
Evaluation of CT in Predicting Central Lymph Node Metastasis of Papillary Thyroid Microcarcinoma
-
摘要: 目的:明确CT在预测甲状腺微小乳头状癌(PTMC)中央区淋巴结转移(CLNM)中的价值。方法:选取成都市第三人民医院157例经病理证实的PTMC患者,回顾分析患者的CT及临床病理资料,受试者工作特征曲线(ROC曲线)得出PTMC长径预测CLNM的最佳截断值,通过CT及临床病理资料建立PTMC CLNM的二元logistic回归模型,并通过ROC曲线评价模型的诊断价值。结果:ROC曲线得出预测PTMC CLNM的最佳截断值为6 mm;单因素分析:咬饼征、微钙化、多灶癌、PTMC长径≥6 mm、男性、年龄<45岁是PTMC CLNM的危险因素;二元Logistic回归分析:咬饼征伴突出(OR=5.159,95% CI=1.137~23.400)、多灶癌(OR=2.734,95% CI=1.215~6.154)、PTMC长径≥6 mm(OR=3.259,95% CI=1.326~8.008)、男性(OR=3.776,95% CI=1.339~10.653)、年龄<45岁(OR=3.222,95% CI=1.419~7.777)是PTMC CLNM的独立危险因素;ROC曲线得出,约登指数=0.502时,诊断CLNM的敏感性、特异性分别为82.5%和68.0%。结论:二元Logistic回归模型有助于预测PTMC CLNM;咬饼征伴突出、PTMC≥6 mm、男性、年龄<45岁是PTMC CLNM的独立危险因素。对于上述类型患者,外科医师可考虑中央区淋巴结清扫。
-
关键词:
- 计算机体层成像 /
- 甲状腺微小乳头状癌 /
- Logistic回归分析
Abstract: Objective: To determine the value of CT in predicting CLNM in PTMC. Methods: 157 patients with PTMC confirmed by pathology in our hospital were enrolled, and the CT and clinicopathological data of the patients were retrospectively analyzed. ROC curve was used to determine the optimal cutoff value of PTMC greatest diameter for CLNM. The binary logistic regression model of PTMC CLNM was established based on CT and clinical pathological data, and the diagnostic value of the model was evaluated by ROC curve. Results: According to the ROC curve, the optimal cutoff value for predicting PTMC CLNM was 6 mm. Univariate analysis: Cookie bite sign , microcalcification, multifocality, PTMC greastest diameter ≥6 mm, male, Age<45 were risk factors for PTMC CLNM. Binary Logistic regression analysis: Cookie bite sign with protruding (OR=5.159, 95% CI=1.137 ~ 23.400), multifocality (OR=2.734, 95% CI=1.215 ~ 6.154), PTMC greastest diameter ≥6 mm (OR=3.259, 95% CI=1.326 ~ 8.008), male (OR=3.776, 95% CI=1.339 ~ 10.653), age <45 (OR=3.222, 95% CI=1.419 ~ 7.777), were independent risk factors for PTMC CLNM. According to the ROC curve, when the Youden index=0.502, the sensitivity and specificity in predicting CLNM were 82.5% and 68.0%, respectively. Conclusion: The binary logistic regression model is helpful in predicting PTMC CLNM. Cookie bite sign with protruding, PTMC greastest diameter≥6 mm, male, and age<45 were independent risk factors for PTMC CLNM. For this type of patients, we suggest that surgeons should consider central lymph node dissection. -
-
![]()
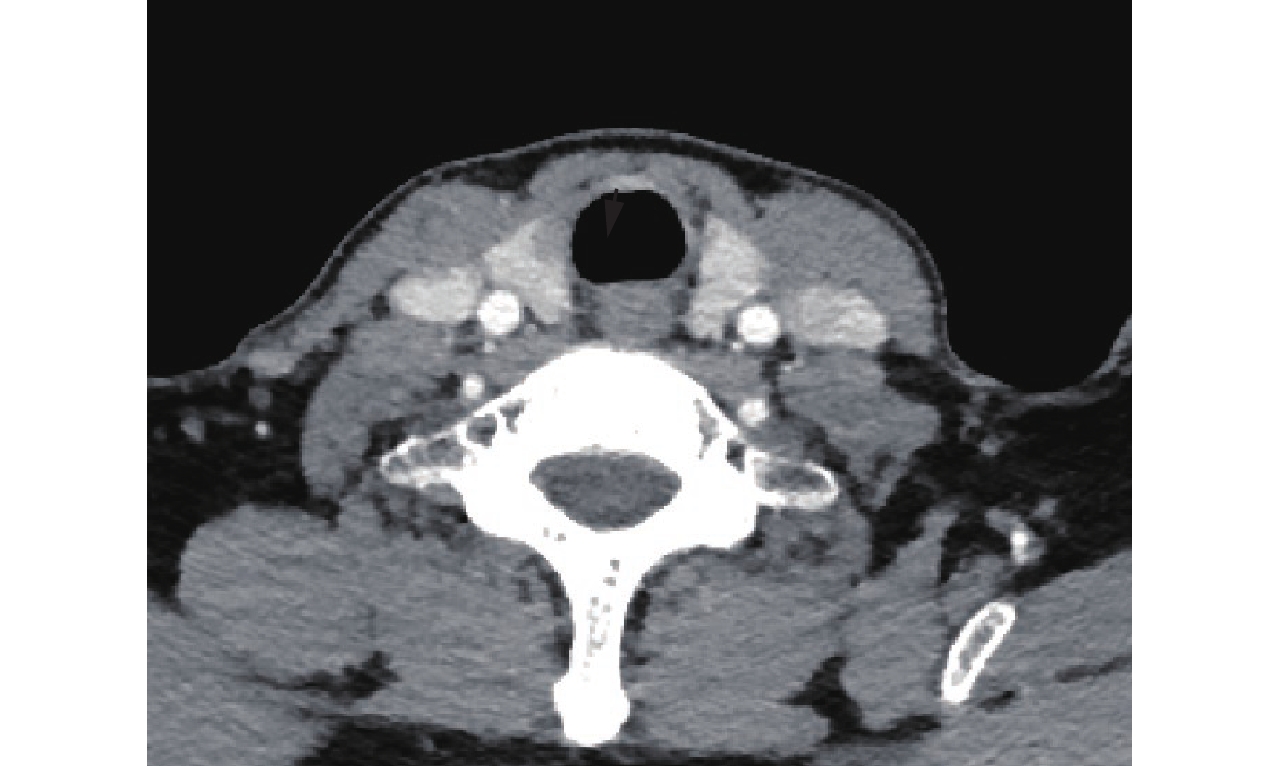
图 1 53岁女性,甲状腺右侧叶结节无咬饼征(黑箭头),病理结果:PTMC不伴CLNM
Figure 1. Female, 53 years old,the nodule in the right thyroidal lobe without cookie bite sign (black arrow). Pathological results: PTMC without CLNM
![]()
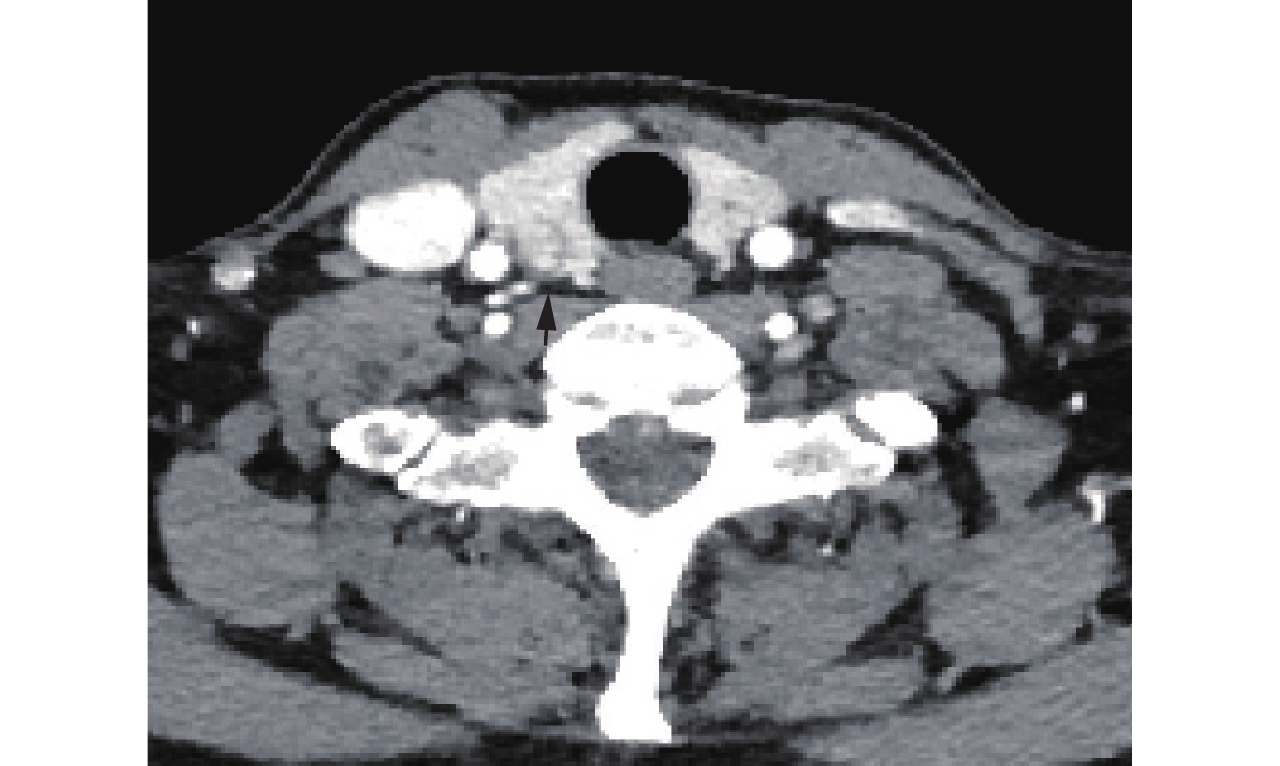
图 2 45岁女性,甲状腺右侧叶结节咬饼征不伴突出(黑箭头),病理结果提示PTMC不伴CLNM
Figure 2. Female, 45 years old, the nodule in the right thyroidal lobe with cookie bite sign without protruding (black arrow). Pathological results: PTMC without CLNM
![]()
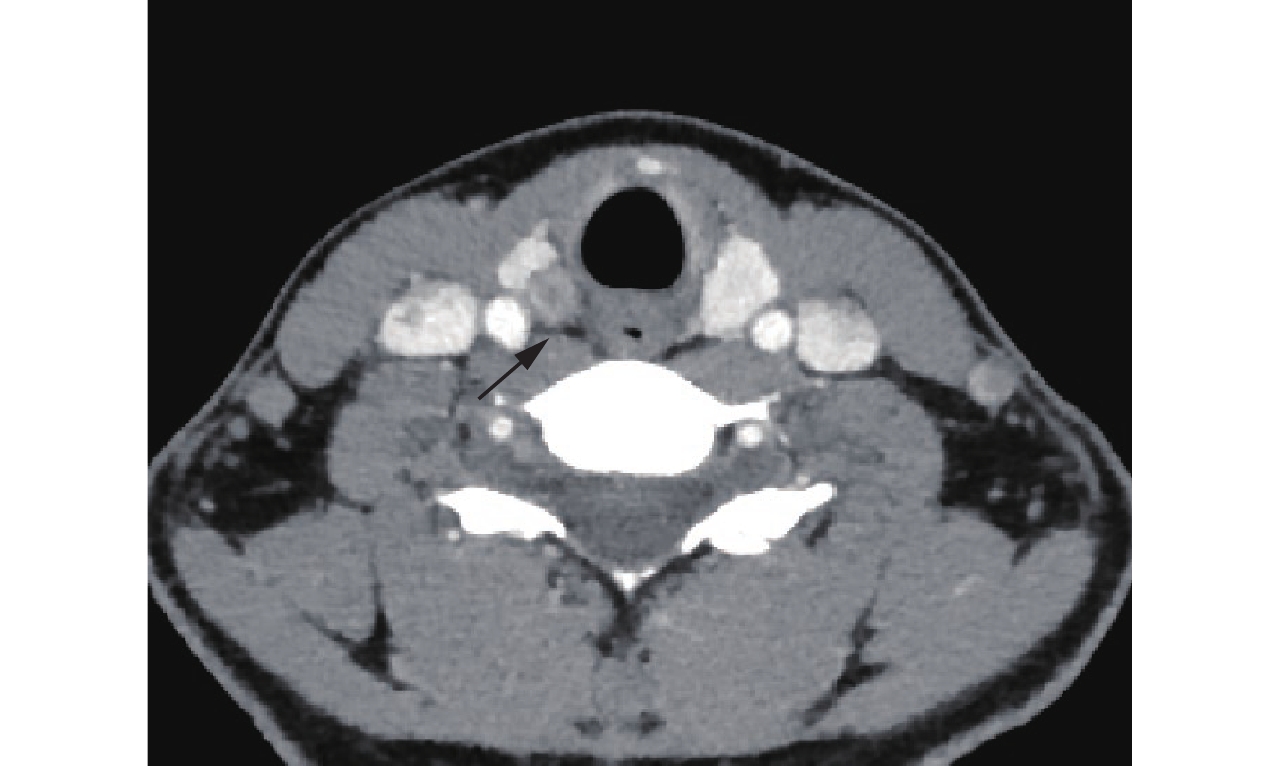
图 3 52岁男性,甲状腺右侧叶结节咬饼征伴突出(黑箭头),病理结果提示PTMC伴CLNM
Figure 3. Male, 53 years old, the nodule in the right thyroidal lobe with cookie bite sign with protruding (black arrow). Pathological results: PTMC CLNM
![]()
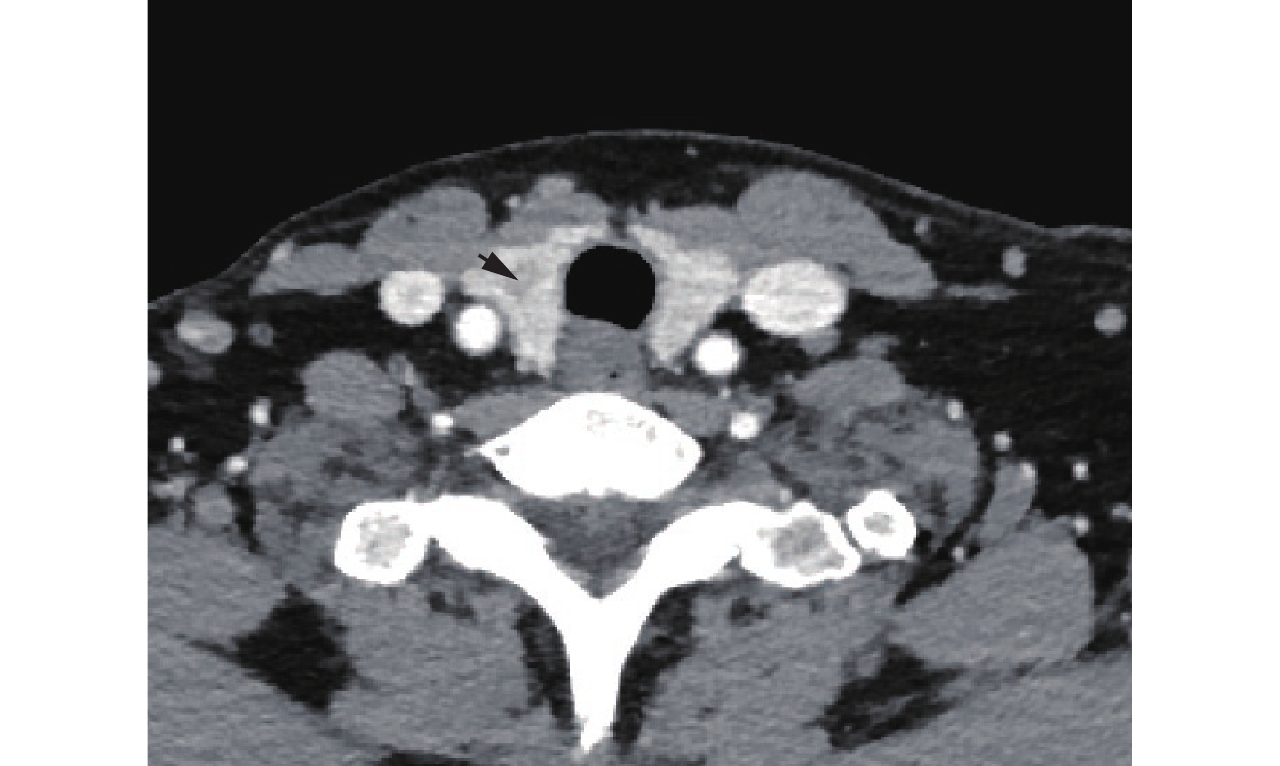
图 4 34岁女性,甲状腺右侧叶结节咬饼征伴突出(黑箭头),病理结果提示PTMC伴CLNM
Figure 4. Female, 34 years old, the nodule in the right thyroidal lobe with cookie bite sign with protruding (black arrow). Pathological results: PTMC CLNM
表 1 PTMC CLNM的单因素分析结果
Table 1 The result of Univariate analysis in PTMC CLNM
项目 特征 CLNM 统计检验 是 否 χ2 P 咬饼征 咬饼征伴突出 32 28 14.119 0.001 咬饼征不伴突出 21 49 无咬饼征 4 23 增强后边界模糊 是 43 79 0.266 0.606 否 14 21 微钙化 是 24 21 7.909 0.006 否 33 79 多灶癌 是 34 27 16.290 <0.001 否 23 73 长径≥6 mm 是 47 45 20.995 <0.001 否 10 55 PTMC位置 甲状腺上叶 28 51 0.175 0.916 甲状腺下叶 24 42 甲状腺峡部 5 7 性别 男 18 17 4.455 0.046 女 39 83 年龄<45岁 是 44 48 12.754 <0.001 否 13 52  下载: 导出CSV
下载: 导出CSV
表 2 PTMC CLNM的二元Logistic回归分析结果
Table 2 The result of binary Logistic regression analysis in PTMC CLNM
项目 β P OR OR 95% CI 下限 上限 微钙化 0.669 0.122 1.952 0.836 4.554 多灶癌 1.006 0.015 2.734 1.215 6.154 长径≥6 mm 1.181 0.010 3.259 1.326 8.008 男性 1.329 0.012 3.776 1.339 10.653 年龄<45岁 1.201 0.006 3.322 1.419 7.777 咬饼征不伴突出 0.920 0.207 2.510 0.602 10.468 咬饼征伴突出 1.641 0.033 5.159 1.137 23.400 常数 -4.176 <0.000 0.015 — —
下载: 导出CSV
-
[1] MOLINARO E, CAMPOPIANO M C, ELISEI R. Management of endocrine disease: Papillary thyroid microcarcinoma: Toward an active surveillance strategy[J]. European Journal of Endocrinology, 2021, 185(1): R23−r34. DOI: 10.1530/eje-21-0256.
[2] HAUGEN B R, ALEXANDER E K, BIBLE K C, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer the american thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer[J]. Thyroid, 2016, 26(1): 1−133. DOI: 10.1089/thy.2015.0020.
[3] FENG J W, PAN H, WANG L, et al. Determine the optimal extent of thyroidectomy and lymphadenectomy for patients with papillary thyroid microcarcinoma[J]. Frontiers in Endocrinology, 2019, 10: 363. DOI: 10.3389/fendo.2019.00363.
[4] 张伽铭, 韩志江. 甲状腺微小乳头状癌多种CT征象的多因素分析[J]. 国际医学放射学杂志, 2017,40(1): 6−9. doi: 10.19300/j.2017.L4245 ZHANG J M, HAN Z J. Multivariate analysis of various CT signs of papillary thyroid microcarcinoma[J]. International Journal of Medical Radiology, 2017, 40(1): 6−9. (in Chinese). doi: 10.19300/j.2017.L4245
[5] 史学伟, 唐笑先, 赵杰, 等. 甲状腺乳头状癌CT特征与中央组淋巴结转移的相关性[J]. 实用放射学杂志, 2021,37(3): 373−376. doi: 10.3969/j.issn.1002-1671.2021.03.008 SHI X W, TANG X X, ZHAO J, et al. Research on the relationship between papillary thyroid carcinoma's CT features and central lymph node metastasis[J]. Journal of Practical Radiology, 2021, 37(3): 373−376. (in Chinese). doi: 10.3969/j.issn.1002-1671.2021.03.008
[6] ZHENG X, PENG C, GAO M, et al. Risk factors for cervical lymph node metastasis in papillary thyroid microcarcinoma: A study of 1587 patients[J]. Cancer Biology Medicine, 2019, 16(1): 121−130. DOI: 10.20892/j.issn.2095-3941.2018.0125.
[7] KIM S K, PARK I, WOO J W, et al. Predictive factors for lymph node metastasis in papillary thyroid microcarcinoma[J]. Annals of Surgical Oncology, 2016, 23(9): 2866−2873. DOI: 10.1245/s10434-016-5225-0.
[8] SIDDIQUI S, WHITE M G, ANTIC T, et al. Clinical and pathologic predictors of lymph node metastasis and recurrence in papillary thyroid microcarcinoma[J]. Thyroid, 2016, 26(6): 807−815. DOI: 10.1089/thy.2015.0429.
[9] SUN J, JIANG Q, WANG X, et al. Nomogram for preoperative estimation of cervical lymph node metastasis risk in papillary thyroid microcarcinoma[J]. Frontiers in Endocrinology, 2021, 12: 613974. DOI: 10.3389/fendo.2021.613974.
[10] LI J, LIU J, QIAN L. Suspicious ultrasound characteristics correlate with multiple factors that predict central lymph node metastasis of papillary thyroid carcinoma: Significant role of HBME-1[J]. European Journal of Radiology, 2020: 123. DOI: 10.1016/j.ejrad.2019.108801.
[11] 周瑾, 周世崇, 李佳伟, 等. 单灶性甲状腺乳头状癌中央区淋巴结转移危险因素分析[J]. 中华超声影像学杂志, 2019,28(3): 235−240. DOI: 10.3760/cma.j.issn.1004-4477.2019.03.009. ZHOU J, ZHOU S C, LI J W, et al. Risk factors of central neck lymph node metastasis following solitary papillary thyroid carcinoma[J]. Chinese Journal of Ultrasonography, 2019, 28(3): 235−240. DOI: 10.3760/cma.j.issn.1004-4477.2019.03.009. (in Chinese).
[12] 孙可敏, 何秀丽, 郭玲玲. 甲状腺微小乳头状癌临床及超声特征与中央区淋巴结转移的危险因素[J]. 临床耳鼻咽喉头颈外科杂志, 2021,35(3): 260−263. DOI: 10.13201/j.issn.2096-7993.2021.03.015. SUN K M, HE X L, GUO L L. Clinical and ultrasonic features of papillary thyroid microcarcinoma and risk factors for central lymph node metastasis[J]. Journal of Clinical Otorhinolaryngology Head and Neck Surgery, 2021, 35(3): 260−263. DOI: 10.13201/j.issn.2096-7993.2021.03.015. (in Chinese).
[13] 胡磊, 余盛敬, 王才善, 等. 多因素Logistic分析单灶甲状腺微小乳头状癌中央区淋巴结转移的危险因素[J]. 川北医学院学报, 2020,35(3): 453−457. DOI: 10.3969/j.issn.1005-3697.2020.03.025. HU L, YU S J, WANG C S, et al. Multivariate logistic analysis of risk factors analysis of lymph node metas-tasis in central region of single-foci thyroid micropapillary carcinoma[J]. Journal of North Sichuan Medical College, 2020, 35(3): 453−457. DOI: 10.3969/j.issn.1005-3697.2020.03.025. (in Chinese).
[14] ZHANG T T, QI X Z, CHEN J P, et al. The association between tumor's location and cervical lymph nodes metastasis in papillary thyroid cancer[J]. Gland Surgery, 2019, 8(5): 557−568. DOI: 10.21037/gs.2019.10.02.
计量
- 文章访问数:
- HTML全文浏览量:
- PDF下载量:


