
CT Manifestations of Pulmonary Infarction Secondary to Acute Pulmonary Embolism
-
摘要: 目的:探讨急性肺动脉栓塞(APE)继发肺梗死(PI)CT特征。方法:回顾性分析41例APE继发PI患者的临床及CT资料,总结PI的数量、位置、形态、边缘、胸腔积液及其动态变化特征。结果:PI的CT特征:①数量及位置:共79个PI病灶,18例患者为单发PI,23例患者为多发;所有PI病灶均位于胸膜下,与胸膜呈宽基底相连;46.8%(37/79)位于右肺下叶,36.7%(29/79)位于左肺下叶,右肺上叶、中叶分别为3.8%(3/79)、6.3%(5/79),左肺上叶舌段6.3%(5/79)。②形态:45.6%(36/79)病灶表现为反晕征(RHS),36.7%(29/79)为椭圆形、楔形及驼峰样实变,17.7%(14/79)为斑片状磨玻璃影。③支气管血管束包埋征:79.7%(63/79)病变内可见支气管血管束走行其中,21.3%(16/79)病变范围较小,其内未见明确支气管血管束走行、包埋。④增强后,79个PI病灶均未见强化。⑤治疗后期,所有PI病灶均演变为斑片或索条影。⑥胸腔积液:63.4%(26/41)患者出现胸腔积液,42.3%(11/26)为双侧胸腔积液,57.7%(15/26)单侧胸腔积液。结论:APE继发PI的CT表现具有一定特征性,胸膜下出现单发或多发病变,有反晕征、楔形或驼峰样实变、支气管血管束包埋特征时应考虑到PI,另外胸腔积液有助于诊断。Abstract: Objective: To investigate the CT findings of pulmonary infarction (PI) secondary to acute pulmonary embolism (APE). Method: The clinical and CT data of 41 patients with PI secondary to APE were analyzed retrospectively. The number, location, shape, margin of PI, pleural effusion and dynamic changes were summarized. Results: CT features of PI: (1) Number and location: Among the total 79 PI lesions, 18 patients had single lesion and 23 patients had multiple lesions. All lesions were located under the pleura and connected to the pleura with a broad base, 46.8% (37/79) were located in the lower lobe of the right lung, 36.7% (29/79) in the lower lobe of the left lung, 3.8% (3/79) in the upper lobe, 6.3% (5/79) in the middle lobe of the right lung, and 6.3% (5/79) in the lingual segment of the upper lobe of the left lung. (2) Shape: 45.6% (36/79) of the lesions showed Reversed Halo Sign (RHS), 36.7% (29/79) displayed consolidation of oval, wedge or hump, 17.7% (14/79) revealed ground glass opacity. (3) Bronchovascular bundles in PI: Bronchovascular bundles were found in 79.7% (63/79) of PI. In 21.3% (16/79) of the cases, there was no bronchovascular bundle in the lesion because of its small size; (4) After enhancement, there was no enhancement shown in the 79 PI lesions. (5) All 79 lesions changed into patchy or linear during the end of the treatment period. (6) Pleural effusion: 63.4% (26/41) of patients had pleural effusion, among whom 42.3% (11/26) had bilateral pleural effusion, and 57.7% (15/26) had unilateral pleural effusion. Conclusion: The imaging manifeatations of PE secondary to API hole certain characteristics. For single or multiple lesions under the pleura, with RHS, consolidation of wedge or hump, bronchovascular bundles, APE secondary to API should be considered. In addition, pleural effusion is helpful for diagnosis.
-
-
![]()
图 1 女,70岁,胸痛,APE继发PI
(a)左肺下叶肺梗死,呈“反晕征”改变,内部为网格样磨玻璃密度影,周边为较薄的实性环,左侧胸腔少量积液;(b)CTPA示左下肺动脉及分支内大量栓子形成(红箭)及相应部位肺梗死(黄箭,与(a)箭头所示为同一病灶),左侧肋膈角少量胸腔积液;(c)治疗1个月后复查,反晕征演变为斑片实变影,胸腔积液消失。
Figure 1. A 70-year-old femal with chest pain and pulmonary infarction secondary to acute pulmonary embolism
![]()
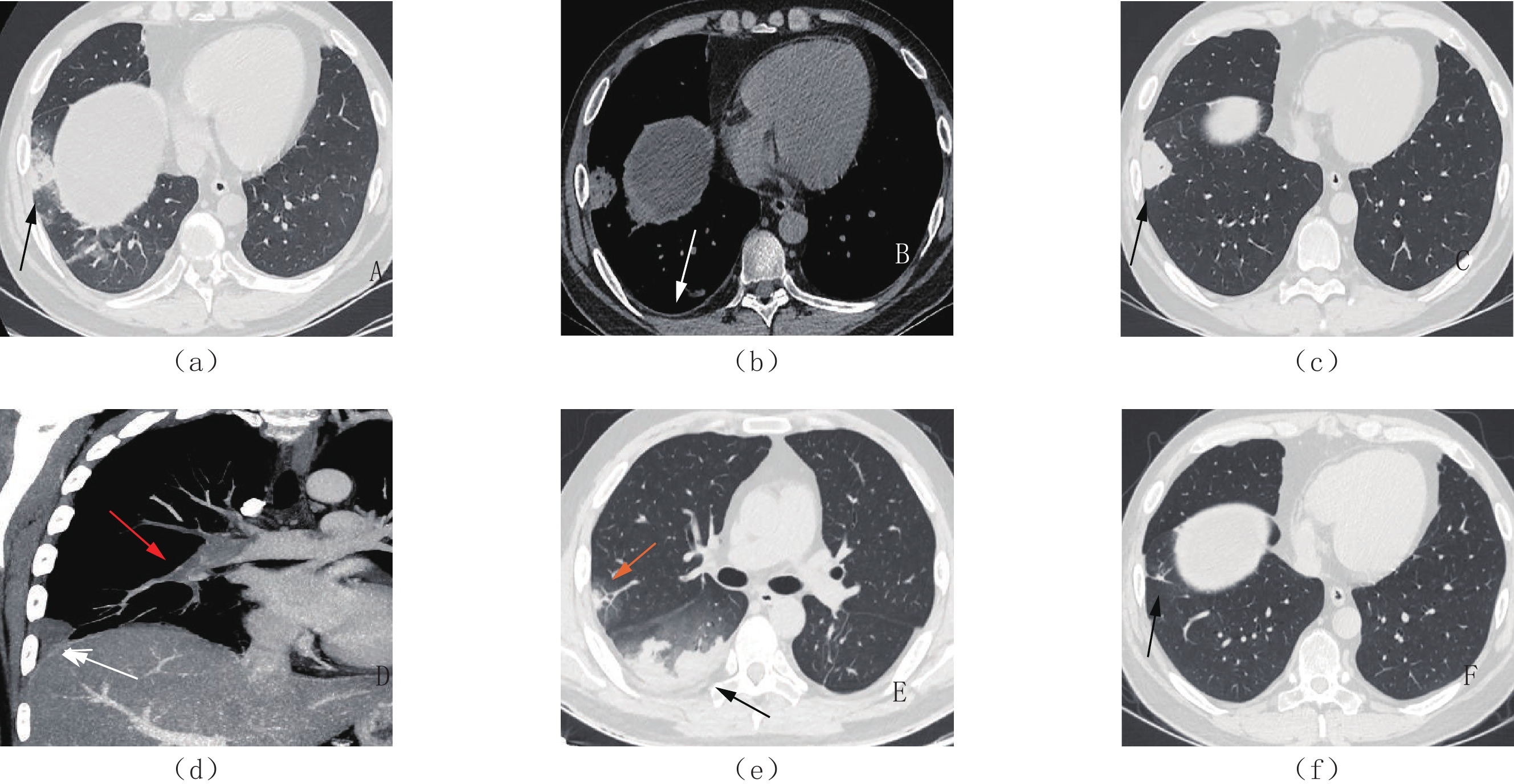
图 2 27岁,男,发热、腹痛,APE继发PI
(a)右肺下叶楔形肺梗死(箭头),内部密度不均,局部呈磨玻璃样改变,误诊为肺炎;(b)纵隔窗:肺梗死内散在小泡状气体密度影,为肺泡腔内残存气体,右侧胸腔少量积液(白箭);(c)抗炎治疗13天后,右肺下叶前基底段病灶变实,边界锐利清晰(箭头);(d)CTPA示右下肺动脉内栓子形成(红箭)及相应部位的楔形肺梗死(白箭);(e)抗凝溶栓治疗1周后,CTPA示肺动脉栓塞范围较前减少,但肺梗死却较前增多,新出现右肺中叶椭圆形肺梗死(黄箭),其内侧可见支气管血管束包埋,右肺下叶驼峰样肺梗死(黑箭);(f)抗凝溶栓治疗后期,右肺下叶肺梗死演变为小索条影(黑箭)。
Figure 2. A 27-year-old male with abdominal pain and fever and pulmonary infarction secondary to acute pulmonary embolism
表 1 41例APE继发PI患者的临床资料
Table 1 Clinical data of 41 patients with pulmonary infarction secondary to acute pulmonary embolism
项目 数量/例 比例/% 项目 数量/例 比例/% 病史 无特殊既往史 6 14.6 临床症状 胸痛 25 61.0 冠心病 9 22.0 呼吸困难 7 17.1 高血压 17 41.5 咯血 0 慢性阻塞性肺疾病 11 26.7 胸闷 5 12.2 糖尿病 4 9.8 咳嗽 14 34.1 肿瘤病史 7 17.1 发热 1 2.4 口服孕药 2 4.9 腹痛 5 12.27 系统性红斑狼疮 1 2.4 D-二聚体 0-1.5 mg/L(正常
参考范围)6 14.6 形成双下肢血栓 31 75.6 右心房血栓 2 4.9 ≥1.5mg/L 35 85.4  下载: 导出CSV
下载: 导出CSV
-
[1] HE H, STEIN M W, ZALTA B, et al. Pulmonary infarction: Spectrum of findings on multidetector helical CT[J]. Journal of Thoracic Imaging, 2006, 21(1): 1−7. DOI: 10.1097/01.rti.0000187433.06762.fb.
[2] STEIN P D, MATTA F, MUSANI M H, et al. Silent pulmonary embolism in patients with deep venous thrombosis: A systematic review[J]. The American Journal of Medicine, 2010, 123(5): 426−431. DOI: 10.1016/j.amjmed.2009.09.037.
[3] ISLAM M, FILOPEI J, FRANK M, et al. Pulmonary infarction secondary to pulmonary embolism: An evolving paradigm[J]. Respirology, 2018, 23(9): 866−872. DOI: 10.1111/resp.13299.
[4] MANÇANANO A D, RODRIGUES R S, BARRETO M M, et al. Incidence and morphological characteristics of the reversed halo sign in patients with acute pulmonary embolism and pulmonary infarction undergoing computed tomography angiography of the pulmonary arteries[J]. Jornal Brasileiro de Pneumologia: Publicacao Oficial da Sociedade Brasileira de Pneumologia Tisilogia, 2019, 45(1): e20170438. DOI: 10.1590/1806-3713/e20170438.
[5] 李菲, 唐笑先, 师建强, 等. 不同类型急性肺栓塞临床相关因素分析及胸部继发改变的CT肺动脉成像特征[J]. 中华放射学杂志, 2018,52(1): 9−14. DOI: 10.3760/cma.j.ssn.1005?1201.2018.01.03. LI F, TANG X X, SHI J Q, et al. Clinical correlative factors and CT pulmonary angiography characteristics of secondary changes of chest in different types of acute pulmonary embolism[J]. Chinese Journal of Radiology, 2018, 52(1): 9−14. DOI: 10.3760/cma.j.ssn.1005?1201.2018.01.03. (in Chinese).
[6] GOLDHABER S Z, VISANI L, DE ROSA M. Acute pulmonary embolism: Clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER)[J]. Lancet, 1999, 353: 1386−1389. DOI: 10.1016/s0140-6736(98)07534-5.
[7] MINIATI M. Pulmonary infarction: An often unrecognized clinical entity[J]. Seminars in Thrombosis and Hemostasis, 2016, 42(8): 865−869. DOI: 10.1055/s-0036-1592310.
[8] MARCHIORI E, MENNA BARRETO M, PEREIRA FREITAS H M, et al. Morphological characteristics of the reversed halo sign that may strongly suggest pulmonary infarction[J]. Clinical Radiology, 2018, 73: 503.e7−503.e13. DOI: 10.1016/j.crad.2017.11.022.
[9] TORBICKI A, PERRIER A, KONSTANTINIDES S, et a1. Guidelines on the diagnosis and management of acute pulmonary embolism: The task force for the diagnosis and management of acute pulmonary embolism of the european society of cardiology (ESC)[J]. European Heart Journal, 2008, 29(18): 2276−2315. DOI: 10.1093/eurheartj/ehn310.
[10] KAPTEIN F H J, KROFT L J M, HAMMERSCHLAG G, et al. Pulmonary infarction in acute pulmonary embolism[J]. Thrombosis Research, 2021, 202: 162−169. DOI: 10.1016/j.thromres.2021.03.022.
[11] BLOOMER W E, HARRISON W. Respiratory function and blood flow in the bronchial artery after ligation of the pulmonary artery[J]. The American Journal of Physiology, 1949, 157(2): 317−328. DOI: 10.1152/ajplegacy.1949.157.2.317.
[12] WAGENVOORT C A. Pathology of pulmonary thromboembolism[J]. Chest, 1995, 107(Sl): 10S−17S. DOI: 10.1378/chest.107.1_supplement.10s.
[13] VOLOUDAKI A E, BOUROS D E, FROUDARAKIS M E, et al. Crescentic and ring-shaped opacities: CT features in two cases of bronchiolitis obliterans organizing pneumonia (BOOP)[J]. Acta Radiologica, 1996, 37(6): 889−892. DOI: 10.1177/02841851960373P289.
[14] MARCHIORI E, HOCHHEGGER B, ZANETTI G. Importance of the reversed halo sign for diagnosis of mucormycosis[J]. The Lancet. Infectious Diseases, 2020, 20(5): 538. DOI: 10.1016/S1473-3099(20)30266-8.
[15] 蒋玮丽, 龙斌, 柏玉涵, 等. 新型冠状病毒肺炎的胸部CT特征[J]. 中国医学影像学杂志, 2020,28(11): 817−819, 824. DOI: 10.3969/j.issn.1005-5185.2020.11.005. JIANG W L, LONG B, BAI Y H, et al. Chest CT features of COVID-19[J]. Chinese Journal of Medical Imaging, 2020, 28(11): 817−819, 824. DOI: 10.3969/j.issn.1005-5185.2020.11.005. (in Chinese).
[16] SALES A R, CASAGRANDE E M, HOCHHEGGER B, et al. The reversed halo sign and COVID-19: Possible histopathological mechanisms related to the appearance of this imaging finding[J]. Archivos de Bronconeumologia, 2021, 57: 73−75. DOI: 10.1016/j.arbres.2020.06.029.
[17] 张旭辉, 陈晓荣, 陈涛. 以反晕征为主要表现的间质型肺结核一例[J]. 放射学实践, 2020,2: 253−254. doi: 10.13609/j.cnki.1000-0313.2020.02.027 [18] MARCHIORI E, ZANETTI G, IRION KL, et al. Reversed halo sign in active pulmonary tuberculosis: Criteria for differentiation from cryptogenic organizing pneumonia[J]. American Journal of Roentgenology, 2011, 197: 1324−1327. DOI: 10.2214/AJR.11.6543.
[19] 童永秀, 张玮, 张惠娟, 等. 以反晕征为主要CT表现的继发性肺结核影像特征分析[J]. 临床放射学杂志, 2020,(1): 69−72. DOI: 10.13437/j.cnki.jcr.2020.01.014. TONG Y X, ZHANG W, ZHANG H J, et al. Aanlysis the imaging features of secondary pulmonary tuberculosis with reversed halo sign as the manifestation[J]. Journal of Clinical Radiology, 2020, (1): 69−72. DOI: 10.13437/j.cnki.jcr.2020.01.014. (in Chinese).
[20] 车宏伟, 张晓琴, 柴军, 等. 新型冠状病毒肺炎临床表现及CT影像学分析[J]. CT理论与应用研究, 2021,30(4): 525−532. DOI: 10.15953/j.1004-4140.2021.30.04.14. CHE H W, ZHANG X Q, CHAI J, et al. Clinical manifestations and CT imaging analysis of corona virus disease 2019[J]. CT Theory and Applications, 2021, 30(4): 525−532. DOI: 10.15953/j.1004-4140.2021.30.04.14. (in Chinese).
[21] NATTUSAMY L, MADAN K, KHILNANI G C, et al. Pulmonary infarction in acute pulmonary embolism: Reversed halo sign[J]. BMJ Case Reports, 2014: bcr2014205181. DOI: 10.1136/bcr-2014-205181.
[22] GOSHIMA H, TOMIOKA H, NISHIO C, et al. Reversed halo sign in pulmonary infarction with tumor emboli: A case report[J]. Respiratory Investigation, 2014, 52(3): 199−202. DOI: 10.1016/j.resinv.2013.08.004.
[23] 周旭辉, 李菁, 李子平, 等. 肺动脉栓塞中发生肺梗死的CT表现及相关因素分析[J]. 中华放射学杂志, 2006,40(5): 502−506. DOI: 10.3760/j.issn:1005-1201.2006.05.012. ZHOU X H, LI J, LI Z P, et al. Analysis of finding and correlative factors for pulmonary infarction complicated with pulmonary embolism[J]. Chinese Journal of Radiology, 2006, 40(5): 502−506. DOI: 10.3760/j.issn:1005-1201.2006.05.012. (in Chinese).
[24] CHOI S H, CHA S I, SHIN K M, et al. Clinical relevance of pleural effusion in patients with pulmonary embolism[J]. Respiration, 2017, 93(4): 271−278. DOI: 10.1159/000457132.
[25] KOCIJANCIC I, VIDMAR J, KASTELIC M. Dynamics of CT visible pleural effusion in patients with pulmonary infarction[J]. Radiology and Oncology, 2018, 52(3): 245−249. DOI: 10.2478/raon-2018-0033.
[26] 王璐, 易坤明, 毛锐利, 等. 大叶性肺炎与肺炎型肺癌患者的CT影像分析[J]. 中华医院感染学杂志, 2018,28(23): 3568−3571. DOI: 10.11816/cn.ni.2018-173844. WANG L, YI K M, MAO R L, et al. CT imaging study of patients with lobar pneumonia and pneumonia-type lung cancer[J]. Chinese Journal of Nosocomiology, 2018, 28(23): 3568−3571. DOI: 10.11816/cn.ni.2018-173844. (in Chinese).
[27] 王庆宜, 李万湖, 张德贤, 等. 原发性肺浸润型黏液腺癌影像学表现及病理特点[J]. 中华肿瘤防治杂志, 2020,27(8): 647−652, 657. DOI: 10.16073/j.cnki.cjcpt.2020.08.11. WANG Q Y, LI W H, ZHANG D X, et al. Imaging findings and pathological features of primary lung invasive mucinous adenocarcinoma[J]. Chinese Journal of Cancer Prevention and Treatment, 2020, 27(8): 647−652, 657. DOI: 10.16073/j.cnki.cjcpt.2020.08.11. (in Chinese).
-
期刊类型引用(2)
1. 黄盛晶,周昌盛,张霖,卢璐,张小宇. 以反晕征为主要CT表现的肺栓塞临床及影像特点分析. 温州医科大学学报. 2024(02): 146-150+155 .  百度学术
百度学术
2. 张锐,刘崇华,杨奉常,袁双虎. 肺癌合并肺梗死患者临床病理特征和预后影响因素. 中华肿瘤防治杂志. 2024(12): 746-751 . 百度学术
其他类型引用(0)

计量
- 文章访问数: 355
- HTML全文浏览量: 229
- PDF下载量: 42
- 被引次数: 2


