
Deep Learning Computer-aided Diagnostic Model for Non-small Cell Lung Cancer Based on Convolutional Neural Network and Attention Mechanism
-
摘要:
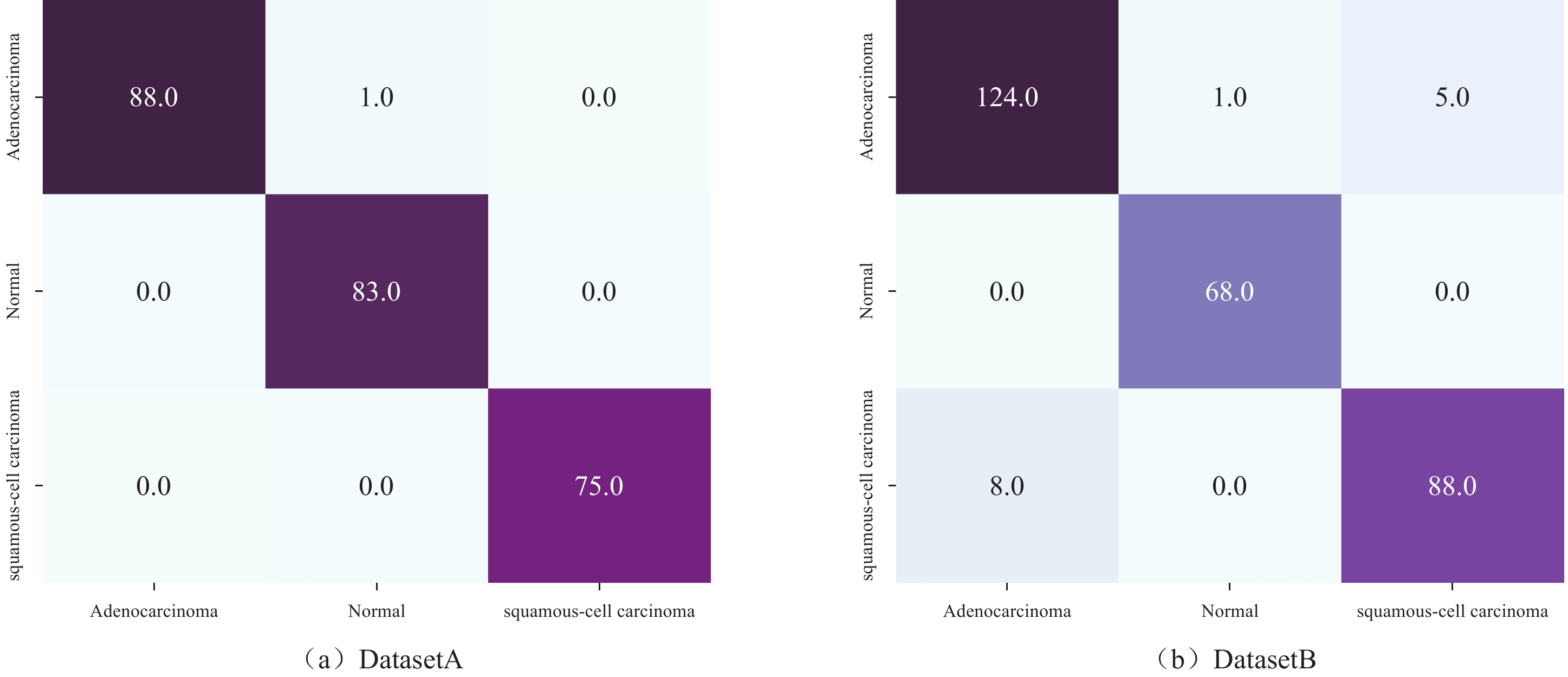
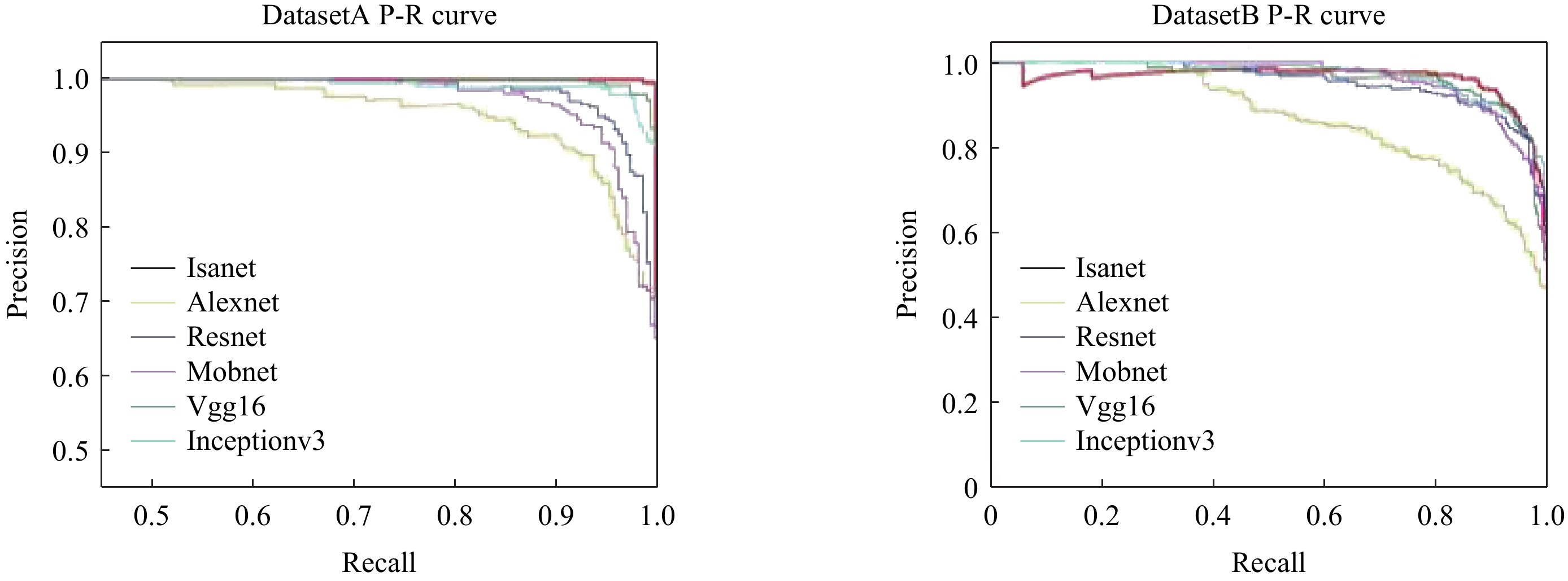
目的:构建基于卷积神经网络(CNN)和注意力机制的改进CNN模型(ISANET),评估模型的性能,并与传统CNN模型进行比较。方法:收集经手术病理证实的肺鳞癌(LUSC)或肺腺癌(LUAD)患者60例以及肺部正常患者30例的肺部CT平扫或增强图像共619张,组成DatasetA;收集公共数据集图像共737张,组成DatasetB。两数据集均按6∶4将随机分为训练集和测试集。构建ISANET模型并进行训练和验证,然后记录查准率、召回率,并计算出F1分数,用以评价ISANAT模型的效能。最后,将ISANET模型与传统CNN模型AlexNet,VGG 16,Inception V3,Mobilenet V2,ResNet 18进行对比,绘制P-R(P-R)曲线,计算出P-R曲线下面积,并评估不同模型对肺鳞癌和肺腺癌的鉴别效能。结果:相较于传统CNN模型,ISANET模型对非小细胞肺癌分类的准确度明显提高,在DatasetA和DatasetB中分别为99.6%和95.2%。结论:ISANET模型较好地实现了对肺鳞癌和肺腺癌的无创预测,提高了肺鳞癌和肺腺癌CT影像鉴别的准确度,能够帮助诊断医师对非小细胞肺癌进行快速准确的分类。
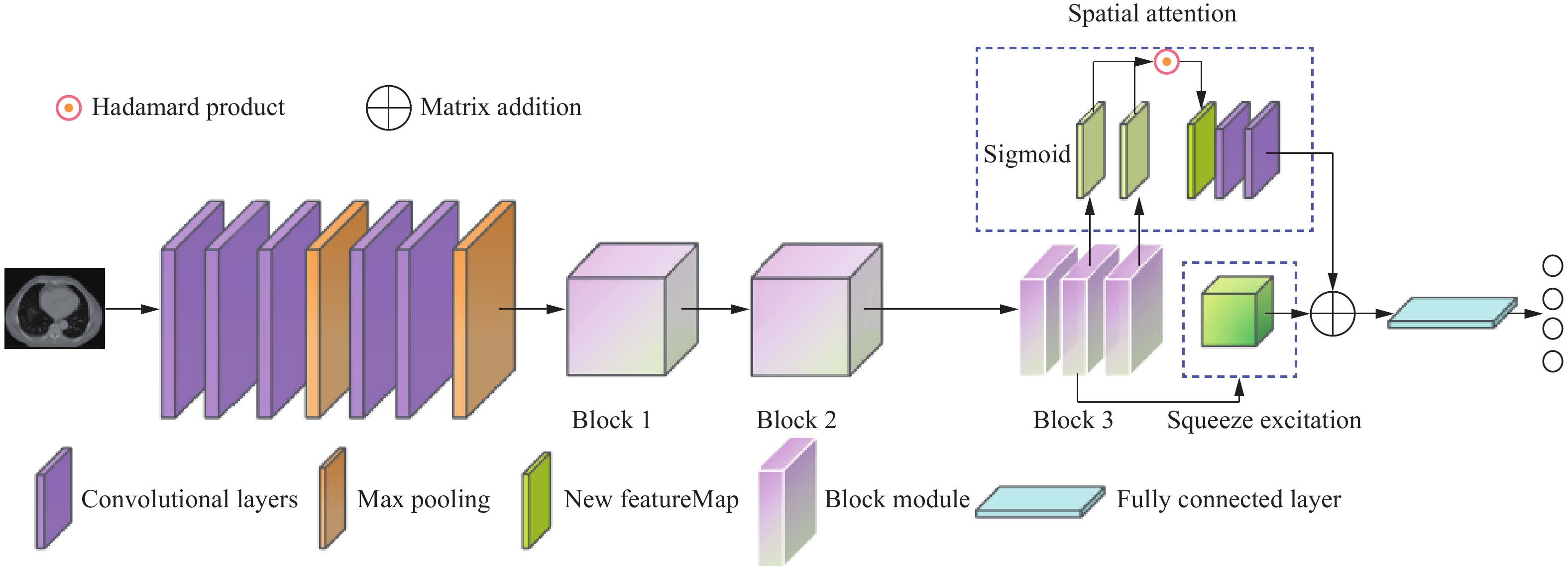
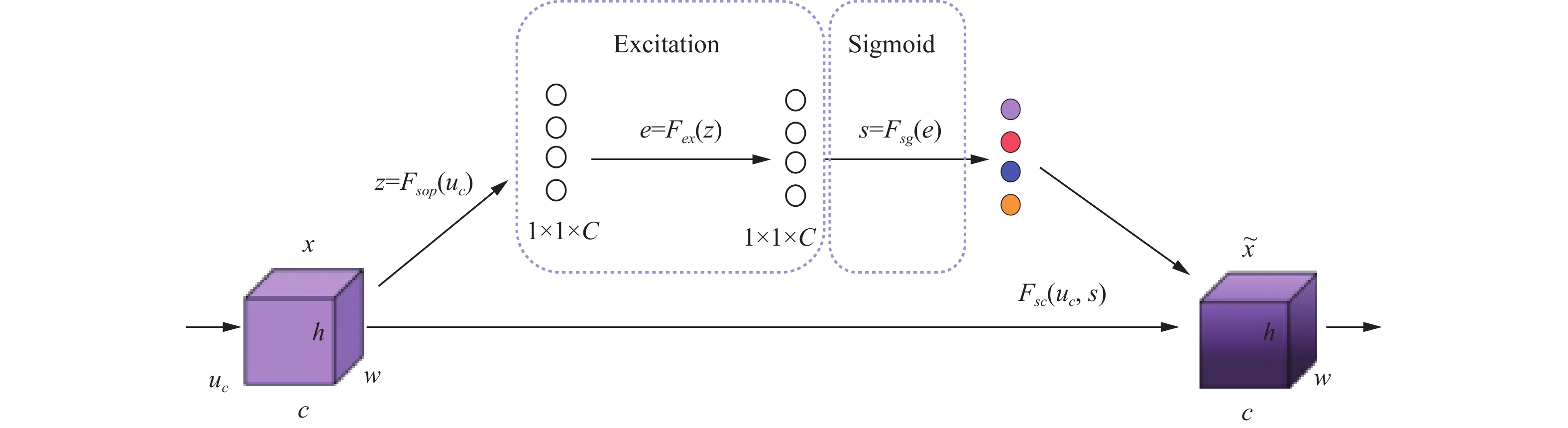
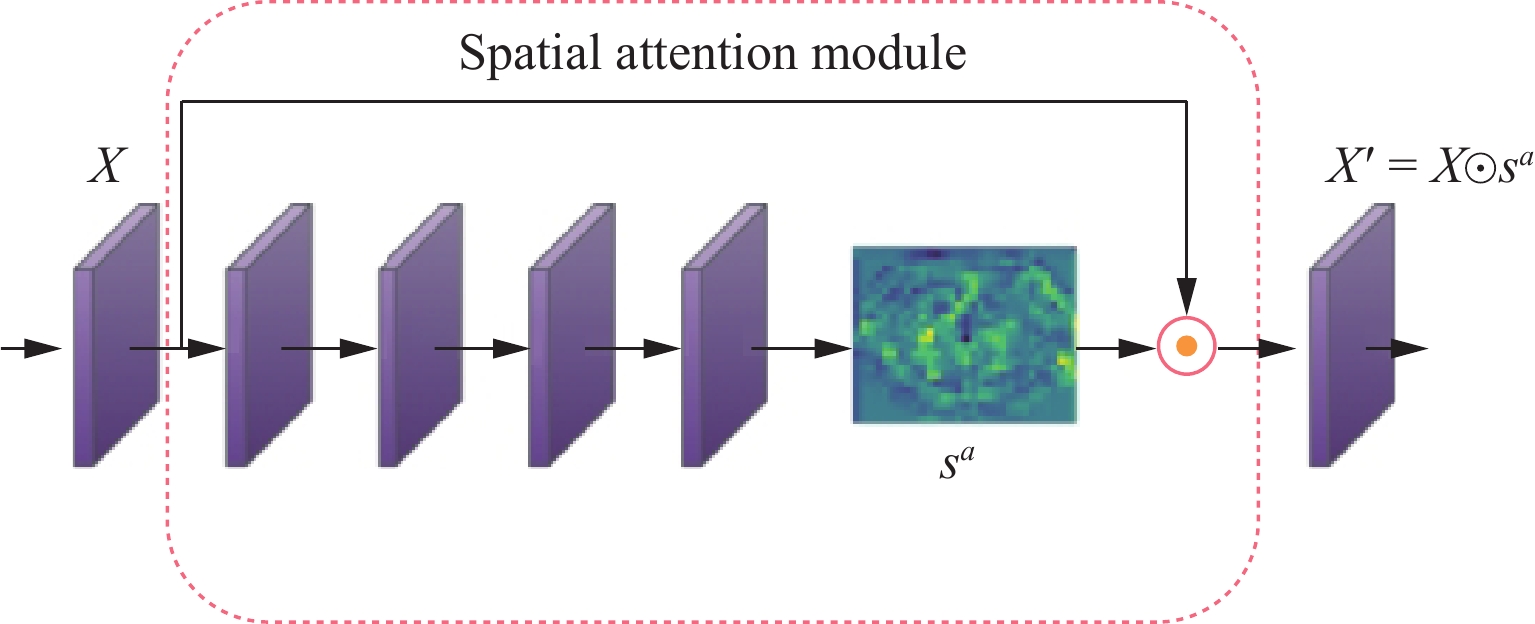
Abstract:Objective: To construct an improved deep learning computer-aided diagnosis model based on convolutional neural network (CNN) and Attention Mechanism proposed as Inception Spatial and Channel Attention Network (ISANET) and evaluate the model's performance, comparing it with the traditional CNN model. Methods: A total of 619 lung CT images of 60 patients with lung squamous cell carcinoma or lung adenocarcinoma confirmed by surgical pathology and 30 patients with normal lungs were collected retrospectively to form Dataset A; a total of 737 public dataset images were collected to form Dataset B. The two datasets were randomly divided into training and test sets at a 6:4 ratio. Construct the ISANET model and conduct training and verification, then record the precision ratio and recall ratio to calculate the F1 score and evaluate the performance of the ISANAT model. Finally, the ISANET model was compared with the traditional CNN models such as AlexNet, VGG16, InceptionV3, MobilenetV2, and ResNet18 by drawing the Precision-Recall (P-R) curve and calculating the area under the P-R curve to evaluate the classification performance of different models for LUSC and LUAD. Results: Compared with the traditional CNN model, the accuracy of the ISANET model for non-small cell lung cancer classification improved significantly, reaching 99.6% and 95.2% in Dataset A and Dataset B, respectively. Conclusions: The ISANET model provides better non-invasive prediction of LUSC and LUAD, improves the accuracy of CT imaging identification of lung squamous cell carcinoma and lung adenocarcinoma, and can help diagnosticians quickly and accurately classify non-small cell lung cancer.
-
Keywords:
- non-small cell lung cancer /
- CNN /
- attention mechanisms /
- computer-aided diagnosis
-
颅内孤立性纤维瘤(intracranial solitary fibrous tumor,ISFT)是一种间叶组织来源的梭形细胞肿瘤,发病罕见,尽管近年来国内外相关报道的病例逐渐增多,但是影像及临床医生对其仍缺乏全面认识,术前误诊率高。
本文介绍1例经术后病理证实的颅内孤立性纤维瘤,结合其病例资料进行相关分析,以提高医生对此种罕见病的术前诊断准确率,对手术方案制定及预后有重要价值,具有报道意义。
1. 病例资料
1.1 临床资料
患者,男,52岁,因“双下肢无力,步态不稳20天”入院。入院前10年无明显诱因出现头痛,自行口服药物治疗,未系统治疗。近20天感下肢行走无力,伴踩棉花感,发病以来精神食欲及睡眠较差,大小便正常。
1.2 实验室检查
白蛋白37.3↓(40~55 g/L),天门冬氨酸转移酶9.8↓(15~40 U/L),胱抑素C 1.49↑(0~1.4 mg/L),补体C1 q138.9↓(159~233 mg/L);余(-)。
1.3 影像学表现
CT:平扫左侧桥小脑角区片状低密度影(图1)。MRI:左侧桥小脑角区听神经根部可见大小约4.3 cm×5.9 cm×4.8 cm,囊实性混杂信号影,实性部分T1WI、T2WI呈混杂信号,边界清晰,边缘欠规整,DWI呈混杂信号。增强扫描实性成分呈不均匀明显持续性强化(图2),听神经增粗,左侧内听道扩大。影像诊断为左侧听神经瘤。
![]() 图 1 ISFT患者CT平扫图像(a)和(b)轴位CT平扫示左侧桥小脑角区片状低密度影(红箭),周围水肿明显,左侧内听道扩大(蓝箭)。Figure 1. CT plain scan of the patient with ISFT
图 1 ISFT患者CT平扫图像(a)和(b)轴位CT平扫示左侧桥小脑角区片状低密度影(红箭),周围水肿明显,左侧内听道扩大(蓝箭)。Figure 1. CT plain scan of the patient with ISFT![]() 图 2 ISFT患者MRI平扫及增强图像(a)~(c)MRI平扫示左侧桥小脑角区听神经根部大小约4.3 ㎝×5.9 ㎝×4.8 ㎝囊实性混杂信号影(红箭),实性部分T1WI(a)、T2WI(b)呈混杂信号,边界清晰,边缘欠规整,DWI(c)呈混杂信号,听神经增粗,左侧内听道扩大,邻近脑实质及第四脑室受压推移,瘤周水肿明显,并可见流空血管影;(d)~(g)增强扫描图像,(d)和(e)为轴位,(f)和(g)分别为矢状位和冠状位,肿瘤实性成分呈不均匀明显持续性强化(红箭),窄基底与硬脑膜相连,T2WI低信号区强化明显。Figure 2. MRI plain and contrast-enhanced images of the patient with ISFT
图 2 ISFT患者MRI平扫及增强图像(a)~(c)MRI平扫示左侧桥小脑角区听神经根部大小约4.3 ㎝×5.9 ㎝×4.8 ㎝囊实性混杂信号影(红箭),实性部分T1WI(a)、T2WI(b)呈混杂信号,边界清晰,边缘欠规整,DWI(c)呈混杂信号,听神经增粗,左侧内听道扩大,邻近脑实质及第四脑室受压推移,瘤周水肿明显,并可见流空血管影;(d)~(g)增强扫描图像,(d)和(e)为轴位,(f)和(g)分别为矢状位和冠状位,肿瘤实性成分呈不均匀明显持续性强化(红箭),窄基底与硬脑膜相连,T2WI低信号区强化明显。Figure 2. MRI plain and contrast-enhanced images of the patient with ISFT1.4 诊疗过程
手术记录:术中见肿瘤色淡红,包膜完整,血供丰富,肿瘤向上方生长到小脑幕孔,压迫脑干,与脑干粘连紧密,并包绕面神经。
术后病理:脑部梭形细胞肿瘤(图3),免疫组化结果支持孤立性纤维性肿瘤。免疫组化结果:Vim(+),GFAP(-),CD34(+),EMA(-),CK(-),S-100(-),SMA(-),Calponin(-),CD31(-),Bcl-2(+),CD99(少部分+),CD68(散+),Lysozyme(散+),P53(-),Ki-67(+3~5%)。
![]() 图 3 ISFT患者术后病理图像(a)和(b)镜下肿瘤细胞呈梭形,稀疏区与密集区交替分布(HE,×200)。Figure 3. Postoperative pathological images of the patient with ISFT
图 3 ISFT患者术后病理图像(a)和(b)镜下肿瘤细胞呈梭形,稀疏区与密集区交替分布(HE,×200)。Figure 3. Postoperative pathological images of the patient with ISFT1.5 随访
患者术后1年半门诊复查,左侧面神经麻痹,左侧面部憋胀,余无明显不适。
2. 讨论
孤立性纤维瘤(solitary fibrous tumor,SFT)是一种间叶组织来源的梭形细胞肿瘤,起源于结缔组织中的CD34阳性的树突状细胞,既可发生于胸膜腔,也可发生于全身各部位,如肝脏、腹膜、头颈部等。颅内孤立性纤维瘤由Carneiro等[1]于1996年首先报道,发病率极低,目前国内外文献报道相关病例较少。
2021年WHO中枢神经系统肿瘤将其划分为间叶性非脑膜上皮肿瘤,分为Ⅰ~Ⅲ 级;核分裂象<5/10 HPF时,若镜下有致密胶原纤维伴相对较低密度的梭形细胞则为Ⅰ级,若梭形肿瘤细胞多而胶原较少,且有“鹿角”状脉管系统则为Ⅱ级,核异型性明显,核分裂象≥5/10个高倍镜视野(high power field,HPF)时,为 Ⅲ 级。该分类取消了2016版“孤立性纤维瘤/血管外皮细胞瘤(hemangiopericytoma,HPC)”的混合术语,并将所谓HPC合并于“孤立性纤维瘤”[2-3]。
2.1 病因及发病机制
孤立性纤维瘤的病因及发病机制尚不明确,Miettinen等[4]认为SFT的发生可能与环境因素或基因变异相关,其可能的机制是包含NAB2-STAT6融合基因的染色体12q13臂内倒置。
2.2 临床特征
ISFT在人群中的发病率并无显著性别差异,可发生于任何年龄段,以51~60岁年龄组占比最大,本例ISFT为中老年男性,发病年龄与以往文献报道一致。ISFT大多位于小脑幕(16%),其次是大脑额凸、桥小脑角区(CPA)、脑室、大脑镰和颅后窝[5]。
临床表现依据病程和发生的部位不同表现各异,初期可无明显症状,肿瘤体积增大时发生在幕上常有头痛、头晕、恶心、呕吐、癫痫等症状;幕下可有听力下降、脑干受压或行走不稳等症状。本例发生于左侧桥小脑角区,双下肢无力,步态不稳,符合幕下ISFT临床特征。
2.3 CT与MRI影像学表现
CT平扫检查ISFT表现为孤立性、实质性肿块,多呈圆形、类圆形,一般体积较大,边界多光整,境界清楚,无分叶或浅分叶,呈软组织密度,囊变坏死区呈低密度,钙化少见。增强扫描病灶实性部分明显强化,体积较大时可见无强化的囊变坏死区[6]。
MRI检查具有良好的软组织分辨能力,在ISFT诊断中具有明显优势。T1WI多呈等低或等信号,T2WI可表现为高信号、稍高信号或低信号。T2WI上出现高低信号混杂的现象称为“阴阳征”或“黑白征”,是影像诊断ISFT一个相当重要的典型征象,即高信号区反映黏液坏死变性及血管间质细胞堆积,稍高信号区反映肿瘤细胞密集区域,低信号区反映致密胶原纤维[7-8]。动态增强扫描肿瘤多为不均匀持续性强化或进行性延迟强化,T2WI低信号区明显强化[9-10]。
此外,ISFT由于瘤体及瘤周血运丰富,常出现流空血管影,也是典型征象之一。但是部分脑膜瘤也可见血管流空,区别在于ISFT多表现为“蛇形流空效应”,而脑膜瘤以“光芒征”多见,其原因是ISFT主要来源于颈内动脉或椎动脉分支供血,而脑膜瘤主要来源于颈外动脉的脑膜中动脉供血[11-12],因此可以为二者鉴别诊断提供思路。部分ISFT可见“脑膜尾征”,但该征象少见,不具有特异性,只能说明肿瘤与硬脑膜关系密切,并不能对肿瘤来源进行鉴别。
本例患者出现“阴阳征”与流空血管影,并且肿瘤以窄基底与硬膜相连,呈“脑膜尾征”,符合文献报道。
2.4 诊断与鉴别诊断
尽管颅内孤立性纤维瘤患者的MRI表现具有相对特异性,但是未出现“阴阳征”等典型表现时较难做出明确诊断,确诊依赖于病理及免疫组织化学检查。ISFT病理主要表现为梭形细胞呈束状或不规则排列在透明样病变血管周围,伴有宽大的胶原纤维[13]。免疫组化检查常表现为CD34(+)、Bcl-2(+)和Vimentin(+);EMA(-)和S-100(-)[14],其中CD34可作为特异性免疫标志物之一,本例患者免疫组化结果与文献一致,符合颅内孤立性纤维瘤诊断。
随着对SFT的深入研究,有学者发现STAT6诊断SFT有高度敏感性和特异性[15],STAT6与CD34等传统标记物联合诊断SFT可能成为新趋势。
ISFT在影像学上主要与脑膜瘤、神经鞘瘤和转移瘤等鉴别。①脑膜瘤:起源于蛛网膜帽状细胞,多呈圆形或类圆形,CT平扫肿瘤多为均匀的略高密度,钙化多见,相邻颅骨可见增生,增强扫描肿瘤呈均匀一致的显著强化,边缘锐利;在T1WI上多数为等信号,少数低信号,T2WI可为高、等或低信号,增强扫描明显均匀强化并有“脑膜尾征”。而ISFT信号多不均匀,稍高信号内可见小片状低信号,不均匀持续性强化或进行性延迟强化;相邻颅骨可有侵蚀,增生少见。②神经鞘瘤:ISFT发生于桥小脑角区时需与听神经鞘瘤鉴别,后者可见特征性桥小脑角区“冰激凌征”,与周围组织分界清楚,囊变坏死多见,多呈不均匀T1WI低、T2WI高信号,增强扫描实性部分明显强化,较早出现颅神经功能缺损症状。本例患者肿瘤发生于桥小脑角区,影像可见听神经增粗、内听道扩大等表现,故术前误诊为听神经瘤。
综上所述,颅内孤立性纤维瘤是一种临床罕见的中枢神经系统肿瘤,当瘤内出现“阴阳征”或“黑白征”、T2WI低信号区明显强化及流空血管影等时应考虑诊断ISFT,最终确诊需病理及免疫组织化学检查。
-
![]()
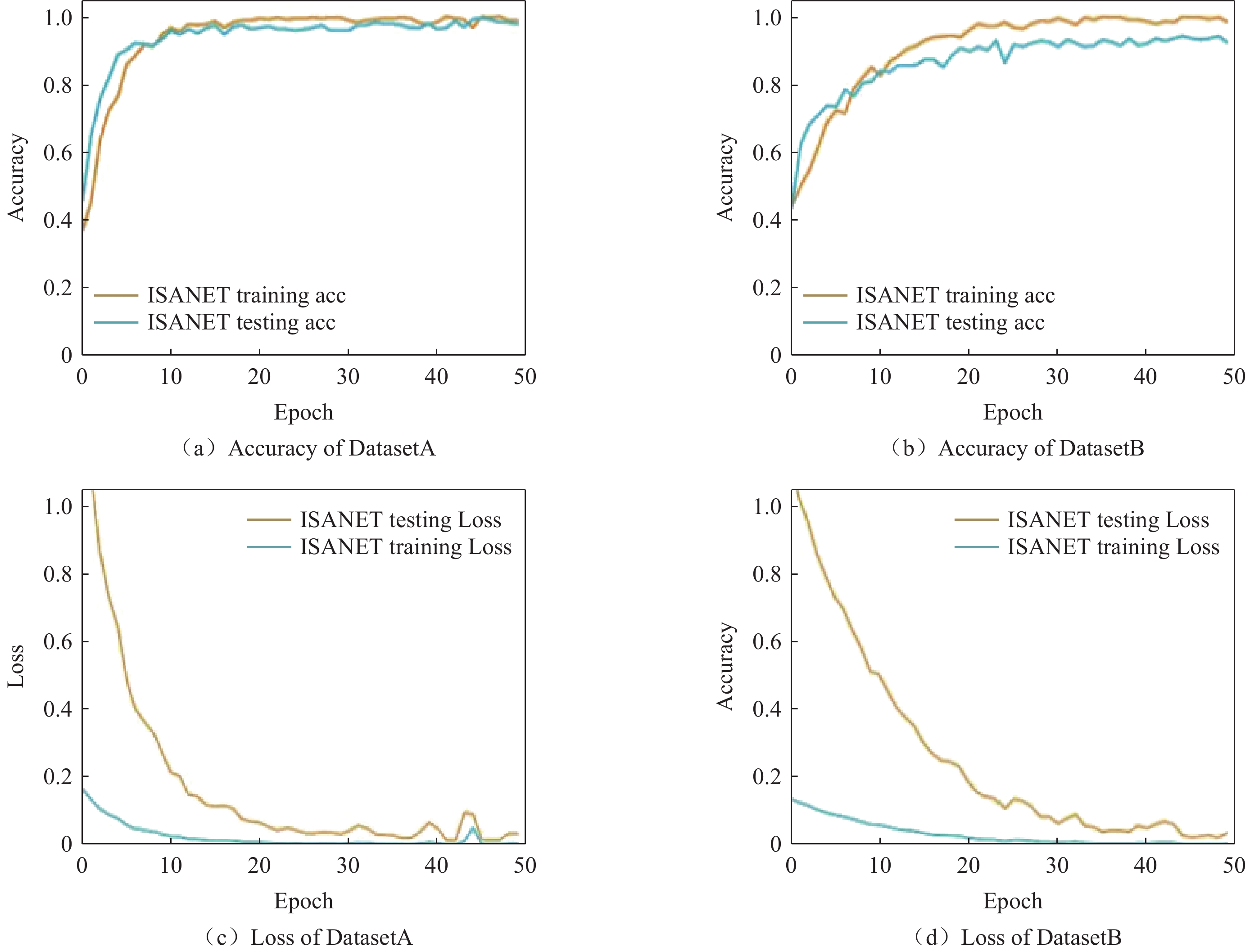
图 5 ISANET模型在不同数据集中的准确率和损失曲线
Figure 5. Accuracy and loss curves of ISANET on different datasets
表 1 不同模型在DatasetA中的查准率、召回率和F1值比较情况
Table 1 Comparison of precision, sensitivity, and F1 score of different models in dataset A
算法名称 腺癌 鳞癌 未见明显异常 查准率 召回率 F1值 查准率 召回率 F1值 查准率 召回率 F1值 ISANET 0.898 0.925 0.906 0.946 0.914 0.928 0.959 0.985 0.968 AlexNet 0.870 0.852 0.854 0.863 0.895 0.872 0.994 0.999 0.996 VGG16 0.798 0.789 0.761 0.764 0.857 0.771 0.995 0.992 0.994 InceptionV3 0.974 0.807 0.873 0.754 0.941 0.824 0.961 0.954 0.951 MobileNetV2 0.640 0.902 0.733 0.933 0.711 0.799 0.959 0.963 0.953 ResNet18 0.919 0.929 0.919 0.927 0.905 0.911 0.960 0.992 0.969  下载: 导出CSV
下载: 导出CSV
表 2 不同模型在DatasetB中的查准率、召回率和F1值比较情况
Table 2 Comparison of precision, sensitivity, and F1 score of different models in dataset B
算法名称 腺癌 鳞癌 未见明显异常 查准率 召回率 F1值 查准率 召回率 F1值 查准率 召回率 F1值 ISANET 0.911 0.824 0.862 0.754 0.882 0.808 0.937 0.942 0.936 AlexNet 0.846 0.740 0.779 0.575 0.816 0.646 0.992 0.895 0.941 VGG16 0.814 0.720 0.717 0.507 0.668 0.531 0.964 0.949 0.952 InceptionV3 0.883 0.835 0.849 0.758 0.824 0.777 0.876 0.938 0.882 MobileNetV2 0.896 0.748 0.805 0.601 0.858 0.670 0.939 0.904 0.910 ResNet18 0.831 0.866 0.842 0.792 0.785 0.788 0.989 0.874 0.926
下载: 导出CSV
表 3 各模型在不同数据集中的准确度
Table 3 Accuracy of each model in different datasets
算法名称 Dataset A Dataset B ISANET 0.996 0.952 AlexNet 0.951 0.854 VGG16 0.939 0.901 InceptionV3 0.980 0.946 MobileNetV2 0.964 0.932 ResNet18 0.992 0.939
下载: 导出CSV
表 4 消融实验结果
Table 4 The results of ablation experiments
组别 Dataset A Dataset B A组 0.806 0.745 B组 0.810 0.735 C组 0.854 0.796 D组 0.802 0.721
下载: 导出CSV
-
[1] HERBST R S, MORGENSZTERN D, BOSHOFF C. The biology and management of non-small cell lung cancer[J]. Nature, 2018, 553(7689): 446-454. DOI: 10.1038/nature25183.
[2] 中华医学会肿瘤学分会, 中华医学会杂志社. 中华医学会肺癌临床诊疗指南(2022版)[J]. 中华肿瘤杂志, 2022, 44(6): 457-490. DOI: 10.3760/cma.j.cn112152-20220413-00255. ONCOLOGY SOCIETY OF CHINESE MEDICAL ASSOCIATION, CHINESE MEDICAL ASSOCIATION PUBLISHING HOUSE. Chinese Medical Association guideline for clinical diagnosis and treatment of lung cancer (2022 edition)[J]. Chinese Journal of Oncology, 2022, 44(6): 457-490. DOI: 10.3760/cma.j.cn112152-20220413-00255.
[3] CARRILLO-PEREZ F, MORALES J C, CASTILLO-SECILLA D, et al. Non-small-cell lung cancer classification via RNA-Seq and histology imaging probability fusion[J]. BMC Bioinformatics, 2021, 22(1): 454. DOI: 10.1186/s12859-021-04376-1.
[4] WOODARD G A, JONES K D, JABLONS D M. Lung cancer staging and prognosis[J]. Cancer Treatment and Research, 2016, 170: 47-75. DOI: 10.1007/978-3-319-40389-2_3.
[5] CAO B, WANG P, GU L, et al. Use of four genes in exosomes as biomarkers for the identification of lung adenocarcinoma and lung squamous cell carcinoma[J]. Oncology Letters, 2021, 21(4): 249. DOI: 10.3892/ol.2021.12510.
[6] KIM T-H, WOO S, YOON S H, et al. CT Characteristics of non–small cell lung cancer with anaplastic lymphoma kinase rearrangement: A systematic review and meta-analysis[J]. American Journal of Roentgenology, 2019, 213(5): 1059-1072. DOI: 10.2214/AJR.19.21485.
[7] 宋若晨, 褚相乐, 黄勇华, 等. 基于颅脑T1WI对比增强图像构建卷积神经网络模型鉴别肺癌与乳腺癌脑转移[J]. 中国医学影像技术, 2023, 39(7): 982-986. SONG R C, CHU X L, HUANG Y H, et al. Convolutional neural network model based on contrast-enhanced cranial T1WI for differentiating brain metastases from lung cancer or breast cancer[J]. Chinese Journal of Medical Imaging Technology, 2023, 39(7): 982-986.
[8] LITJENS G, KOOI T, BEJNORDI B E, et al. A survey on deep learning in medical image analysis[J]. Medical Image Analysis, 2017, 42: 60-88. DOI: 10.1016/j.media.2017.07.005.
[9] YAMASHITA R, NISHIO M, DO R K G, et al. Convolutional neural networks: An overview and application in radiology[J]. Insights into Imaging, 2018, 9(4): 611-629. DOI: 10.1007/s13244-018-0639-9.
[10] RUSSAKOVSKY O, DENG J, SU H, et al. ImageNet large scale visual recognition challenge[J]. International Journal of Computer Vision, 2015, 115(3): 211-252. DOI: 10.1007/s11263-015-0816-y.
[11] SZEGEDY C, VANHOUCKE V, IOFFE S, et al. Rethinking the inception architecture for computer vision[C]//2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Las Vegas, NV, USA: IEEE, 2016: 2818-2826.
[12] COUDRAY N, OCAMPO P S, SAKELLAROPOULOS T, et al. Classification and mutation prediction from non–small cell lung cancer histopathology images using deep learning[J]. Nature Medicine, 2018, 24(10): 1559-1567. DOI: 10.1038/s41591-018-0177-5.
[13] JIANG X, SHEN H. Classification of lung tissue with cystic fibrosis lung disease via deep convolutional neural networks[C]//Proceedings of the 2nd International Symposium on Image Computing and Digital Medicine. Chengdu China: ACM, 2018: 113-116.
[14] MOITRA D, KR. MANDAL R. Classification of non-small cell lung cancer using one-dimensional convolutional neural network[J]. Expert Systems with Applications, 2020, 159: 113564. DOI: 10.1016/j.eswa.2020.113564.
[15] 唐秉航, 王艳芳, 马力, 等. 基于混合注意力机制的肺结节假阳性降低[J]. CT理论与应用研究, 2022, 31(1): 63-72. DOI: 10.15953/j.ctta.2021.002. TANG B H, WANG Y F, MA L, et al. False positive reduction of pulmonary nodules based on mixed attentional raechanism[J]. CT Theory and Applications, 2022, 31(1): 63-72. DOI: 10.15953/j.ctta.2021.002.
[16] TERAMOTO A, TSUKAMOTO T, KIRIYAMA Y, et al. Automated classification of lung cancer types from cytological images using deep convolutional neural networks[J]. BioMed Research International, 2017, 2017: 1-6.
[17] TERAMOTO A, YAMADA A, KIRIYAMA Y, et al. Automated classification of benign and malignant cells from lung cytological images using deep convolutional neural network[J]. Informatics in Medicine Unlocked, 2019, 16: 100205. DOI: 10.1016/j.imu.2019.100205.
[18] 樊雪林, 文昱齐, 乔志伟. 基于Transformer增强型U-net的CT图像稀疏重建与伪影抑制[J]. CT理论与应用研究(中英文), 2024, 33(1): 1-12. DOI: 10.15953/j.ctta.2023.183. FAN X L, WEN Y Q, QIAO Z W. Sparse Reconstruction of Computed Tomography Images with Transformer Enhanced U-net[J]. CT Theory and Applications, 2024, 33(1): 1-12. DOI: 10.15953/j.ctta.2023.183.
[19] KHAN M A, RAJINIKANTH V, SATAPATHY S C, et al. VGG19 network assisted joint segmentation and classification of lung nodules in CT images[J]. Diagnostics, 2021, 11(12): 2208. DOI: 10.3390/diagnostics11122208.
[20] 王媛媛, 周涛, 陆惠玲, 等. 基于集成卷积神经网络的肺部肿瘤计算机辅助诊断模型[J]. 生物医学工程学杂志, 2017, 34(4): 543-551. DOI: 10.7507/1001-5515.201607003. WANG Y Y, ZHOU T, LU H L, et al. Computer aided diagnosis model for lung tumor based on ensemble convolutional neural network[J]. Journal of Biomedical Engineering, 2017, 34(4): 543-551. DOI: 10.7507/1001-5515.201607003.
[21] AKSELROD-BALLIN A, KARLINSKY L, ALPERT S, et al. A Region Based Convolutional Network for Tumor Detection and Classification in Breast Mammography[M]//Carneiro G, Mateus D, Peter L, et al. Deep Learning and Data Labeling for Medical Applications: Vol. 10008. Cham: Springer International Publishing, 2016: 197-205.
[22] HELWAN A, EL-FAKHRI G, SASANI H, et al. Deep networks in identifying CT brain hemorrhage[J]. Journal of Intelligent & Fuzzy Systems, 2018, 35(2): 2215-2228.
[23] ESTEVA A, KUPREL B, NOVOA R A, et al. Dermatologist-level classification of skin cancer with deep neural networks[J]. Nature, 2017, 542(7639): 115-118. DOI: 10.1038/nature21056.
[24] HARANGI B. Skin lesion classification with ensembles of deep convolutional neural networks[J]. Journal of Biomedical Informatics, 2018, 86: 25-32. DOI: 10.1016/j.jbi.2018.08.006.
[25] ALOM M Z, YAKOPCIC C, NASRIN MST S, et al. Breast Cancer Classification from Histopathological Images with Inception Recurrent Residual Convolutional Neural Network[J]. Journal of Digital Imaging, 2019, 32(4): 605-617. DOI: 10.1007/s10278-019-00182-7.
[26] SANDLER M, HOWARD A, ZHU M, et al. MobileNetV2: Inverted residuals and linear bottlenecks[C]//2018 IEEE/CVF Conference on Computer Vision and Pattern Recognition. Salt Lake City, UT: IEEE, 2018: 4510-4520.
[27] SZEGEDY C, LIU W, JIA Y Q, et al. Going deeper with convolutions[C]//2015 IEEE Conference on Computer Vision and Pattern Recognition (CVPR). Boston, MA, USA: IEEE, 2015: 1-9.
[28] IOFFE S, SZEGEDY C. Batch normalization: accelerating deep network training by reducing internal covariate shift[M]. arXiv, 2015. http://arxiv.org/abs/1502.03167, 2015-03-02.
[29] 王坤, 王冠民, 路志凯. 动态增强CT对周围型肺癌的诊断价值[J]. 肿瘤研究与临床, 2021, 33(4): 304-306. DOI: 10.3760/cma.j.cn115355-20201127-00667. [30] 薛彩强, 杜晓灏, 金龙, 等. 基于MRI深度学习模型预测WHOⅡ、Ⅲ级胶质瘤MGMT启动子甲基化状态[J]. 中华放射学杂志, 2021, 55(7): 734-738. XUE C K, DU X H, JIN L, et al. Prediction of methylation status of MGMT promoter in WHO grade Ⅱ, Ⅲ glioma based on MRI deep learning model[J]. Chinese Journal of Radiology, 2021, 55(7): 734-738.
[31] 孟宇, 马之骋, 阮敬儒, 等. 基于Faster R卷积神经网络构建胸部X线片异物智能检测模型的可行性研究[J]. 中华放射学杂志, 2022, 56(12): 1359-1364. MENG Y, MA Z C, RUAN J R, et al. Feasibility of constructing the intelligent detection model for foreign bodies on chest X-ray based on Faster R-convolutionalneural network[J]. Chinese Journal of Radiology, 2022, 56(12): 1359-1364.
-
期刊类型引用(1)
1. 魏昊业,柳青,宗会迁. GE LightSpeed Pro 16 CT伪影故障维修3例. 医疗卫生装备. 2024(10): 118-120 .  百度学术
百度学术
其他类型引用(0)



计量
- 文章访问数: 88
- HTML全文浏览量: 9
- PDF下载量: 19
- 被引次数: 1


