
Exploration of the Application Value of Dual Energy CT in the Diagnosis and Phase IIA Display of Talar Osteochondrial Injury
-
摘要:
目的:以MRI为参考标准,探讨双能CT对距骨骨软骨损伤及ⅡA期的诊断价值。方法:连续纳入2023年1月至2023年12月收入的因长期踝关节疼痛,经临床及MRI检查确诊为距骨骨软骨损伤的患者,共30例。患者于MRI检查后24h内完成了双能CT检查。医生A对30例MRI图像进行诊断及分期,分期依据Hepple等改良的MRI分期标准;医生B和医生C分别对DECT图像进行后处理生成虚拟去钙图像,然后独立双盲对图像进行视觉评估分期。医生D依照MRI结果,使用虚拟去钙技术对ⅡA期图像进行定量评估。以MRI为参考标准,统计医生B和C定性评估DECT的结果。医生D定量评估ⅡA期病灶区与对照组CT值是否有统计学差异。结果:医生B和医生C的DECT定性诊断的敏感性、特异性、准确性、阳性预测值、阴性预测值分别为84%,91%、89%、83%、90%和85%、89%、88%、83%和91%(Kappa值0.771和0.758)。医生B和C定性评估ⅡA期的敏感性、特异性分别为85%、94%和84%和93%(Kappa值0.807和0.801)。医生D定量诊断具有统计学差异,最佳截断值为-21.85HU(敏感性、特异性92%、98.9%)。结论:DECT 及虚拟去钙技术对距骨骨软骨损伤及ⅡA期的诊断具有较大的应用价值。
Abstract:Objective: To investigate the diagnostic value of dual-energy computed tomography (DECT) for Stage IIA talar osteochondral injuries, with magnetic resonance imaging (MRI) as the reference standard. Methods: Thirty consecutive patients admitted to the orthopedics department of our hospital from January 2023 to December 2023, with long-term ankle pain and diagnosed with an osteochondral lesion of the talus through clinical and MRI examinations, were enrolled. DECT was performed on the patients within 24 hours after the MRI examination. Doctor A diagnosed and staged the 30 MRI images based on the modified MRI staging criteria by Hepple et al. Doctors B and C, independently and blindly, performed visual assessment and staging of the DECT images after post-processing to generate virtual non-calcium images. Doctor D quantitatively assessed images from the patients with a Stage IIA injury using the virtual non-calcium technique, based on the MRI results. With MRI as the reference standard, the qualitative assessments of DECT were statistically analyzed by Doctors B and C. Doctor D quantitatively assessed whether there was a statistical difference in CT attenuation values in the lesion area in patients with Stage IIA injuries compared with the controls. Results: The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of DECT qualitative diagnosis by Doctors B and C were 84%, 91%, 89%, 83%, and 90% and 85%, 89%, 88%, 83%, and 91%, respectively (Kappa values of 0.771 and 0.758). The sensitivity and specificity of qualitative assessment of Stage IIA lesions by Doctors B and C were 85% and 94%, and 84% and 93%, respectively (Kappa values of 0.807 and 0.801). The quantitative diagnosis by Doctor D showed a statistical difference, with an optimal cutoff value of −21.85 HU (sensitivity and specificity: 92% and 98.9%). Conclusion: DECT and virtual non-calcium imaging techniques have significant diagnostic value for patients with Stage IIA talar osteochondral injuries.
-
Keywords:
- dual-energy CT /
- virtual non-calcium technique /
- OLT /
- bone marrow edema /
- Phase IIA
-
距骨骨软骨损伤(osteochondral lesion of talus,OLT)系发生在距骨穹隆,累及软骨和软骨下骨的病变,是踝关节最常见的损伤之一。临床上可无症状,或者表现为脚踝疼痛,活动时加重,疼痛位置与OLT位置没有必然关系。OLT病情进展的危险因素直接影响临床治疗手段,危险因素包括MRI上损伤深度、关节软骨下囊肿形成、骨髓水肿程度[1]。通常采用Hepple等[2]改良的MRI分期标准如下,Ⅰ期:关节软骨损伤;ⅡA期:关节软骨损伤伴软骨下隐匿性骨折,MRI显示周围骨髓水肿;ⅡB期关节软骨损伤伴软骨下隐匿性骨折,不伴周围骨髓水肿;Ⅲ期骨软骨块分离,无移位;Ⅳ期骨软骨块分离,有移位;Ⅴ期关节软骨下囊肿形成。由于MRI分辨率较高,能显示软骨及软骨下骨髓水肿等改变,使MRI成为诊断OLT的最常用的影像手段。MRI上发现骨髓水肿,是早期诊断OLT和疗效评估的依据。但MRI检查时间长,层间距较厚,禁忌症多,并且对OLT骨质囊变及骨折的显示不如CT。双能CT(dual-energy CT,DECT)兼备常规CT的优势,不仅辐射剂量较常规CT小,更重要的是能显示脊柱及四肢骨的骨髓水肿[3]。DECT虚拟去钙(virtual non-calcium,VNCA)技术利用两种不同的X射线能谱采集两组数据集,使用三物质分离算法,经后处理去除钙元素,生成彩色编码的VNCA图像,可以显示异常的骨髓水肿,对异常骨髓进行定性及定量分析。Ⅰ期患者通常保守治疗就能恢复,但是ⅡA期患者需要定期复查,防止病情进展进展,必要时可早期干预,鉴于目前ⅡA期患者发病率较高,所以影像诊断ⅡA期对于OLT的临床转归非常重要[4]。
迄今为止尚无DECT应用于OLT的文献报道。本研究旨在探讨DECT对OLT及ⅡA期的诊断价值。
1. 材料与方法
1.1 研究对象
本研究通过医院伦理委员会批准,所有纳入研究的患者均签署知情同意书。纳入标准:①临床上踝关节后足跟对齐情况、稳定性、运动范围及美国足踝骨科协会量表评分[5]符合OLT表现;②MRI图像有典型明确的OLT影像表现,并可以根据Hepple改良的MRI分期标准进行分级;③无踝关节手术史;④无急性外伤或踝关节骨折。
根据上述纳入标准,纳入2023年1月至2023年12月河北省人民医院骨科接诊,经临床及MRI检查确诊为OLT的患者共30例,男14例,女16例,年龄18~70岁,平均年龄为(42±16)岁。所有纳入的患者均进行患侧踝关节MRI检查及双侧踝关节DECT检查,两种检查间隔时间在24 h内。
1.2 DECT扫描参数及图像的重建和后处理
所有患者均使用第3代双源双能CT(somatom Definition Force,Siemens Healthineers)进行扫描。该设备有两套X线球管,A球管:管电压80 kV,管电流150 mA;B球管:管电压Sn 150 kV,管电流100 mA,准直器0.6 mm,螺距0.7,重建层厚3.0 mm。使用自动管电流调制技术(CARE DOSE 4 D)。患者仰卧位,双脚跟并拢,足先进的方式,扫描范围自胫骨下段至跟骨下缘。一次DECT扫描后,得到80 kV,Sn 150 kV和0.5系数融合图,0.5系数融合图与单能120 kV的加权图像相近,可以作为常规CT分析使用。将其发送至工作站(Syngo Via DECT,VB10)进行处理。VNCA技术选择“Bone Marrow”后处理功能,形成VNCA彩色编码的图像。
1.3 MRI扫描参数
采用GE1.5 MRI(Signa Excitehdx;GE Healthcare),使用踝关节专用表面线圈,扫描范围同CT。包括的序列有:矢状位快速自旋回波T1 WI序列(TR580 ms,TE11.8 ms,FOV18×18 mm;矩阵288×224,层厚3.0 mm,层间距1.0 mm),冠状位脂肪抑制T2 WI序列(fat saturation T2 weighted image,FS-T2 WI),(TR
3560 ms,TE 68.5 ms,FOV17×17 mm;矩阵288×192,层厚3.0 mm,层间距1.0 mm),轴位T2 WI(TR3240 ms,TE 63.0 ms,FOV15×15 mm;矩阵320×192,层厚4.0 mm,层间距1.0 mm)。1.4 主观定性及客观定量评估
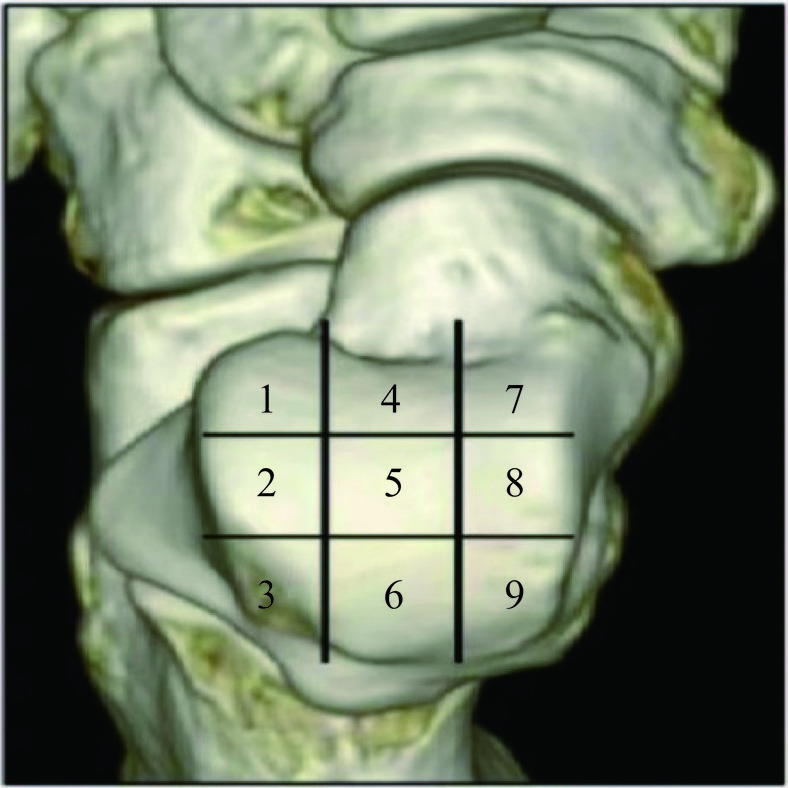
为方便记录病变的区域及范围,将距骨穹隆表面划为九宫格分区[6](图1)。DECT三维重建,利用轴位的分区进行矢状位及冠状位的定位。MRI同样根据轴位,使用定位线对矢状位及冠状位进行病灶定位。采用Hepple等改良的MRI分期标准。为方便研究、比较,我们将阴性的区域,定为0期。
![]() 图 1 距骨骨软骨的九宫格分区(上面观)Figure 1. Nine-grid partitioning of the talar osteochondral surface (superior view)
图 1 距骨骨软骨的九宫格分区(上面观)Figure 1. Nine-grid partitioning of the talar osteochondral surface (superior view)本研究由4名骨科经验丰富的放射科主治医生A、B、C和D,分别对MRI及DECT图像进行分期。A医生对30例MRI图像进行诊断及分期。B医生和C医生,在不知MRI结果的情况下,对0.5系数DECT融合图和VNCA图像进行视觉评估分期。DECT图像评估时,首先观察0.5系数融合图及其三维重建图像,对OLT进行Ⅰ、Ⅱ、Ⅳ、Ⅳ、Ⅴ的大体分期,再观察VNCA图像,把Ⅱ期分为ⅡA期和ⅡB期,有骨髓异常信号为ⅡA期,无骨髓异常信号为ⅡB期。在VNCA图像上,观察关节软骨下的骨髓,正常骨髓颜色为蓝紫色,异常的骨髓区域,表现为边缘模糊的绿色(图2)。
![]() 图 2 患者女62岁,诊断为OLTFigure 2. The patient is a 62 year-old female diagnosed with an osteochondral lesion of the talus
图 2 患者女62岁,诊断为OLTFigure 2. The patient is a 62 year-old female diagnosed with an osteochondral lesion of the talusD医生对照MRI的T2 WI序列,使用VNCA技术对ⅡA期相应病变区域进行定量评估。在VNCA图像上找到相应的异常区域,避开骨皮质下2 mm区域,手动画感兴趣区(region of interest,ROI),面积为0.2 cm2,同一区域进行至少两次测量,取平均CT值。在VNCA图像上找正常骨髓区域(同一患者同侧距骨),避开骨皮质下2 mm区域(减少骨皮质对病变的干扰),手动画ROI,面积为0.2 cm2,进行至少两次测量,取平均CT值。
1.5 统计学分析
利用SPSS 26.0统计软件分析。以MRI结果为标准,分别评估医生B和医生CDECT分级结果与MRI分期结果的一致性,及两名医生之间DECT分期结果的一致性。当0.80<Kappa≤1时,表示两结果具有高度一致性;当0.60<Kappa≤0.80时,两结果一致性好;当0.40<Kappa≤0.60时,两结果具有中等一致性;当0.20<Kappa≤0.40时,表示两结果一致性尚可,当Kappa≤0.20时,两结果一致性差。
以MRI为诊断标准,分别计算B医生和C医生的DECT分期结果的敏感性、特异性、准确性、阳性预测值(positive predictive value,PPV)、阴性预测值(negative predictive value,NPV)和一致性;两名医生DECT结果之间的一致性。B医生和C医生使用虚拟去钙技术视觉评估ⅡA的敏感性、特异性;对比MRI结果,B医生和C医生视觉评估ⅡA的一致性;两名医生之间的一致性。
D医生在VNCA图像上ⅡA期病灶区测得的CT值及对照组CT值,进行正态性检验,若数据符合正态性分布,则对这组数据使用独立样本T检验,若数据不符合正态性分布,则使用Mann-Whitney U检验。使用受试者工作(receiver operating characteristic,ROC)曲线对这组数据进行分析,计算曲线下面积(areas under the curve,AUC),计算ⅡA期病变区与正常区骨髓CT值的最佳截断值,及此时的敏感性、特异性。
2. 结果
2.1 主观图像分析
总共收录30个踝关节,270个区域。
A医生MRI评估结果如下,164个0期区域,5个Ⅰ期区域,89个ⅡA期区域,4个ⅡB期区域,5个Ⅲ期区域,2个Ⅳ期区域,1个Ⅴ期区域。
B医生DECT评估结果如下,158个0期区域,0个Ⅰ期区域,85个ⅡA期区域,16个ⅡB期区域,5个Ⅲ期区域,2个Ⅳ期区域,4个Ⅴ期区域(表1)。
表 1 B医生DECT分区结果与MRI结果计数Table 1. Counts of dual energy computed tomography (DECT) staging results and magnetic resonance imaging (MRI) results performed by Doctor B分区 0 Ⅰ Ⅲ IⅤ Ⅴ ⅡA ⅡB DECT Total 0 151 0 0 0 3 10 0 164 Ⅰ 5 0 0 0 0 0 0 5 Ⅲ 0 0 5 0 0 0 0 5 Ⅳ 0 0 0 2 0 0 0 2 Ⅴ 0 0 0 0 1 0 0 1 ⅡA 2 0 0 0 0 75 12 89 ⅡB 0 0 0 0 0 0 4 4 MRI Total 158 0 5 2 4 85 16 270 C医生DECT评估结果如下,158个0期区域,0个Ⅰ期区域,86个ⅡA期区域,15个ⅡB期区域,5个Ⅲ期区域,2个Ⅳ期区域,4个Ⅴ期区域(表2)。
表 2 C医生DECT分区结果与MRI结果计数Table 2. Counts of dual energy computed tomography (DECT) staging results and magnetic resonance imaging (MRI) results performed by Doctor C分区 0 Ⅰ Ⅲ Ⅳ Ⅴ ⅡA ⅡB DECT Total 0 150 0 0 0 3 11 0 164 Ⅰ 5 0 0 0 0 0 0 5 Ⅲ 0 0 5 0 0 0 0 5 Ⅳ 0 0 0 2 0 0 0 2 Ⅴ 0 0 0 0 1 0 0 1 ⅡA 3 0 0 0 0 75 11 89 ⅡB 0 0 0 0 0 0 4 4 MRI Total 158 0 5 2 4 86 15 270 以MRI为参考标准,B医生和C医生运用DECT评估OLT结果的敏感性、特异性、准确性、阳性预测值、阴性预测值分别为84%,91%、89%、83%、90%和85%、89%、88%、83%、91%。B医生和C医生的DECT结果与MRI结果Kappa值分别为0.771和0.758;B医生和C医生的DECT结果Kappa值为0.886。
对比MRI,B医生和C医生使用虚拟去钙技术视觉评估ⅡA的敏感性、特异性分别为85%、94%和84%、93%,对比MRI,B医生和C医生视觉评估ⅡA的Kappa值分别为0.807和0.801,B医生和C医生之间的Kappa值为0.889。
在ⅡA期评估中,B医生和C医生的假阳性区域分别有10个和11个区域,其中区域并不完全相同。B医生假阴性区域有14个,其中12个区域因未发现骨髓异常,被诊断为ⅡB期,另2个区域,因未发现隐匿性骨折和骨髓异常,被诊断为0期;C医生假阴性14个,其中11个区域因未发现骨髓异常,被诊断为ⅡB期,另3个区域,因未发现隐匿性骨折和骨髓异常,被诊断为0期。
2.2 客观图像分析
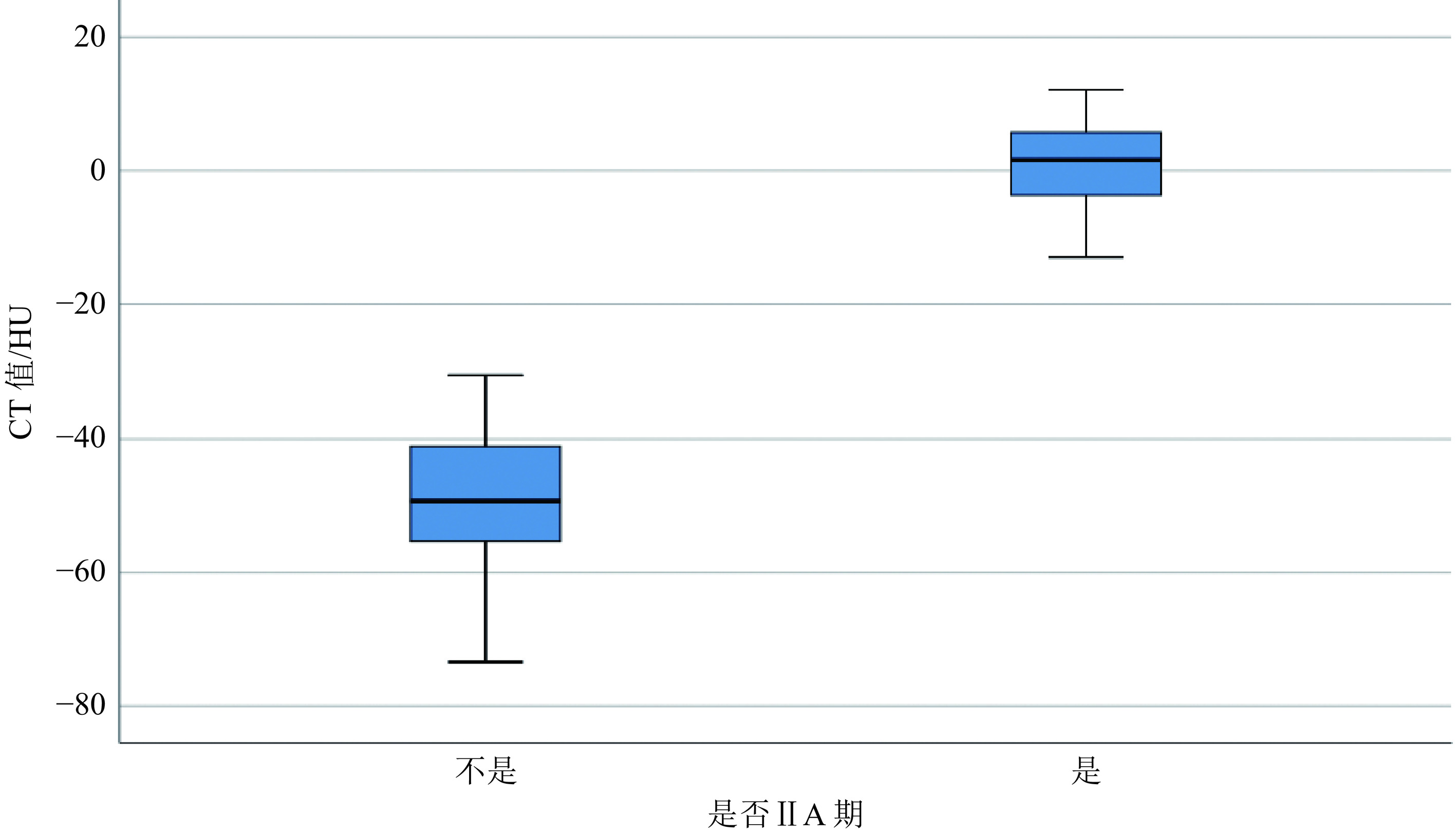
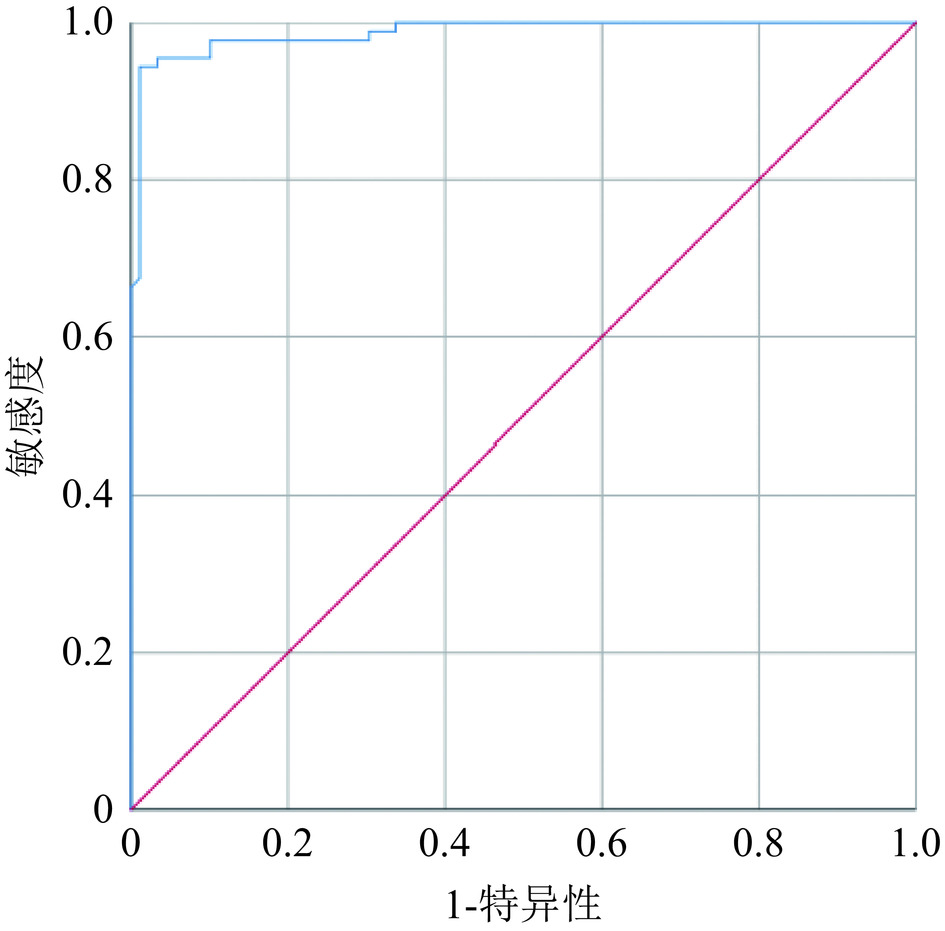
以MRI为参考标准,总共有89个ⅡA期区域,D医生在VNCA图像上找出与T2 WI序列上相对应的骨髓水肿区域,测量得出89个异常CT值,对照组(在同一患者的同侧距骨上)测出89个正常骨髓区CT值。总共测出的178个CT值,经SPSS统计软件计算,病变区骨髓CT值(0.55±1.22)HU,对照组骨髓CT值(−48.30±1.24)HU(表3),病变区骨髓CT值与对照组CT值存在统计学差异(P<0.01)(图3)。病变区的CT值ROC曲线显示(图4),AUC值为0.987(95%置信区间:0.974−1.000),病变区骨髓CT值与对照组CT值的最佳截断值为−21.85 HU,此时的敏感性、特异性分别为92%和98.9%。
表 3 在VNCA图像上,D医生测得的IIA期病变区CT值和对照组CT值Table 3. Normal bone marrow computed tomography (CT) attenuation and Stage IIA lesion CT attenuation values measured on the virtual non-calcium images (VNCA) by Doctor DNormal bone marrow (none Edema) Stage IIA (with bone marrow edema) P CT value (0.55±1.22)HU (−48.30±1.24)HU <0.01 ![]() 图 3 D医生在VNCA图像上测得IIA期病灶区CT值与对照组CT值Figure 3. The computed tomography (CT) attenuation values of Stage IIA lesion area and the normal bone marrow CT attenuation values on virtual non-calcium (VNCA) images performed by Doctor D
图 3 D医生在VNCA图像上测得IIA期病灶区CT值与对照组CT值Figure 3. The computed tomography (CT) attenuation values of Stage IIA lesion area and the normal bone marrow CT attenuation values on virtual non-calcium (VNCA) images performed by Doctor D![]() 图 4 D医生测量统计定量诊断IIA 的ROC曲线Figure 4. Region under the curve (ROC) plot of the diagnostic value of dual energy computed tomography virtual non-calcium images for Stage IIA osteochondral lesion of the talus measured by Doctor D
图 4 D医生测量统计定量诊断IIA 的ROC曲线Figure 4. Region under the curve (ROC) plot of the diagnostic value of dual energy computed tomography virtual non-calcium images for Stage IIA osteochondral lesion of the talus measured by Doctor D3. 讨论
3.1 OLT的病因及发病机制
OLT主要影响距骨穹隆的软骨及软骨下骨,其病因多样,因人群而异[7]。儿童和年轻人中,病因包括局部缺血、次级关节下骺板异常软骨内骨化、重复性微创伤及遗传倾向,常表现为剥脱性骨软骨炎,特征是软骨退变与软骨下骨骨质分离,被视为非创伤性特发性现象。成年人中,OLT可归因于外伤、内分泌或代谢异常、维生素D缺乏及退行性关节疾病[8],其中外伤最为常见。外伤性距骨骨软骨损伤具有特定规律[9]:前外侧区域损伤通常由踝关节内翻和背伸暴力引起,形成浅而圆片状的损伤;后内侧区域损伤则因反复内翻、跖屈和外旋暴力所致,形成深而杯形的损伤。
OLT的病理改变涉及距骨穹窿的软骨下骨[10]。外伤等因素可导致微骨折和骨挫伤,愈合不良后,液体间歇性地渗入软骨下骨,产生压力,引发骨坏死和骨吸收,形成溶解性病变和骨软骨碎片。液体压力减少时,骨吸收停止,周围发生骨重塑和过度成骨反应,导致修复困难[11]。软骨下骨板的损伤对软骨代谢至关重要,其退化会导致蛋白聚糖和糖蛋白流失,加剧软骨受损[13]。因此,早期检测软骨下骨板损伤对OLT的干预至关重要[14]。由于MRI的T2 WI序列能显示因液体压力导致的骨吸收、骨溶解和骨囊变的高信号[12],因此MRI为本病的主要影像检查手段。目前有关本病的MRI报道较多,而DECT用于OLT诊断迄今尚未见文献报道。
3.2 DECT在骨髓水肿诊断中的应用价值
常规CT使用多能谱射线,会产生射线硬化现象[15],导致物质真实的衰减系数与CT多能谱射线的衰减只是近似相等。相比之下,双能量CT(DECT)采用单一能谱的单色射线[16],其光子能量相同。DECT的虚拟非钙成分分析(VNCA)技术通过三物质分离技术[17],能分解每个体素的衰减为钙含量和虚拟去钙含量,生成钙图和VNCA图。VNCA图以彩色编码直接显示骨髓颜色变化,蓝紫色代表正常黄骨髓,绿色表示骨髓水肿或炎症[18]。在评估非创伤性骨髓水肿时,DECT使用50 HU截止值进行颜色编码图像可视化[19],有助于区分轻度和重度骨髓水肿[20],并通过调整叠加级别和阈值获得更清晰显示[21]。
文献[22]指出DECT在脊柱及四肢创伤性、非创伤性骨髓水肿及关节炎性病变诊断方面呈现出较高的应用价值。Foti等[23]等的综述显示,DECT对急性压缩骨折患者的急性骨髓水肿检查具有高度的敏感性(86.2%)、特异性(91.2%)和准确性(89.3%)。Wang等[24]研究认为DECT在膝关节和踝关节的骨软骨损伤诊断中表现非凡。对于创伤性及非创伤性损伤,尤其是骨关节炎伴疼痛时出现的典型骨髓水肿,DECT通过虚拟非钙成分分析(VNCA)技术能够清晰观察到软骨下不均匀、边界模糊的骨髓水肿[25]。尽管软骨下骨硬化可能导致一定的误诊或漏诊[26],但结合关节间隙变窄、关节炎、韧带及半月板损伤等影像学特征,有效的提高了DECT的诊断准确性。Jans等[27]的研究表明,VNCA技术在诊断外伤引起的距骨创伤性骨髓水肿方面,无论是定性(敏感性97.4%、特异性 86.9%、PPV88.2%、NPV97.1%、准确性95.5%)还是定量(敏感性98.00%、特异性90.31%、PPV91.00%、NPV92.31%和准确性96.83%)分析,均呈现出高度的敏感性、特异性和准确性。此外,也有文献报道,DECT在检测软骨下骨折及骨皮质受累方面较MRI更为准确[28],因其能较好的显示关节软骨下骨的小囊变、早期骨质硬化、坍塌骨质周围的骨髓水肿,从而有助于关节骨软骨损伤的分期评估[29]。
本研究结果显示,在OLT的ⅡB期、Ⅲ期、Ⅳ期、Ⅴ期的诊断中,DECT的诊断效能与MRI基本相仿。值得关注的是,在CT诊断的Ⅴ期病例中有3例MRI漏诊。笔者体会这可能与距骨关节面下囊性灶较小(直径均小于1.5 mm),常规CT对骨质的细小病灶显示及测量较扫描层厚较厚的MRI图像更具优势有关,此点与文献[30-31]报道相符。尽管本研究上述四期病例的样本量相对较少,但仍能说明DECT对OLT的诊断价值不容小觑。
本研究结果还显示,对于OLT的ⅡA期,两名医生主观评估的敏感性、特异性分别为85%、94%和84%、93%,两名医生DECT评估结果对比MRI的Kappa值分别为0.807和0.801,两名医生之间的Kappa值为0.889,与Ren等[32]研究结果基本相符,而在诊断敏感性方面与longo[33]、何绪成等[34]研究结果相比较略低。我们认为,这与本研究纳入的OLT患者骨髓损伤程度较轻,病变范围相对较小,以及OLT的异常骨髓密度位于软骨下区域,易受到关节腔和关节面下骨质硬化的干扰[35],导致VNCA图像编码颜色发生变化,从而影响了DECT的检测效果有关。
关于本研究ⅡA期诊断出现的假阳性(B医生约11.8%、C医生约12.8%)及假阴性(B医生约15.7%、C医生约15.7%)现象,同样值得关注。笔者分析前者可能与以下因素有关:①年轻患者的距骨可能含有较多不均匀分布的红骨髓,导致VNCA图像呈现相对高密度;②距骨穹隆的骨质硬化也可能使VNCA图像呈现高密度,进而引发假阳性。因此,在评估过程中,先查看DECT的0.5系数融合图以了解骨硬化部位,有助于减少误诊风险。后者形成的原因可能为:①异常骨髓病变范围较小,程度较轻,VNCA上未能显示。②轻度病变与正常骨髓颜色差距小,不同阅读者在识别时可能会有差异,在DECT 0.5系数融合图上,未发现阴性骨折。③患者年龄偏大,距骨骨皮质及其下方骨质有不同程度的骨质疏松、密度较低,导致特别轻微的骨小梁断裂未被发现而漏诊[36]。
本研究结果尚显示,OLTⅡA期骨髓异常区与正常骨髓区CT值具有显著统计学差异,前者CT值明显高于后者,最佳截断值为−21.85 HU,其敏感性、特异性分别为92%和98.9%,与Foti等[37]研究结果(截断值为−20 HU,敏感性88%,特异性86.6%)相仿。表明CT定量检测对OLTⅡA期骨髓水肿的诊断具有重要的佐证意义。然而,由于设备、扫描参数、检测位点、受检者年龄等因素影响[38],有研究[37-38]显示最佳截断CT值存在较大差异,需要在实际工作中予以甄别。
3.3 本研究的局限性
本研究具有以下局限性:①所收集的病例以轻症患者为主,除ⅡA期外,其他四期的病例样本数偏少,未来需要收集更多其他各期病例,以更好的印证DECT对其他各期的诊断价值;②DECT对Ⅰ期仅软骨损伤的病例观察受限。由于VNCA技术不能很好的显示关节软骨,本研究5例Ⅰ期患者均出现假阴性结果。笔者赞同其原因可能与踝关节间隙较窄,关节软骨较薄有关[39]。期待通过优化检查方法,通过轴向牵引踝关节并行CT检查,以增宽关节间隙,再经特定软件处理及颜色编码,更好的显示关节软骨[40],从而使OLTⅠ期患者得到及时诊断与治疗。③本研究侧重于OLT的DECT分期及ⅡA期的诊断,以MRI作为评估骨髓水肿的金标准并与其进行对照分析,但MRI在OLT尤其是在Ⅰ期诊断的准确性并非100%,未来需要记录关节镜及手术结果加以对照。④本研究中使用的VNCA算法只与相同的供应商的特定后处理软件兼容,是否与其他制造商的DECT系统兼容尚未可知。
综上研究表明,相较于MRI检查,DECT在OLT的诊断及分期上具备可行性。借助VNCA技术,能够识别OLT区域中的骨髓水肿,并对ⅡA期进行准确、量化的诊断评估,呈现出良好的诊断效能。然而,DECT在Ⅰ期的诊断上表现欠佳。本研究仅为初步探索,未来还需深入研究。期待DECT在OLT诊断领域为临床提供更多有价值的信息。
-
![]()
图 1 距骨骨软骨的九宫格分区(上面观)
Figure 1. Nine-grid partitioning of the talar osteochondral surface (superior view)
![]()
图 2 患者女62岁,诊断为OLT
Figure 2. The patient is a 62 year-old female diagnosed with an osteochondral lesion of the talus
![]()
图 3 D医生在VNCA图像上测得IIA期病灶区CT值与对照组CT值
Figure 3. The computed tomography (CT) attenuation values of Stage IIA lesion area and the normal bone marrow CT attenuation values on virtual non-calcium (VNCA) images performed by Doctor D
![]()
图 4 D医生测量统计定量诊断IIA 的ROC曲线
Figure 4. Region under the curve (ROC) plot of the diagnostic value of dual energy computed tomography virtual non-calcium images for Stage IIA osteochondral lesion of the talus measured by Doctor D
表 1 B医生DECT分区结果与MRI结果计数
Table 1 Counts of dual energy computed tomography (DECT) staging results and magnetic resonance imaging (MRI) results performed by Doctor B
分区 0 Ⅰ Ⅲ IⅤ Ⅴ ⅡA ⅡB DECT Total 0 151 0 0 0 3 10 0 164 Ⅰ 5 0 0 0 0 0 0 5 Ⅲ 0 0 5 0 0 0 0 5 Ⅳ 0 0 0 2 0 0 0 2 Ⅴ 0 0 0 0 1 0 0 1 ⅡA 2 0 0 0 0 75 12 89 ⅡB 0 0 0 0 0 0 4 4 MRI Total 158 0 5 2 4 85 16 270  下载: 导出CSV
下载: 导出CSV
表 2 C医生DECT分区结果与MRI结果计数
Table 2 Counts of dual energy computed tomography (DECT) staging results and magnetic resonance imaging (MRI) results performed by Doctor C
分区 0 Ⅰ Ⅲ Ⅳ Ⅴ ⅡA ⅡB DECT Total 0 150 0 0 0 3 11 0 164 Ⅰ 5 0 0 0 0 0 0 5 Ⅲ 0 0 5 0 0 0 0 5 Ⅳ 0 0 0 2 0 0 0 2 Ⅴ 0 0 0 0 1 0 0 1 ⅡA 3 0 0 0 0 75 11 89 ⅡB 0 0 0 0 0 0 4 4 MRI Total 158 0 5 2 4 86 15 270
下载: 导出CSV
表 3 在VNCA图像上,D医生测得的IIA期病变区CT值和对照组CT值
Table 3 Normal bone marrow computed tomography (CT) attenuation and Stage IIA lesion CT attenuation values measured on the virtual non-calcium images (VNCA) by Doctor D
Normal bone marrow (none Edema) Stage IIA (with bone marrow edema) P CT value (0.55±1.22)HU (−48.30±1.24)HU <0.01
下载: 导出CSV
-
[1] MASQUIJO J J, ALLENDE F, CARABAJAL M. Ankle morphology and juvenile osteochondritis dissecans (JOCD) of the talus: is there an association an MRI study[J]. Journal of Pediatric Orthopedics, 2021, 41(2): e147-e152. DOI: 10.1097/BPO.0000000000001715.
[2] PATEL M, FRANCAVILLA M L, LAWRENCE J, et al. Osteochondral lesion of the talus in children: Are there MRI findings of instability[J]. Skeletal Radiology, 2020, 49(8): 1305-1311. DOI: 10.1007/s00256-020-03436-6.
[3] FOTI G, FACCIOLI N, SILVA R, et al. Bone marrow edema around the hip in non-traumatic pain: dual-energy CT vs MRI[J]. European Radiology, 2020, 30(7): 4098-4106. DOI: 10.1007/s00330-020-06775-z.
[4] DRAKOS M C, EBLE S K, CABE T N, et al. Comparison of functional and radiographic outcomes of talar osteochondral lesions repaired with micronized allogenic cartilage extracellular matrix and bone marrow aspirate concentrate vs microfracture[J]. Foot and Ankle International, 2021, 42(7): 841-850. DOI: 10.1177/1071100720983266.
[5] BRUNS J, HABERMANN C, WERNER M. Osteochondral lesions of the talus: A review on talus osteochondral injuries, including osteochondritis dissecans[J]. Cartilage, 2021, 13(S1): 1380S-1401S.
[6] WEI Y, SONG J, YUN X, et al. Outcomes of single-stage versus staged treatment of osteochondral lesions in patients with chronic lateral ankle instability: A prospective randomized study[J]. Orthopaedic Journal of Sports Medicine, 2022, 10(2): 941674965.
[7] LOPES R, GEFFROY L, PADIOLLEAU G, et al. Proposal of a new CT arthrographic classification system of osteochondral lesions of the talus[J]. Orthopaedics & Traumatology, Surgery & Research, 2021: 107(6): 102890.
[8] NAKASA T, IKUTA Y, SUMII J, et al. Arthroscopic fixation using bioabsorbable pins with bone grafting via a medial malleolus approach to treat osteochondral lesion of the talus[J]. Foot and Ankle Specialist, 2022: 178737358.
[9] BAI L, ZHANG Y, CHEN S, et al. Analysis of factors affecting the prognosis of osteochondral lesions of the talus[J]. International Orthopaedics, 2023, 47(3): 861-871. DOI: 10.1007/s00264-022-05673-x.
[10] CAO Y, XU Y, HUANG Q, et al. Characteristics of osteochondral lesions of the talus in different age groups[J]. International Journal of Sports Medicine, 2020, 41(12): 873-878. DOI: 10.1055/a-1186-1575.
[11] HURLEY E T, STEWART S K, KENNEDY J G, et al. Current management strategies for osteochondral lesions of the talus[J]. Bone and Joint Journal, 2021, 103-B(2): 207-212.
[12] WANG C C, YANG K C, CHEN I H. Current treatment concepts for osteochondral lesions of the talus[J]. Tzu Chi Medical Journal, 2021, 33(3): 243-249. DOI: 10.4103/tcmj.tcmj_106_20.
[13] KANERIA N, REDMAN S, LITTLE D, et al. Diagnostic value of single-photon emission computed tomography-CT foot and ankle studies[J]. Nuclear Medicine Communications, 2022, 43(4): 392-397. DOI: 10.1097/MNM.0000000000001525.
[14] GIANAKOS A L, HARING R S, SHIMOZONO Y, et al. Effect of microfracture on functional outcomes and subchondral sclerosis following distraction arthroplasty of the ankle joint[J]. Foot and Ankle International, 2020, 41(6): 631-638. DOI: 10.1177/1071100720917144.
[15] FOTI G, LONGO C, D'ONOFRIO M, et al. Dual-energy CT for detecting painful knee prosthesis loosening[J]. Radiology, 2023, 306(3): e211818. DOI: 10.1148/radiol.211818.
[16] ABAS S, KUIPER J H, ROBERTS S, et al. Osteochondral lesions of the ankle treated with bone marrow concentrate with hyaluronan and fibrin: A single-centre study[J]. Cells, 2022, 11(4).
[17] JANTZEN C, EBSKOV L B, JOHANSEN J K. AMIC procedure for treatment of osteochondral lesions of talus-a systematic review of the current literature[J]. Journal of Foot and Ankle Surgery, 2022, 61(4): 888-895. DOI: 10.1053/j.jfas.2021.12.017.
[18] PEREIRA G F, STEELE J R, FLETCHER A N, et al. Fresh osteochondral allograft transplantation for osteochondral lesions of the talus: A systematic review[J]. Journal of Foot and Ankle Surgery, 2021, 60(3): 585-591. DOI: 10.1053/j.jfas.2021.02.001.
[19] GIANAKOS A L, WILLIAMSON E, MERCER N, et al. Gender differences may exist in the presentation, mechanism of injury and outcomes following bone marrow stimulation for osteochondral lesions of the talus[J]. The Journal of Foot and Ankle Surgery, 2023, 62(1): 75-79. DOI: 10.1053/j.jfas.2022.04.010.
[20] WALTHER M, GOTTSCHALK O, MADRY H, et al. Etiology, classification, diagnostics, and conservative management of osteochondral lesions of the talus. 2023 recommendations of the working group "Clinical Tissue Regeneration" of the German Society of Orthopedics and Traumatology[J]. Cartilage, 2023, 14(3): 292-304. DOI: 10.1177/19476035231161806.
[21] DENG E, GAO L, SHI W, et al. Both magnetic resonance imaging and computed tomography are reliable and valid in evaluating cystic osteochondral lesions of the talus[J]. Orthopaedic Journal of Sports Medicine, 2020, 8(9): 1811994121.
[22] FOTI G, MANTOVANI W, FACCIOLI N, et al. Identification of bone marrow edema of the knee: diagnostic accuracy of dual-energy CT in comparison with MRI[J]. Radiol Medicine, 2021, 126(3): 405-413. DOI: 10.1007/s11547-020-01267-y.
[23] FOTI G, SERRA G, IACONO V, et al. Identification of traumatic bone marrow oedema: The pearls and pitfalls of dual-energy CT (DECT)[J]. Tomography, 2021, 7(3): 424-433. DOI: 10.3390/tomography7030037.
[24] WANG M Y, ZHANG X Y, XU L, et al. Detection of bone marrow oedema in knee joints using a dual-energy CT virtual non-calcium technique[J]. Clinical Radiology, 2019, 74(10): 811-815.
[25] WANG Y, CHEN Y, ZHENG H, et al. Detection of different degree traumatic vertebral bone marrow oedema by virtual non-calcium technique of dual-source dual-energy CT[J]. Clinical Radiology, 2020, 75(2): 111-156.
[26] NARAYANAN A, DETTORI N, CHALIAN M, et al. Dual-energy CT-generated bone marrow oedema maps improve timely visualisation and recognition of acute lower extremity fractures[J]. Clinical Radiology, 2021, 76(9): 710-719.
[27] JANS L, DE KOCK I, HERREGODS N, et al. Response to: 'Use of dual-energy CT to detect and depict bone marrow oedema in rheumatoid arthritis: is it ready to substitute MRI?' by Wu et al[J]. Annals of The Rheumatic Diseases, 2019, 78(9): e90. DOI: 10.1136/annrheumdis-2018-213960.
[28] WU H, ZHANG G, HUANG X, et al. Use of dual-energy CT to detect and depict bone marrow oedema in rheumatoid arthritis: Is it ready to substitute MRI[J]. Annals of the Rheumatic Diseases, 2019, 78(9): e89. DOI: 10.1136/annrheumdis-2018-213892.
[29] FOTI G, GOBBI F, ANGHEBEN A, et al. Radiographic and HRCT imaging findings of chronic pulmonary schistosomiasis: Review of 10 consecutive cases[J]. British Journal of Radiology Case Reports, 2019, 5(3): 20180088.
[30] FOTI G, LOMBARDO F, FIGHERA A, et al. Role of diffusion tensor imaging of sciatic nerve in symptomatic patients with inconclusive lumbar MRI[J]. European Journal of Radiology, 2020, 131: 109249. DOI: 10.1016/j.ejrad.2020.109249.
[31] LUO S, CAO Y, HU P, et al. Quantitative evaluation of ankle cartilage in asymptomatic adolescent football players after season by T2-mapping magnetic resonance imaging[J]. Biomedical Engineering Online, 2021, 20(1): 130. DOI: 10.1186/s12938-021-00970-9.
[32] REN Q, TANG D, XIONG Z, et al. Traumatic bone marrow lesions in dual-energy computed tomography[J]. Insights into Imaging, 2022, 13(1): 174. DOI: 10.1186/s13244-022-01312-6.
[33] FOTI G, LONGO C, D'ONOFRIO M, et al. Dual-energy CT for detecting painful knee prosthesis loosening[J]. Radiology, 2023, 306(3): e211818. DOI: 10.1148/radiol.211818.
[34] 何绪成, 周闪闪, 叶菊, 等. 双能CT虚拟去钙在距骨骨髓水肿中的应用价值[J]. 中国CT和MRI杂志, 2022, 20(2): 161-165. DOI: 10.3969/j.issn.1672-5131.2022.02.052. HE X C, ZHOU S S, YE J, et al. Application of dual energy CT virtual noncalcium technique in bone marrow edema of talus[J]. Chinese Journal of CT and MRI, 2022, 20(2): 161-165. DOI: 10.3969/j.issn.1672-5131.2022.02.052. (in Chinese).
[35] NAKASA T, IKUTA Y, SUMII J, et al. Characteristics of chronic ankle instability requiring both anterior talofibular and calcaneofibular ligament repair[J]. The Journal of Foot and Ankle Surgery, 2022, 61(5): 1028-1033. DOI: 10.1053/j.jfas.2022.01.009.
[36] 曹家晟, 李保磊. 光子计数X射线CT能量成像精度影响因素分析[J]. CT理论与应用研究, 2024, 34(2): 1-8. DOI: 10.15953/j.ctta.2024.254. CAO J S, LI B L. Analysis of Accuracy Related factors in photon counting X-ray CT energy imaging[J]. CT Theory and Applications, 2024, 34(2): 1-8. DOI: 10.15953/j.ctta.2024.254. (in Chinese).
[37] FOTI G, LOMBARDO F, GUERRIERO M, et al. Management of vertebral compression fractures: the role of dual-energy CT in clinical practice[J]. Radiologia Medica, 2022, 127(6): 627-636. DOI: 10.1007/s11547-022-01498-1.
[38] FOTI G, FIGHERA A, CAMPACCI A, et al. Diagnostic performance of dual-energy CT for detecting painful hip prosthesis loosening[J]. Radiology, 2021, 300(3): 641-649. DOI: 10.1148/radiol.2021203510.
[39] FENG P, LI G, LIANG P. The value of dual-energy computed tomography (DECT) in the diagnosis of urinary calculi: a systematic review and meta-analysis of retrospective studies[J]. PeerJ, 2023, 11: e16076. DOI: 10.7717/peerj.16076.
[40] FACCIOLI N, SANTI E, FOTI G, et al. Cost-effectiveness analysis of including contrast-enhanced ultrasound in management of pancreatic cystic neoplasms[J]. Radiologia Medica, 2022, 127(4): 349-359. DOI: 10.1007/s11547-022-01459-8.
-
期刊类型引用(3)
1. 雷兰芳. 磁共振胰胆管成像联合腹部CT诊断肝外胆管结石的应用价值研究. 影像研究与医学应用. 2025(04): 171-173 .  百度学术
百度学术
2. 夏华伟,朱文雅,胡红杰,文玲. 10例误诊IgG4相关性胰腺炎的影像学表现. 中国医学影像技术. 2025(04): 622-626 . 百度学术
3. 张斌斌,戴娜,杨迎,霍健伟,靳二虎. 自身免疫性胰腺炎患者少见的影像表现. 磁共振成像. 2024(06): 123-128 . 百度学术
其他类型引用(0)

计量
- 文章访问数: 26
- HTML全文浏览量: 4
- PDF下载量: 4
- 被引次数: 3


