A feasibility study of predictive values of lateral cervical lymph node metastasis from cN1-stage papillary thyroid carcinoma based on dual-energy CT nomogram[J]. Chinese Journal of Radiology, 2021, 55(7): 716-722. DOI: 10.3760/cma.j.cn112149-20200829-01039. (in Chinese).
[15] CHUNG S R, BAEK J H, CHOI Y J, et al. Risk factors for metastasis in indeterminate lymph nodes in preoperative patients with thyroid cancer[J]. European Radiology, 2022, 32(6): 3863-3868. DOI: 10.1007/s00330-021-08478-5.
[16] 夏水伟, 林桂涵, 陈炜越, 等. 基于双能量CT的列线图在预测甲状腺乳头状癌腺外侵犯的价值[J]. 温州医科大学学报, 2023, 53(3): 221-226. DOI: 10.3969/j.issn.2095-9400.2023.03.008. [17] PARK J E, LEE J H, RYU K H, et al. Improved diagnostic accuracy using arterial phase CT for lateral cervical lymph node metastasis from papillary thyroid cancer[J]. American Journal of Neuroradiology, 2017, 38(4): 782-788. DOI: 10.3174/ajnr.A5054.
[18] 许晓泉, 周燕, 苏国义, 等. 联合CT图像特征和双能CT定量参数对甲状腺乳头状癌颈部淋巴结转移的诊断价值[J]. 中华放射学杂志, 2021, 55(2): 137-142. DOI: 10.3760/cma.j.cn112149-20200222-00226. XU X Q, ZHOU Y, SU G Y, et al. Integrating CT image features and quantitative dual-energy CT parameters for diagnosing metastatic lymph nodes from papillary thyroid carcinoma[J]. Chinese Journal of Radiology, 2021, 55(2): 137-142. DOI: 10.3760/cma.j.cn112149-20200222-00226. (in Chinese).
[19] 闵蕊, 韩丹, 赵雯, 等. 甲状腺乳头状癌灶双能量CT多参数预测中央组淋巴结转移[J]. 实用放射学杂志, 2020, 36(11): 1837-1840. DOI: 10.3969/j.issn.1002-1671.2020.11.033.
计量
- 文章访问数: 136
- HTML全文浏览量: 25
- PDF下载量: 11


