
Low-Dose Study on Coronary Artery Calcium Score Scanning Using the SEMI Mode of the Intelligent Optimal Tube Voltage Selection Technique in Combination with an Iterative Algorithm
-
摘要:
目的:探讨智能最佳管电压技术[1]SEMI模式(Care kV SEMI)联合迭代算法在冠状动脉检查中钙化积分低剂量扫描成像中的可行性。方法:模体实验采用Care kV SEMI模式和管电流调制技术(CareDose 4D on)。参数设置:SEMI 120 kV(ref.kV分别为100 kV、120 kV),ref.mAs分别为40 mAs、60 mAS、80 mAs,重建算法分别为滤波反投影算法(FBP)、基于模型的高级迭代算法(ADMIRE)3、4、5。比较各组图像的容积CT剂量指数(CTDIvol)、对比噪声比(CNR模)和品质因子(FOM)。回顾性分析30例冠状动脉钙化积分扫描图像作为对照组(ref.kV 120 kV,ref.mAs 80 mAs,重建算法FBP),前瞻性采集109例患者冠脉钙化积分CT图像作为实验组(ref.kV 100 kV,ref.mAs 80 mAs,重建算法分别为FBP、ADMIRE3、5),两组实际管电压均为SEMI 120 kV。记录并计算剂量长度乘积(DLP)、有效剂量(ED)、左主干(LM)和右冠状动脉(RCA)开口层面的CNR患、钙化积分(Agatston Score)以及风险分级。由两名高年资诊断医生对患者冠脉图像进行4分法主观评价。对临床研究两组患者冠状动脉CT钙化积分扫描的辐射剂量、钙化积分数值、风险分级以及图像质量差异进行统计学分析。结果:①模体研究结果:实验组辐射剂量较对照组均降低。相同扫描条件CNR模随迭代算法等级增加而增加。ref.kV 100 kV+ref.mAs 80 mAs组四种重建算法下FOM均高于对照组。②临床研究结果:实验组与对照组ED存在统计学差异。实验组FBP和对照组CNR患在LM和RCA两个层面上均无统计学差异。实验组不同重建算法所得Agatston积分间无统计学差异。实验组风险等级Kappa值分别为0.93、0.88,一致性好。两名医生主观评价Kappa值为0.952,实验组与对照组主观评分有统计学差异。结论:BMI18-25患者进行冠状动脉钙化积分CT扫描时,使用CARE kV SEMI模式联合迭代算法对钙化积分和风险分级影响较小,可以有效降低患者辐射剂量。
-
关键词:
- CARE kV SEMI模式 /
- 迭代算法 /
- 钙化积分 /
- 体层摄影术 /
- 低剂量
Abstract:Objective: To explore the feasibility of the SEMI mode of the intelligent optimal tube voltage selection technique (Care kV SEMI) in combination with an iterative algorithm in low-dose calcium score scanning for coronary artery examination. Methods: SEMI-automatic tube voltage (Care kV SEMI) and tube current (CareDose 4D on) modulation were used in the phantom experiment. For the SEMI automatic tube voltage group SEMI 120 kV (ref.kV was 100 and 120 kV), ref.mAs was 40, 60, and 80 mAs. The reconstruction algorithms were filtered back projection ADMIRE 3, 4, 5. The volume CT dose index (CTDIvol), contrast-to-noise ratio (CNRp) and figure of merit (FOM) of each group were compared, and a set of parameters were selected for clinical patient image acquisition after a comprehensive comparison. A retrospective analysis of coronary artery calcium score scanning images was conducted, using 30 patients as a control group (ref.kV, 120 kV; ref.mAs, 80 mAs; reconstruction algorithm, FBP) and a prospective collection of 109 patients with coronary artery calcium score CT images as an experimental group (Care kV SEMI, 120 kV; ref.kV, 100 kV; ref.mAs, 80 mAs). The reconstruction algorithms were FBP and ADMIRE 3, 5. The dose length product (DLP), effective dose (ED), contrast-to-noise ratio (CNR) at the left main coronary artery (LM) and right coronary artery (RCA) ostial level, Agaston score, and risk classification were recorded and compared between groups. The images of the patients were evaluated by two senior diagnostic doctors on a four-point scale. The radiation dose, calcification score, risk classification, and image quality were statistically analyzed using SPSS software. Results: ① Phantom experiment: The radiation dose of the experimental group was lower than that of the control group. Under the same scanning parameters, the CNRp increased with an increasing reconstruction algorithm level. The FOM of the four reconstruction algorithms in the ref.kV 100 kV + ref.mAs 80 mAs group was higher than that in the control group. ② Clinical study: There was a statistically significant difference in ED between the experimental group and the control group (P < 0.001). There was no statistically significant difference in CNRc between the experimental group with FBP and the control group on the LM and RCA levels (P >
0.0125 ).There was no significant difference in Agaston score between the experimental and control groups (P > 0.05). The consistency of the risk grade in the experimental group was good, with kappa values of 0.93 and 0.88, respectively. There was no statistically significant difference in FBP and CNRc between the experimental and control groups at either level (P >0.0125 ). The subjective evaluation results of doctors A and B were consistent, and the kappa value was 0.952. There was a statistically significant difference in the subjective evaluation between the two groups (P < 0.001). Conclusion: Care kV SEMI combined with an iterative algorithm has little effect on the calcification score and risk classification, and it can effectively reduce the radiation doses of patients with a BMI of 18–25.-
Keywords:
- Care kV SEMI /
- iterative algorithm /
- calcium score /
- computed tomography /
- low-dose
-
冠状动脉粥样硬化性心脏病是临床常见疾病之一,自上世纪八十年代以来,我国冠心病患病率持续上升,成为危害我国人民生命健康的主要因素[2]。基于CT图像计算的冠状动脉钙化积分(Coronary Artery Calcium Score,CACS)是量化分析冠状动脉钙化程度的方法之一,准确地测量钙化积分有助于显示患者的冠状动脉的情况,可以帮助了解患者在未来发生心血管疾病的概率。由于CT检查的辐射剂量远高于X线检查,这使得CT成为医源性放射的主要来源[3]。因此在确保检查准确性的同时降低患者辐射剂量显得尤为重要。本研究旨探讨自动调制技术联合迭代算法在冠状动脉检查中钙化积分低剂量扫描成像中的可行性。
1. 实验材料
Simens双源Force CT机(德国Simens公司);PBU-2型成人胸部拟人模体(日本岛津公司);荷兰Philips Extended Brilliance后处理工作站,Siemens Syngo.via工作站。
2. 模体实验
2.1 体位设计
胸部模体置于检查床正中,激光线对准胸骨正中,水平线位于腋中线。
2.2 参数设置
2.2.1 定位像参数设置
正位定位像,管电压120 kV,管电流20 mA。
2.2.2 钙化积分参数设置
应用智能最佳管电压技术SEMI模式(Care kV SEMI)120 kV及自动管电流调制技术(CareDose 4D on)对胸部模体行6组不同参数的钙化积分扫描,各组ref.kV与ref.mAs分别为:A组120 kV+40 mAs;B组120 kV+60 mAs;C组120 kV+80 mAs;D组100 kV+40 mAs;E组100 kV+60 mAs;F组100 kV+80 mAs。对6组数据行FBP、ADMIRE 3、ADMIRE 4、ADMIRE 5四种算法的重组,其中C组作为对照组。采用回顾性门控采集模式,开启Heart Monitor Demo Mode,模拟心率为60次/分,曝光窗30%~80%,重建设备推荐最佳时相。旋转时间0.25 s,探测器宽度192×0.6 mm,螺距0.2,扫描长度150 mm。层厚3 mm,滤过核:QR36,窗宽/窗位345/50 HU。
2.3 辐射剂量评估
记录6组扫描条件的容积CT剂量指数(CTDIvol)。
2.4 图像质量客观评价
选取每组图像的第26层作为参考层面(模拟左主干口层面)。分别在纵膈区域(信号区)和空气区(背景区)勾画约100 mm2的圆形感兴趣区(图1),测量CT信、CT背、SD背。根据公式(1)计算对比噪声比(CNR模)。
$$ {\mathrm{C}\mathrm{N}\mathrm{R}}_{\mathrm{模}}=({\mathrm{C}\mathrm{T}}_{\mathrm{信}}-{\mathrm{C}\mathrm{T}}_{\mathrm{背}})/{\mathrm{S}\mathrm{D}}_{\mathrm{背}} 。 $$ (1) 2.5 品质因数
根据公式(2)计算品质因数(FOM),用于衡量图像质量与辐射剂量利益最优化的情况。
$$ \mathrm{FOM=CNR}_{ \mathrm{模}}^{ \mathrm{2}} \mathrm{/CTDI}_{ \mathrm{vol}} \mathrm{。} $$ (2) 3. 临床研究
3.1 一般资料
入组标准:BMI18~25,钙化积分不等于0,心率50~95[4]。
排除标准:接受过心脏支架或搭桥手术患者。
回顾性选取41例2021年8月至2021年9月在我院行冠状动脉钙化积分CT扫描的患者作为对照组,年龄(61.3±11.4)岁,男性77%,女性23%,心率(73.5±14.0)BPM;前瞻性选取109例2022年2月至2022年11月在我院使用优化后的钙化积分CT扫描参数进行扫描的患者作为实验组,年龄(63.7±9.9)岁,男性48%,女性52%,心率(73.9±14.2)BPM。
本研究获医学伦理委员会批准,伦理号为TREC2022-KY035。
3.2 参数设置
定位像参数设置与模体扫描相同。两组钙化积分扫描均采用Care kV SEMI 120 kV、CareDose 4D ref.mAs 80 mAs,实验组与对照组ref.kV与参数设置分别为:100 kV与120 kV,余参数与模体扫描参数相同,选择曝光窗内冠脉显示最佳时相进行重建。两组患者钙化积分均行FBP、ADMIRE 3、ADMIRE 5三种重建算法进行重建。
3.3 辐射剂量评估
记录所有患者剂量长度乘积(DLP),根据公式(3)计算有效剂量(ED)。
$$ \mathrm{E}\mathrm{D}=\mathrm{D}\mathrm{L}\mathrm{P}\mathrm{x}0.014 ^{[5] } $$ (3) 3.4 钙化积分和风险分级
测量实验组患者不同重建算法图像的钙化积分,记录Agatston Score,并进行风险分级。分级标准[3]为:1级:0~1,为极低风险;2级:1~99,为低风险;3级:100~399,为中度风险;4级:大于400,为高风险。
3.5 图像质量客观评价
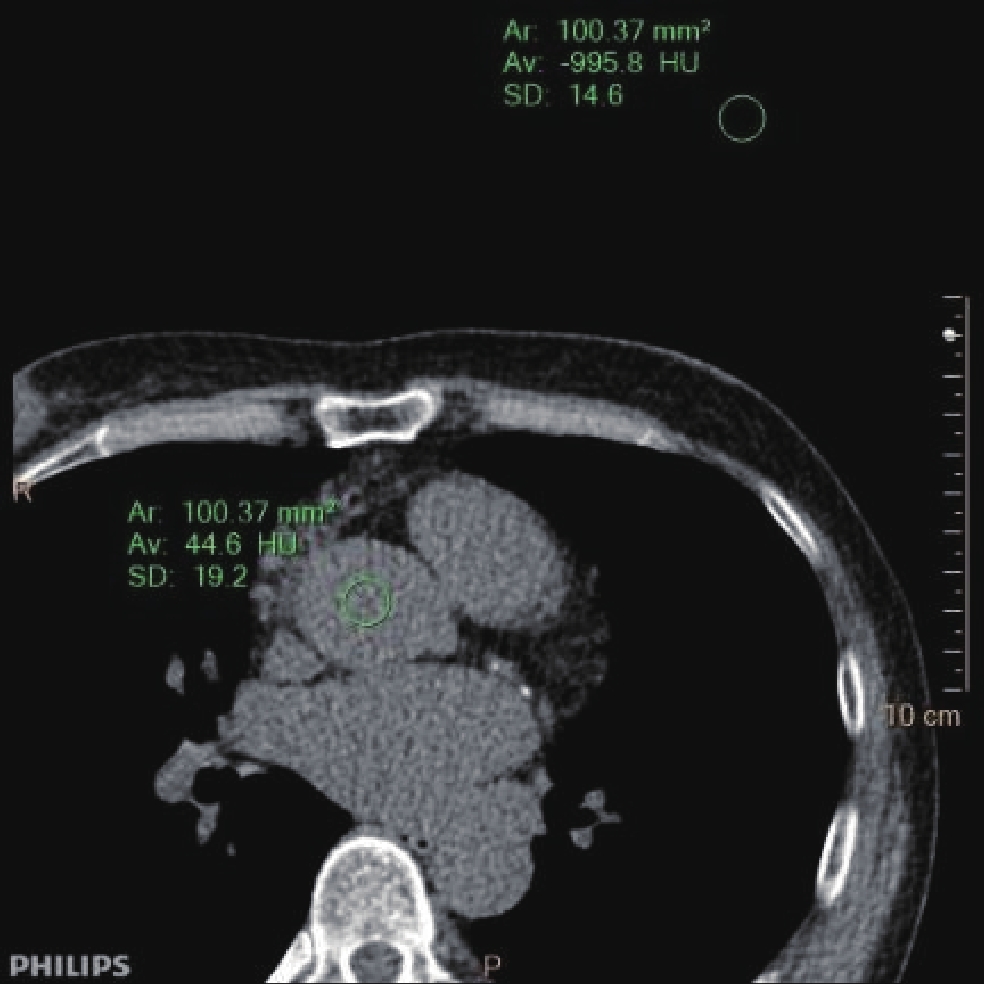
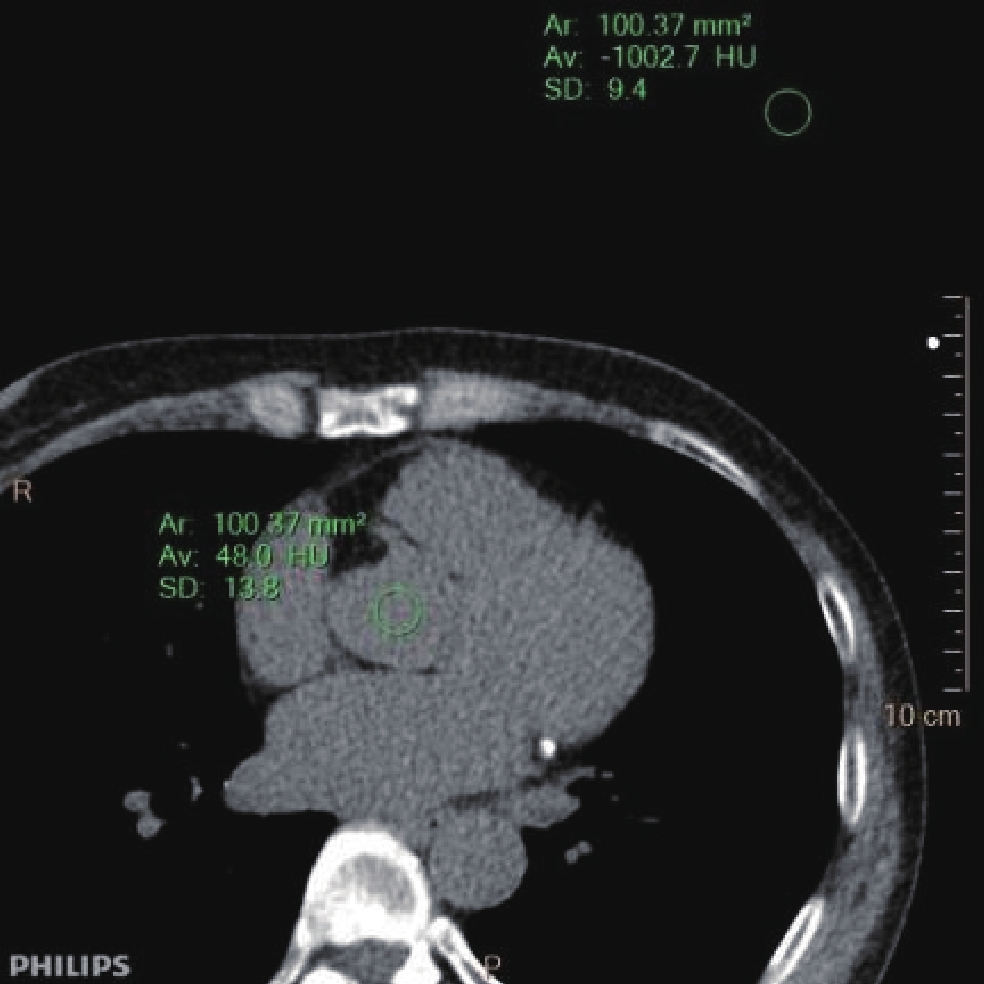
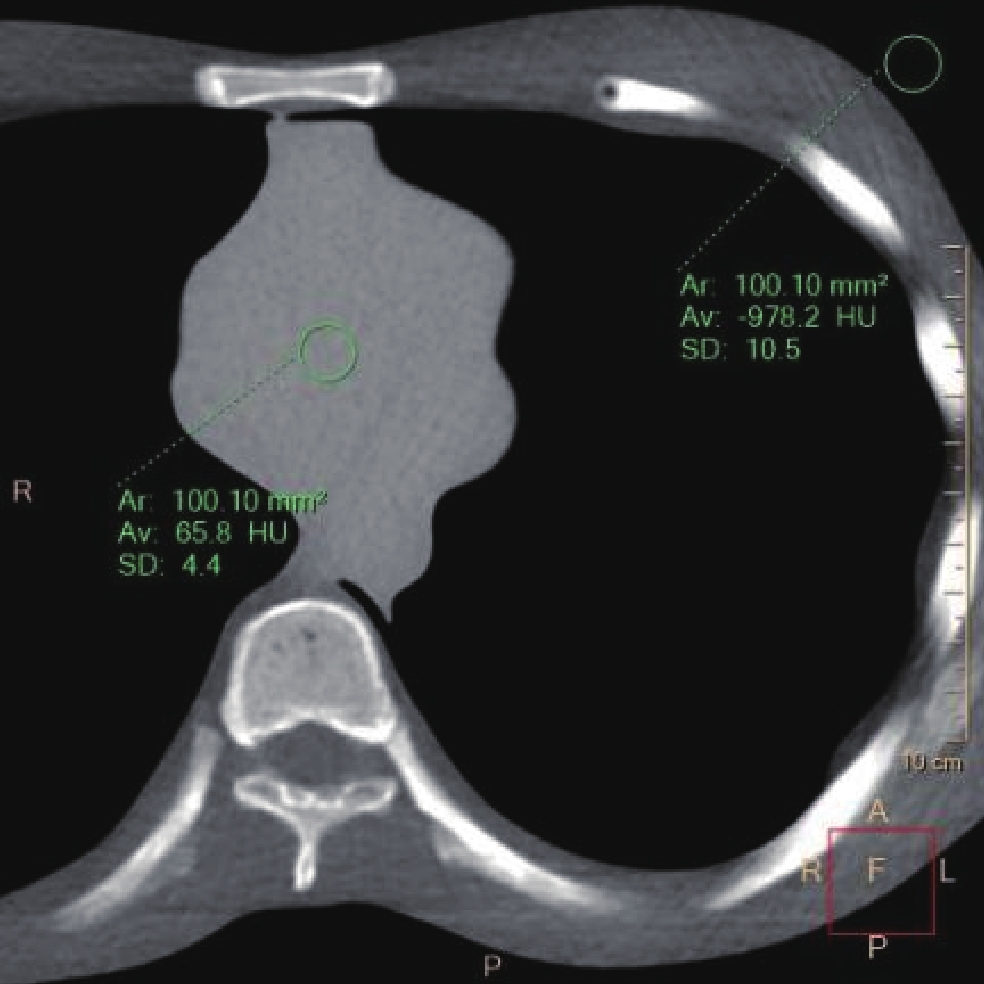
测量对照组和实验组患者图像,选择左主干(LM)与右冠状动脉(RCA)的起始处作为参考层面(图2、3),在两个层面的主动脉内(信号区)和胸壁上方空气区(背景区),勾画约100 mm2的圆形感兴趣区,分别测量CT主、CT空、SD空。根据公式(1)计算对比噪声比(CNR患)。
![]() 图 3 右冠状动脉(RCA)开口层面及感兴趣区位置Figure 3. Level of right coronary artery (RCA) opening and location of ROI
图 3 右冠状动脉(RCA)开口层面及感兴趣区位置Figure 3. Level of right coronary artery (RCA) opening and location of ROI3.6 图像质量主观评价
由两名高年资诊断医生对实验组患者冠脉钙化积分CT扫描图像进行主观评级,采用4分法:4分,钙化斑块边缘显示清晰;血管显示清楚,边缘锐利,无运动伪影;图像无噪声;3分,钙化斑块边缘显示比较清晰;血管显示略模糊,边缘比较锐利,有少量运动伪影;图像少量噪声;2分,钙化斑块边缘显示比较模糊,周边存在条带状伪影;血管显示模糊,存在运动伪影;图像有噪声,但不影响钙化积分评估;1分,钙化斑块边缘显示不清,有大量条带状伪影;血管变形,运动伪影较明显;图像噪声较大,无法诊断。统计检查成功数(评分≥2为成功,评分1为失败)。
3.7 统计分析
使用IBM SPSS Statistics 21进行数据分析。正态分布计量资料用
$ \bar{{x}}\pm s $ 表示,非正态分布计量资料用M(P25,P75)形式表示,计数资料用百分比表示。DLP、ED用两独立样本t检验,P < 0.05差异具有统计学意义。实验组三种算法钙化积分、实验组和对照组CNR患以及主观评分用多独立样本秩和检验,P < 0.05差异有统计学意义。进一步两两比较时,因经多个独立样本秩和检验,重复多次的假设检验将第1类错误α扩大,必须重新规定检验水准,其检验水准按公式(4)计算:$$ \mathrm{\alpha '=\alpha /N。} $$ (4) N为参加检验的组数。N=4(CNR患、主观评分),即新的检验水准为
0.0125 。实验组三种重建算法测得风险分级和两名医生对图像主观评分的一致性采用Kappa检验,Kappa值≤0.4为一致性差,0.4<Kappa值≤0.6为一致性中等,0.6<Kappa值≤1.0为一致性好。
4. 结果
4.1 模体研究结果
4.1.1 辐射剂量
胸部模体6组扫描的辐射剂量值见表1。CTDIvol最大值:9.76 mGy(ref.kV 120,ref.mAs 80),最小值3.01 mGy(ref.kV 100,ref.mAs 40)。6组扫描的实际管电压均为120 kV,实际辐射剂量数据表明:相同ref.kV数值,随着ref.mAs数值的增大,实际管电流和CTDIvol增大;相同ref.mAs数值下,随着ref.kV数值增大,实际管电流和CTDIvol增大。
表 1 模体扫描参数和辐射剂量Table 1. Phantom scanning parameters and radiation dose组别 管电压调制技术 参考管电压(kV) 参考管电流(mAs) 实际管电压(kV) 实际管电流(mAs) CTDIvol(mGy) A SEMI 120 kV 120 40 120 16 4.61 B SEMI 120 kV 120 60 120 26 7.02 C SEMI 120 kV 120 80 120 36 9.76 D SEMI 120 kV 100 40 120 10 3.01 E SEMI 120 kV 100 60 120 16 4.55 F SEMI 120 kV 100 80 120 22 5.88 4.1.2 图像质量和品质因数
图像质量:CNR模最大值为215.69(ref.kV 120 kV,ref.mAs 80,ADMIRE 5);最小值为87.83(ref.kV 100,ref.mAs 40,FBP)。B和C组、E组和F组在重建算法均为FBP时图像质量相当。同一组别CNR模随迭代算法等级增加而增加。
品质因数:FOM最大值为
8490.49 (ref.kV 100 kV,ref.mAs 40,ADMIRE 5);最小值为1717.57 (ref.kV 120 kV,ref.mAs 40,FBP)。同一组别FOM随迭代算法等级增加而增加。表 2 模体六种扫描参数四重建算法所得图像的CNR、FOM情况Table 2. CNR and FOM of the images of the four reconstruction algorithms under six scanning parameters组别 CNR 品质因数 FBP ADMIRE 3 ADMIRE 4 ADMIRE 5 FBP ADMIRE 3 ADMIRE 4 ADMIRE 5 A 88.98 108.07 120.39 141.25 1717.57 2533.50 3143.79 4328.09 B 125.96 160.27 182.34 215.80 2260.26 3659.17 4736.42 6633.60 C 137.27 167.78 185.44 215.69 1930.72 2884.16 3523.31 4766.79 D 87.83 115.91 130.23 159.86 2562.54 4463.66 5634.90 8490.49 E 110.69 139.88 158.69 193.29 2692.69 4300.41 5534.38 8211.29 F 112.99 134.51 149.68 174.18 2171.19 3076.86 3810.02 5159.66 注:FBP: 滤波反投影, ADMIRE: 全模型迭代重建算法,CNR: 对比噪声比,FOM:品质因数。 4.2 临床研究结果
4.2.1 辐射剂量
实验组与对照组实际扫描参数和辐射剂量统计值,见表3。实验组有效剂量最大值为3.39 mSv,最小值为0.83 mSv。
表 3 实际扫描参数和辐射剂量Table 3. Actual scanning parameters and radiation dose组别 实际管电压(kV) 实际管电流(mAs) DLP(mGy·cm) ED(mSv) 对照组 120 30(26,32) 243.54±83.27 3.40±1.16 实验组 120 28(24,32) 124.82±36.24 1.74±0.50 t 7.611 7.611 P < 0.001 < 0.001 4.2.2 实验组钙化积分和风险分级
实验组同一患者的钙化积分随重建算法等级增加而降低。不同重建算法下测得的钙化积分间无统计学差异(表4)。109例患者在进行风险分级时,有10位患者风险分级降低。FPB分别与ADMIRE 3组和ADMIRE 5组之间一致性较好,Kappa值分别为0.93、0.88。
表 4 实验组不同重建算法钙化积分Table 4. Calcium scores of the experimental group under different reconstruction algorithms组别 Agatston Score FBP 86.9(11.5,267.5) ADMIRE 3 75.4(10.3,242.6) ADMIRE 5 64(7.5,215.2) Z 1.593 P 0.451 4.2.3 图像质量评价
(1)客观评价:CNR患在LM和RCA层面上,对照组、实验FBP组、ADMIRE 3组和ADMIRE 5组,组间比较具有统计学差异。进一步两两比较,在两个层面上,对照组与实验FBP组均无统计学差异,P值分别为0.763、0.785。其余各组之间均具有统计学差异(表5)。
表 5 图像质量客观和主观评价结果Table 5. Results of objective and subjective evaluations of image quality分组 对比信噪比 主观评分* 左主干 右冠状动脉 对照组 94.96(82.70,109.46) 92.63(84.01,101.09) 4(4,4) 实验组FBP 93.38(81.42,108.00) 91.19(79.98,99.66) 3(3,3) 实验组ADMIRE 3 118.34(100.83,137.14) 117.20(101.46,127.70) 3(3,3) 实验组ADMIRE 5 158.14(133.46,188.40) 152.19(129.14,174.01) 4(4,4) Z 191.743 190.199 309.26 P < 0.001 < 0.001 < 0.001 注:主观评分*为两名医生评分合并后结果。 (2)主观评价:A、B两名医生评价一致性好,Kappa值为0.952。实验组与对照组图像主观评分均无失败患者,评分结果见表5。
5. 讨论
冠状动脉钙化(CAC)是冠状动脉粥样硬化进程中最主要的病理学改变之一,冠状动脉的钙化程度与心血管疾病的发病率有紧密联系。基于CT图像计算的冠状动脉钙化积分是量化分析冠状动脉钙化程度最常用的方法之一,常用的冠状动脉钙化诊断方法是在心电门控监测下进行心脏计算机断层扫描(MDCT),随着检查技术的不断更新和CT设备的快速发展,此种检查方法已逐渐成为一种常规检查项目,如何降低受检者辐射剂量已成为众多放射工作者的研究重点。
对于降低扫描计量,降低管电压是更有效的方法,并且可以增加对比度[6]。本研究采用的智能最佳管电压技术可以根据扫描条件预设的图像质量标准以及患者体型计算管电流变化曲线,扫描时选择球管允许的最低管电压,如果对应的管电流超出球管的最大范围,则自动选择次高的管电压值[7],可以根据患者体型进行个性化剂量调制,此种辐射剂量优化方式,在许多部位的CT检查中都得到了很好的应用[8]。
Agatston积分是基于管电压120 kV时钙化斑块的CT值计算得出,如果剂量优化过程中管电压改变则会引起钙化积分和风险分级的变化,风险分级的标准就需要进行重新界定[9,10]。因此在剂量优化过程中,采用Care kV SEMI模式,将实际输出管电压固定为120 kV,以确保钙化积分准确性,同时保证不同参考管电压所得图像具有可比性[11]。另外,本研究采用后门控采集技术,相较于传统的全时相后门控扫描,时相剂量调制的扫描方式(30%~80%采用全剂量扫描)已降低了辐射剂量,再加上优化后的扫描条件,有效剂量最低可达到0.83 mSv,实验组辐射剂量降低48%。由于心动周期时相的选取对于钙化积分的测量起到至关重要的作用[12],前瞻性钙化积分扫描方式需谨慎使用。
由于降低参考管电压降低了图像质量水平,联合应用全模型迭代重建算法,可以在降低辐射剂量的同时,保证图像质量[13]。ADMIRE 算法是全模型迭代重建算法,其对比校正模型完善。通过多次迭代,能在低扫描条件下重建出满足诊疗需求的图像[9]。模体实验中,ref.kV 100 + ref.mAs 80组辐射剂量较对照组降低约39.8%,FBP组图像质量与对照组相当,因此选定Care kV SEMI 120 kV(ref.kV 100 + ref.mAs 80)作为临床实验组患者采集参数,在固定管电压为120 kV的前提下,保证CT值和图像质量不变的情况下降低辐射剂量。同一扫描条件下,模体图像CNR随迭代算法等级增加而增加,进而FOM随之增加。在临床研究中,左主干和右冠开口图像的CNR呈现与模体结果相一致的规律。相较于FBP图像,ADMIRE 3两层面CNR分别升高约26.7%、28.5%,ADMIRE 5两层面CNR分别升高约69.4%、66.9%。但是,随着CNR升高钙化积分呈现降低趋势,高等级迭代算法的使用会对Agatston积分产生影响[13-15]。由于ADMIRE算法间接影响了钙化斑块的最高CT值,导致Agatston积分计算过程中涉及的权重系数降低,最终导致钙化积分值降低。龙斌[17]等人研究不同的迭代算法下钙化积分存在统计学差异,与本研究相反,分析原因可能是其研究使用了SAFIRE算法,而本研究中使用的是ADMIRE算法,在SAFIRE算法基础上增加了模型域的迭代,有利于进一步提高精确度[18]。本研究中有10位患者风险分级发生了改变,迭代算法的使用导致钙化积分降低,进而导致风险分级降低[19],与Marwan[20]的研究结果相同。其中6位患者(6%)风险等级改变发生在重建算法由FBP变为ADMIRE 3时,4位患者(4%)发生在重建算法由ADMIRE 3变为ADMIRE 5时。但相较于FBP图像,两种迭代算法图像的风险等级与FBP图像一致性很高,尤其ADMIRE 3可达到93%。进一步分析,如果高迭代等级对于钙化积分风险分级影响较小,但又可以显著提高图像质量,回顾模体实验中辐射剂量最低的ref.kV 100+ref.mAs 40组图像,迭代等级为5时,其CNR仍然优于对照组图像质量,此时辐射剂量降低约64%。临床研究的扫描参数是否有进一步优化的空间,有待下一步研究。
本研究的局限性在于:首先,模体研究只模拟心率为60次/分的采集时相,可能对临床研究的采集时相产生影响;其次,本研究仅针对BMI18-25的患者,以保证衰减特性尽量与模体相当,此结论对于超重或者肥胖患者并不一定适合。
综上所述,BMI18-25患者进行冠脉钙化积分CT扫描时,可以通过CARE kV SEMI模式联合迭代算法来降低辐射剂量,对图像质量不会产生影响。
-
![]()
图 3 右冠状动脉(RCA)开口层面及感兴趣区位置
Figure 3. Level of right coronary artery (RCA) opening and location of ROI
表 1 模体扫描参数和辐射剂量
Table 1 Phantom scanning parameters and radiation dose
组别 管电压调制技术 参考管电压(kV) 参考管电流(mAs) 实际管电压(kV) 实际管电流(mAs) CTDIvol(mGy) A SEMI 120 kV 120 40 120 16 4.61 B SEMI 120 kV 120 60 120 26 7.02 C SEMI 120 kV 120 80 120 36 9.76 D SEMI 120 kV 100 40 120 10 3.01 E SEMI 120 kV 100 60 120 16 4.55 F SEMI 120 kV 100 80 120 22 5.88  下载: 导出CSV
下载: 导出CSV
表 2 模体六种扫描参数四重建算法所得图像的CNR、FOM情况
Table 2 CNR and FOM of the images of the four reconstruction algorithms under six scanning parameters
组别 CNR 品质因数 FBP ADMIRE 3 ADMIRE 4 ADMIRE 5 FBP ADMIRE 3 ADMIRE 4 ADMIRE 5 A 88.98 108.07 120.39 141.25 1717.57 2533.50 3143.79 4328.09 B 125.96 160.27 182.34 215.80 2260.26 3659.17 4736.42 6633.60 C 137.27 167.78 185.44 215.69 1930.72 2884.16 3523.31 4766.79 D 87.83 115.91 130.23 159.86 2562.54 4463.66 5634.90 8490.49 E 110.69 139.88 158.69 193.29 2692.69 4300.41 5534.38 8211.29 F 112.99 134.51 149.68 174.18 2171.19 3076.86 3810.02 5159.66 注:FBP: 滤波反投影, ADMIRE: 全模型迭代重建算法,CNR: 对比噪声比,FOM:品质因数。
下载: 导出CSV
表 3 实际扫描参数和辐射剂量
Table 3 Actual scanning parameters and radiation dose
组别 实际管电压(kV) 实际管电流(mAs) DLP(mGy·cm) ED(mSv) 对照组 120 30(26,32) 243.54±83.27 3.40±1.16 实验组 120 28(24,32) 124.82±36.24 1.74±0.50 t 7.611 7.611 P < 0.001 < 0.001
下载: 导出CSV
表 4 实验组不同重建算法钙化积分
Table 4 Calcium scores of the experimental group under different reconstruction algorithms
组别 Agatston Score FBP 86.9(11.5,267.5) ADMIRE 3 75.4(10.3,242.6) ADMIRE 5 64(7.5,215.2) Z 1.593 P 0.451
下载: 导出CSV
表 5 图像质量客观和主观评价结果
Table 5 Results of objective and subjective evaluations of image quality
分组 对比信噪比 主观评分* 左主干 右冠状动脉 对照组 94.96(82.70,109.46) 92.63(84.01,101.09) 4(4,4) 实验组FBP 93.38(81.42,108.00) 91.19(79.98,99.66) 3(3,3) 实验组ADMIRE 3 118.34(100.83,137.14) 117.20(101.46,127.70) 3(3,3) 实验组ADMIRE 5 158.14(133.46,188.40) 152.19(129.14,174.01) 4(4,4) Z 191.743 190.199 309.26 P < 0.001 < 0.001 < 0.001 注:主观评分*为两名医生评分合并后结果。
下载: 导出CSV
-
[1] 王俊琴, 刘太峰, 张海燕. 智能最佳管电压联合自动管电流在降低胸部CT扫描剂量中的应用[J]. 临床放射学杂志, 2019, 38(5): 931-935. WANG J Q, LIU T F, ZHANG H Y, et al. Application of the technique of CARE kV combined with CARE dose 4D in reducing radiation dosage of chest CT scanning[J]. Journal of Clinical Radiology, 2019, 38(5): 931-935. (in Chinese).
[2] 《中国心血管健康与疾病报告》编写组. 《中国心血管健康与疾病报告2020》概述[J]. 中国心血管病研究, 2021, 19(7): 582-590. DOI: 10.3969/j.issn.1672-5301.2021.07.002. [3] SCHERNTHANER R E, HAROUN R R, NGUYEN S, et al. Characteristics of a new x-ray imaging system for interventional procedures: improved image quality and reduced radiation dose[J]. Cardiovasc Intervent Radiol, 2018, 41(3): 502-508. DOI: 10.1007/s00270-017-1821-z.
[4] 吴杰, 陆再英, 徐春芳, 等. 中国健康人群正常心率范围的调查[J]. 中华心血管病杂志, 2001, 29(6): 369-371. DOI: 10.3760/j:issn:0253-3758.2001.06.011. WU J, LU Z Y, XU C F, et al. Investigation of the normal heart rate limits of the Chinese[J]. Chinese Journal of Cardiology, 2001, 29(6): 369-371. DOI: 10.3760/j:issn:0253-3758.2001.06.011.
[5] The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Annals of the International Commission on Radiological Protection. 2007;37(2-4): 1-332. DOI: 10.1016/j.icrp.2007.10.003.
[6] 冯梦雅, 李冰, 吴敏, 等. 基于AI的新迭代重建算法与低管电压在降低肥胖患者冠状动脉CTA辐射剂量中的应用[J]. CT理论与应用研究, 2023, 32(6): 777-782. DOI: 10.15953/j.ctta.2022.148. FENG M Y, LI B, WU M, et al. Application of new iterative reconstruction algorithm based on artificial intelligence and low tube voltage in reducing the radiation dose of coronary CTA in obese patients[J]. CT Theory and Applications, 2023, 32(6): 777-782. DOI: 10.15953/j.ctta.2022.148. (in Chinese).
[7] 徐卓东. CARE kV—智能最佳kV扫描技术——降低剂量的同时提高图像质量[J]. 中国医疗设备, 2012, 27(02): 120-123. DOI: 10.3969/j.issn.1674-1633.2012.02.037. XU Z D. CARE kV—Intelligent optimal kV Scanning Technology: Reducing x-ray dose and improVing CT image quality synchronously[J]. China Medical Devices, 2012, 27(02): 120-123. DOI: 10.3969/j.issn.1674-1633.2012.02.037.
[8] 王俊琴, 刘太峰, 张海燕. 智能最佳管电压联合自动管电流在降低胸部CT扫描剂量中的应用[J]. 临床放射学杂志, 2019, 38(05): 931-935. WANG J Q, LIU T F, ZHANG H Y. Application of the technique of CARE kV combined with CARE dose 4D in reducing radiation dosage of chest CT scanning[J]. Journal of Clinical Radiology, 2019, 38(05): 931-935. (in Chinese).
[9] 樊荣荣, 施晓雷, 钱懿等. 应用全模型迭代重组技术的非门控胸部低剂量CT平扫一站式筛查对冠状动脉钙化积分危险度分层的准确性评价[J]. 临床放射学杂志, 2019, 38(03): 547-552. FAN R R, SHI X L, QIAN Y, et al. Assessment of the accuracy of risk stratification of coronary ccalcification by non-gated low-llose chest CT using IMR Technique[J]. Journal of Clinical Radiology, 2019, 38(03): 547-552. (in Chinese).
[10] NAKAZATO R, DEY D, GUTSTEIN A, et al. Coronary artery calcium scoring using a reduced tube voltage and radiation dose protocol with dual-source computed tomography[J]. Journal Of Cardiovascular Computed Tomography, 2009, 3(6): 394-400. DOI: 10.1016/j.jcct.2009.10.002.
[11] ZHANG J, KANG S, HAN D, et al. Application of intelligent optimal kV scanning technology (CARE kV) in dual-source computed tomography (DSCT) coronary angiography[J]. International Journal of Clinical and Experimental Medicine, 2015, 15;8(10): 17644-53.
[12] 汤化民, 苟杰, 林伟等. 心脏CT重建时相对冠状动脉钙化积分危险分级的影响[J]. 中国医学影像技术, 2021, 37(01): 50-53. DOI: 10.13929/j.issn.1003-3289.2021.01.011. TNG H M, GOU J, LIN W, et a1. Impact of cardiac CT reconstruction time interyal on risk stratification of coronary artery calcium scoring[J]. Chinese Journal of Medical Imaging Technology. 2021, 37(01): 50-53. DOI: 10.13929/j.issn.1003-3289.2021.01.011.(in Chinese).
[13] CHOI A D, LEIFER E S, YU J H, ET A1. Reduced radiation dose with model based iterative reconstruction coronary artery calcium scoring[J]. European Journal of Radiology, 2019, 111: 1-5. DOI: 10.1016/j.ejrad.2018.12.010.
[14] WILLEMINK M J, DE JONG P A, LEINER T, et al. Iterative reconstruction techniques for computed tomography Part 1: technical principles[J]. European Radiology, 2013, 23: 1623-1631. DOI: 10.1007/s00330-012-2765-y.
[15] 张卓璐, 刘卓, 洪楠. 混合迭代重建混合权重对心脏CT冠状动脉钙化积分影响[J]. 放射学实践, 2021, 36(06): 751-755. DOI: 10.13609/j.cnki.1000-0313.2021.06.012. ZHANG Z L, LIU Z, HING N. Impact of hybrid iterative reconstruction blending weight on coronary artery calcium score based on cardiac CT[J]. Radiologic. Practice, 2021, 36(06): 751-755. DOI: 10.13609/j.cnki.1000-0313.2021.06.012.
[16] FAN R, SHI X, QIAN Y, et al. Optimized categorization algorithm of coronary artery calcification score on non-gated chest low-dose CT screening using iterative model reconstruction technique[J]. Clinical Imaging, 2018, 52: 287-291. DOI: 10.1016/j.clinimag.2018.08.015.
[17] 龙斌, 宋少辉, 刘怡等. SAFIRE算法对冠状动脉钙化积分的影响[J]. 临床放射学杂志, 2018, 37(07): 1117-1120. LONG B, SONG S H, LIU Y, ET A1. The impact of sinogram-affirmed iterative reconstruction algorithms on coronary calcium scoring[J]. Journal of Clinical Radiology, 2018, 37(07): 1117-1120. (in Chinese).
[18] 谢刚, 邓晓凤, 刘璐思等. 双源CT实时迭代ADMIRE重建技术在肝脏CT扫描中的应用价值[J]. 中国社区医师, 2020, 36(7): 132, 134. DOI: 10.3969/j.issn.1007-614x.2020.07.079. XIE G, DENG X F, LIU L S, et a1. Application value of FORCE CT real-time iterative ADMIRE reconstruction technology in liver CT scanning[J]. Chinese Community Doctors, 2020, 36(7): 132, 134. , 2020, 36(7): 132, 134. DOI: 10.3969/j.issn.1007-614x.2020.07.079.(in Chinese).
[19] MESSERLI M, RENGIER F, DESBIOLLES L, ET A1. Impact of advanced modeled iterative reconstruction on coronary artery calcium quantification[J]. Academic Radiology, 2016, 23(12): 1506-1512. DOI: 10.1016/j.acra.2016.08.008.
[20] MARWAN M, METTIN C, PFLEDERER T, ET A1. Very low-dose coronary artery calcium scanning with high-pitch spiral acquisition mode: comparison between 120-kV and 100-kV tube voltage protocols[J]. Journal of Cardiovascular Computed Tomography, 2013, 7(1): 32-8. DOI: 10.1016/j.jcct.2012.11.004.





计量
- 文章访问数: 19
- HTML全文浏览量: 2
- PDF下载量: 3


