
Study on Multi-slice Spiral CT Enhanced Scanning of Accessory Middle Colonic Artery in Normal Population
-
摘要: 目的:观察分析正常人群中副中结肠动脉(AMCA)的发生率及分布规律。方法:采用回顾性研究方法,收集2021年1月至6月在上海瑞金医院北部院区同时进行上下腹增强CT检查的正常人群331例,发现存在AMCA者97例。将检查的静脉期原始图像进行多平面重建,记录AMCA起源、伴行静脉及与胰腺毗邻关系,并测量AMCA起始点直径,与胰腺最近点的距离。结果:AMCA发生率为29.3%(97/331),66.0% 起源于肠系膜上动脉(64/97)、17.5%起源于肠系膜下动脉(17/97)、16.5% 起源于胰十二指肠下动脉(16/97)。AMCA直径为(2.0±0.24) mm,距离胰腺最近点为(2.1±1.4) mm。AMCA均可见伴行静脉,72.2% AMCA的伴行静脉汇入肠系膜下静脉(70/97),20.6% 汇入肠系膜上静脉(20/97),6.2% 汇入脾静脉(6/97),1% 汇入空肠静脉(1/97)。结论:多层螺旋CT增强扫描能清晰显示AMCA起源、伴行静脉与胰腺毗邻关系,能为临床术前提供准确的血管评估。
-
关键词:
- 多层螺旋CT增强扫描 /
- 血管解剖 /
- 副中结肠动脉
Abstract: Objective: To evaluate the incidence and patterns of AMCA amony normal population. Methods: 331 cases of normal people who underwent Abdomen & Pelvis enhanced CT scan in RuiJin Hospital North Area from January, 2021 to June, 2021 were retrospectively collected for the present study and 97 cases were found to have got AMCA. Multiplanar reconstruction was performed on the original images of venous phase to record how the AMCA originated and the adjacency relationship between the accompanying veins and pancreas. The diameter of AMCA starting point and the distance to the nearest point of pancreas were also measured. Results: The incidence of AMCA was 29.3% (97/331). Among the 97 cases, 66.0% (64/97) occurred in superior mesenteric artery, 17.5% (17/97) occurred in inferior mesenteric artery and 6.5%(16/97) occurred in inferior pancreaticoduodenal artery. The average diameter of AMCA was (2.0±0.24)mm, the minimum distance to pancreas was (2.1±1.4)mm. Accompanying vein was observed in all the 97 AMCA cases, 72.2% (70/97) converged towards inferior mesenteric vein, 20.6% (20/97) converged towards superior mesenteric vein, 6.2% (6/97) converged towards splenic vein, and 1% (1/97) converged towards jejunal vein. Conclusion: Multi-slice spiral CT contrast enhancement scan can clearly show the origin and the adjacency relationship between the accompanying veins and pancreas of ACMA. It can provide accurate evaluation of blood vessels before operation. -
-
![]()
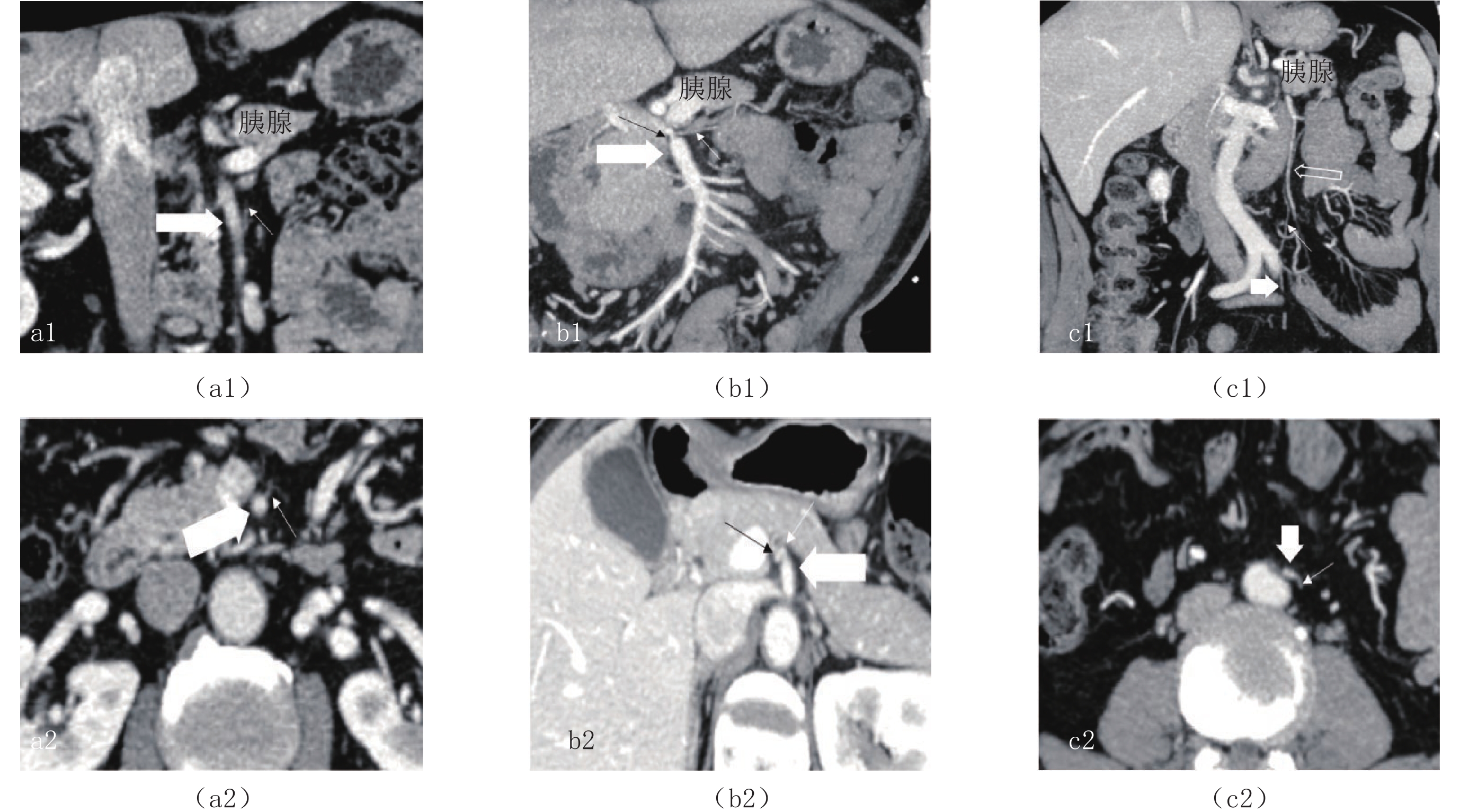
图 2 AMCA起源
(a1)、(a2)同一病例的冠状面重建、横断面图像,(b1)、(b2)同一病例的斜冠状面MIP重建、斜横断面图像;(c1)、(c2)同一病例的斜冠状面MIP重建、横断面图像;(a)~(c)为不同病例。图中白色细箭头AMCA,白色粗长箭头SMA,黑色箭头IPDA,白色粗短箭头 IMA,白色空心箭头IMV。
Figure 2. Origin of AMCA
![]()
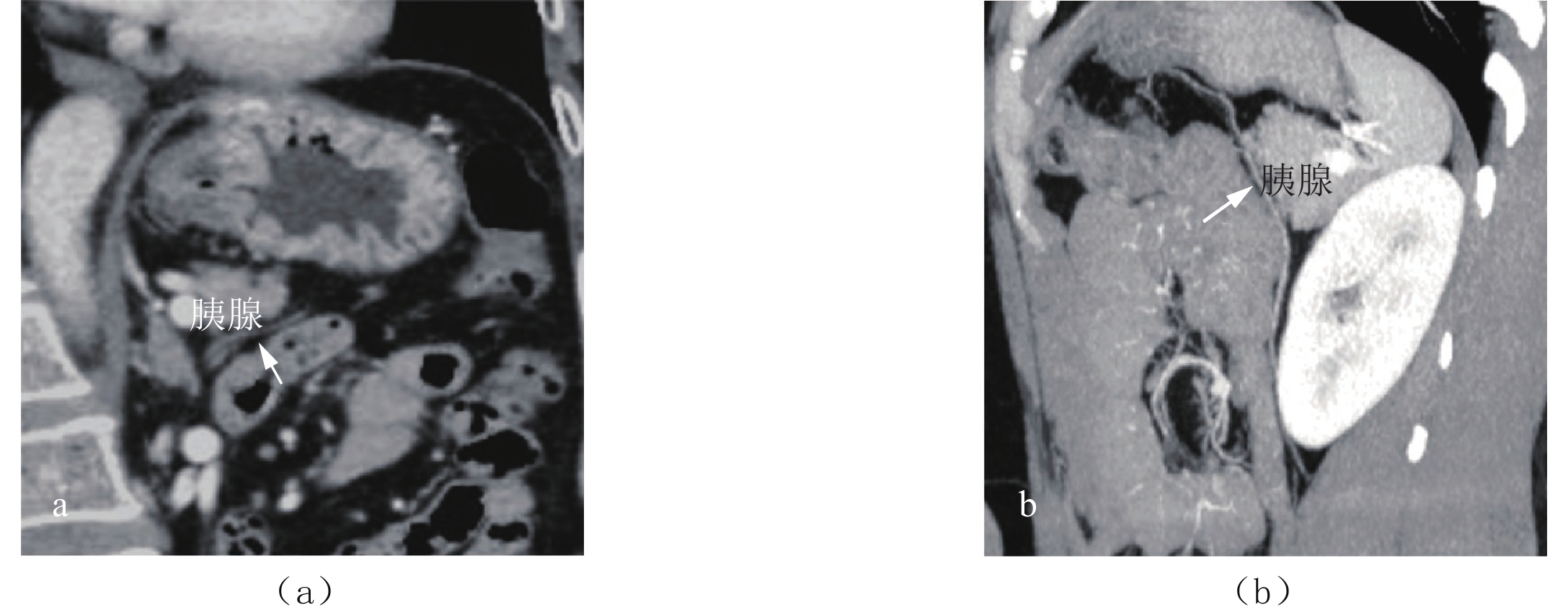
图 3 AMCA与胰腺毗邻关系
(a)斜冠状面重建图像:SMA来源的AMCA沿胰腺下方走行,由胰腺后方/下方走向胰腺前方;(b)斜矢状面MIP重建图像:IMA来源的AMCA斜行于胰腺前方、经过胰腺。图中白色箭头AMCA。
Figure 3. The adjacency relationship between the accompanying veins and pancreas
![]()
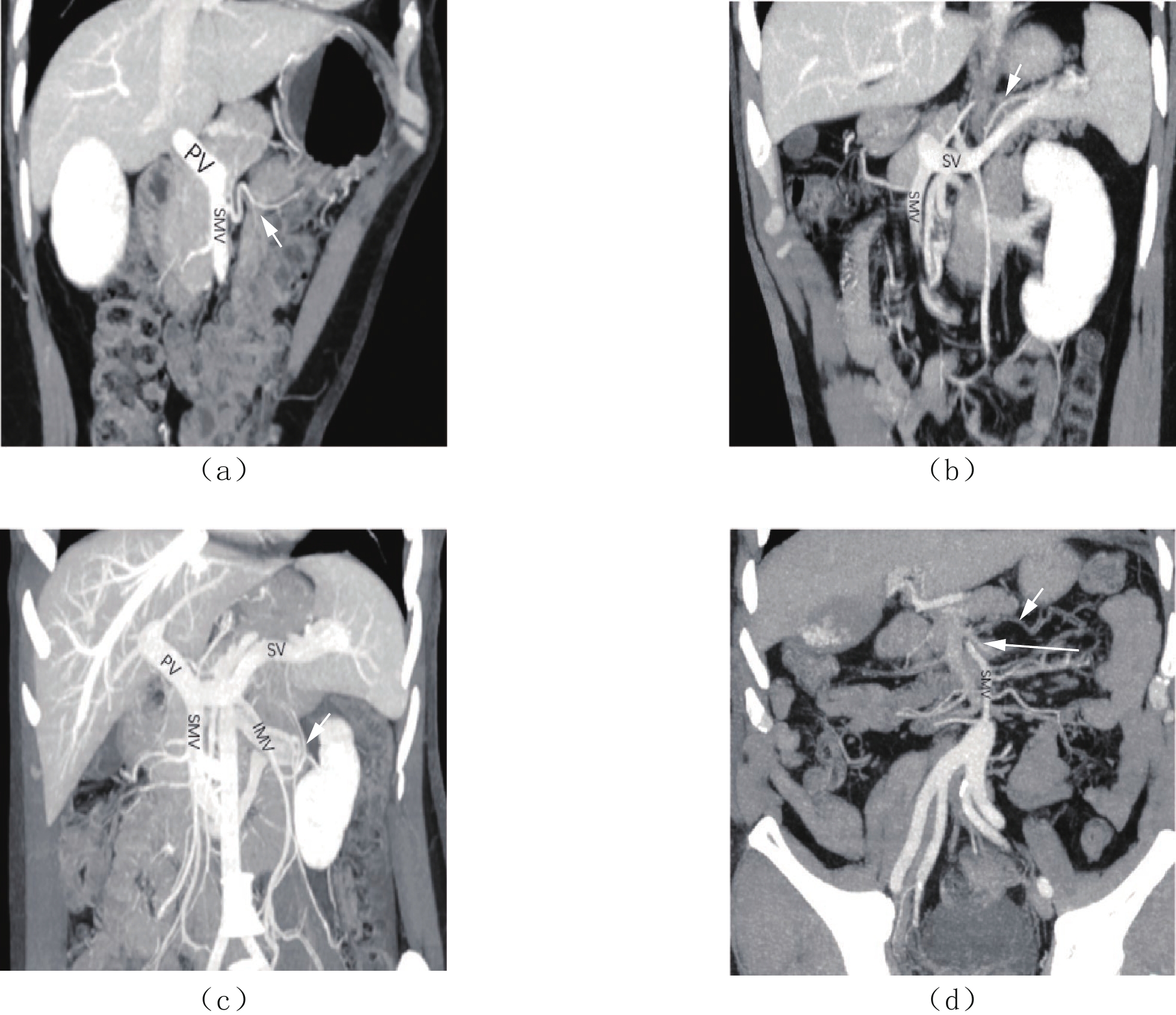
图 4 斜冠状面MIP重建图像:AMCA伴行静脉回流途径
(a)伴行静脉汇入SMV;(b)伴行静脉汇入SV;(c)伴行静脉汇入IMV;(d)伴行静脉汇入空肠静脉。图中白色短箭头为AMCA伴行静脉;白色长箭头为空肠静脉。
Figure 4. Oblique coronal MIP reconstruction image: Return path of AMCA accompanying vein
表 1 AMCA各年龄段分布情况(例)
Table 1 AMCA distribution data among different age groups
性别 人数 AMCA起源 SMA IPDA IMA 男性 50(165) 20~29岁 2(9) 0 1 1 30~39岁 5(19) 2 2 1 40~49岁 6(24) 5 0 1 50~59岁 6(35) 5 0 1 60~69岁 18(37) 12 3 3 70~79岁 11(33) 6 1 4 80~89岁 2(8) 2 0 0 女性 47(166) 20~29岁 2(6) 1 1 0 30~39岁 5(19) 3 1 1 40~49岁 2(17) 2 0 0 50~59岁 11(34) 8 2 1 60~69岁 15(56) 10 3 2 70~79岁 12(29) 8 2 2 80~89岁 0(5) 0 0 0  下载: 导出CSV
下载: 导出CSV
表 2 AMCA伴行静脉回流方向
Table 2 Return direction of AMCA accompanying veins
分布情况 男性/50(97) 女性/47(97) 分布情况 男性/50(97) 女性/47(97) AMCA起源于SMA 32 31 伴行静脉汇入IMV 9 5 伴行静脉汇入SMV 5 6 伴行静脉汇入SV 1 0 伴行静脉汇入IMV 24 23 AMCA起源于IPDA 7 9 伴行静脉汇入SV 2 2 伴行静脉汇入SMV 2 4 伴行静脉汇入空肠静脉 1 0 伴行静脉汇入IMV 5 4 AMCA起源于IMA 11 7 伴行静脉汇入SV 0 1 伴行静脉汇入SMV 1 2
下载: 导出CSV
-
[1] SONNELAND J, ANSON B J, BEATON L E. Surgical anatomy of the arterial supply to the colon from the superior mesenteric artery based upon a study of 600 specimens[J]. Surgery Gynecology & Obstetrics, 1958, 106: 385−98.
[2] WALKER T G. Mesenteric vasculature and collateral pathways[J]. Seminars in Interventional Radiology, 2009, 26(3): 167−174.
[3] STEFFEN C, BOKEY E L, CHAPUIS P H. Carcinoma of the splenic flexure[J]. Colorectal Disease Rectum, 1987, 30(11): 872−874. DOI: 10.1007/BF02555427.
[4] MURONO K, NOZAWA H, KAWAI K, et al. Vascular anatomy of the splenic flexure: A review of the literature[J]. Surgery Today, 2021. DOI: 10.1007/s00595-021-02328-z.
[5] MIYAKE H, MURONO K, KAWAI K, et al. Evaluation of the vascular anatomy of the left-sided colon focused on the accessory middle colic artery: A single-centre study of 734 patients[J]. Colorectal Disease, 2018, 20(11): 1041−1046. DOI: 10.1111/codi.14287.
[6] FUKUOKA A, SASAKI T, TSUKIKAWA S, et al. Evaluating distribution of the left branch of the middle colic artery and the left colic artery by CT angiography and colonography to classify blood supply to the splenic flexure[J]. Asian Journal of Endoscopic Surgery, 2017, 10: 148−153. doi: 10.1111/ases.12349
[7] ITO K, TAKEMURA N, INAGAKI F, et al. Arterial blood supply to the pancreas from accessary middle colic artery[J]. Pancreatology, 2019, 19(5): 781-785. DOI: 10.1016/j.pan.2019.05.458. PMID: 31164320.
[8] MURONO K, MIYAKE H, HOJO D, et al. Vascular anatomy of the splenic flexure, focusing on the accessory middle colic artery and vein[J]. Colorectal Disease, 2020, 22(4): 392−398. DOI: 10.1111/codi.14886.
[9] YANO M, OKAZAKI S, KAWAMURA I, et al. A three-dimensional computed tomography angiography study of the anatomy of the accessory middle colic artery and implications for colorectal cancer surgery[J]. Surgical and Radiologic Anatomy, 2020, 42(12): 1509−1515. DOI: 10.1007/s00276-020-02511-w.
[10] STEWARD J A, RANKIN F W. Blood supply of the large intestine: Its surgical considerations[J]. Archives Surgery, 1933, 26: 843−891. doi: 10.1001/archsurg.1933.01170050113008
[11] 伍德喜, 彭晓春, 易冰倩, 等. 中结肠动脉3条及右侧卵巢静脉变异1例[J]. 中国临床解剖学杂志, 2017,35(2): 239. WU D X, PENG X C, YI B Q, et al. Three middle colic arteries and the right ovarian vein variation: A case report[J]. Chinese Journal of Clinical Anatomy, 2017, 35(2): 239. (in Chinese).
[12] ALDRIDGE M C, FRANCIS N D, GLAZER G, et al. Colonic complications of severe acute pancreatitis[J]. British Journal of Surgery, 1989, 76(4): 362−367. DOI: 10.1002/bjs.1800760416.
[13] MOGHADAMYEGHANEH Z, MASOMI H, MillS S D, et al. Outcomes of conversion of laparoscopic colorectal surgery to open surgery[J]. Journal of the Society of Laparoscopic & Robotic Surgeons, 2014, 18(4): e2014.00230.
-
期刊类型引用(1)
1. 罗建华,朱侣明,陈圣文,邱秦文,谢鑫,杨娇君. CT常规扫描与CT小肠造影对小肠肿瘤的诊断价值比较. 中国当代医药. 2024(09): 36-39 .  百度学术
百度学术
其他类型引用(0)
计量
- 文章访问数: 279
- HTML全文浏览量: 231
- PDF下载量: 14
- 被引次数: 1


