
The Predictive Value of CT Findings in Invasive Behavior of Pancreatic Neuroendocrine Tumors
-
摘要: 目的:探讨胰腺神经内分泌肿瘤(pNET)的CT征象对其侵袭性行为的预测价值。方法:回顾性分析经手术病理确诊、临床及CT资料完整、术前均行胰腺CT平扫及增强检查的120例pNET,分析病灶的部位、形态、包膜、有无囊变和钙化、有无胰管扩张、肿瘤的强化方式,测量肿瘤最大径、最短径以及实性部分平扫、动脉期及门脉期密度,并计算动脉期强化差值、门脉期强化差值。根据手术病理结果将肿瘤分为侵袭组和无侵袭组,比较两组间CT征象的差异。使用绘制受试者操作特征(ROC)曲线评价肿瘤最大径、最短径、动脉期差值和门脉期差值对pNET的侵袭性行为的预测价值。结果:侵袭组和无侵袭组pNET在发病部位、胰管扩张、囊变、钙化及强化方式无差异,在形态、完整包膜上有差异。两组在最大径、最短径、动脉期强化差值、门脉期强化差值定量特征有差异,其ROC曲线下面积为0.693、0.69、0.73和0.64,具有判别效能。对6个差异有统计学意义的影像特征通过多变量Logistic回归分析,结果显示动脉期强化差值为判断pNET侵袭性行为的独立预测因素,动脉期强化差值最佳临界点为90.1 HU(灵敏度0.714,特异性0.656,阳性预测值64.5%,阴性预测值72.4%,准确率68.3%)。结论:胰腺神经内分泌肿瘤体积大、形态不规则、包膜不完整或无包膜,肿瘤实性成分动脉期、门脉期强化差值低等征象提示肿瘤具有侵袭性行为,其中动脉期强化差值为pNET侵袭性行为的独立预测因素。Abstract: Objective: To explore the value of CT findings in predicting the invasive behaviors of pancreatic neuroendocrine tumor (pNET). Methods: The clinical data and CT data of 120 patients with pNET confirmed by surgical resection and pathology were retrospectively analyzed. Preoperative CT plain scan and enhanced examination of pancreas were performed. Image analysis included tumor location, shape, capsule, cystic change, calcification, pancreatic duct dilation and enhancement pattern. The maximum and minimum diameter of the tumor were measured. The CT value of the solid part of the tumor was measured in plain scan, arterial phase and portal vein phase. Enhancement difference in arterial phase and portal vein phase were calculated. The tumors were divided into invasive group and non-invasive group according to the pathological results. The difference of CT findings between the two groups was compared. Receivers operating characteristic (ROC) curves were drawn to evaluate the predictive value of tumor maximum diameter, minimum diameter, enhancement difference in arterial phase and portal vein phase on the invasive behavior of pNET. Results: There were no statistical differences in tumor location, pancreatic duct dilation, cystic change, calcification and enhancement pattern between the invasive and non-invasive groups. There were statistically significant differences between the two groups in the quantitative characteristics of the maximum diameter, the minimum diameter, enhancement difference in arterial phase and portal vein phase and the areas under ROC curve were 0.693, 0.69, 0.73 and 0.64, indicating discrimination efficiency. Multivariate Logistic regression analysis of 6 meaningful image features showed that arterial enhancement difference was an independent predictor of pNET invasive behavior, and the optimal critical point of arterial enhancement difference was 90.1HU (sensitivity 0.714, specificity 0.656, positive predictive value 64.5%, negative predictive value 72.4%, accuracy 68.3%). Conclusion <b<:</b< Large volume, irregular shape, incomplete or no capsule of pancreatic neuroendocrine tumor, and low enhancement difference of solid tumor components in arterial and portal phases suggested invasive behavior of tumor, and enhancement difference in arterial phase was an independent predictor of invasive behavior of pNET.
-
Keywords:
- tomography /
- X-ray computer /
- pancreatic neoplasms /
- neuroendocrine tumor
-
-
![]()
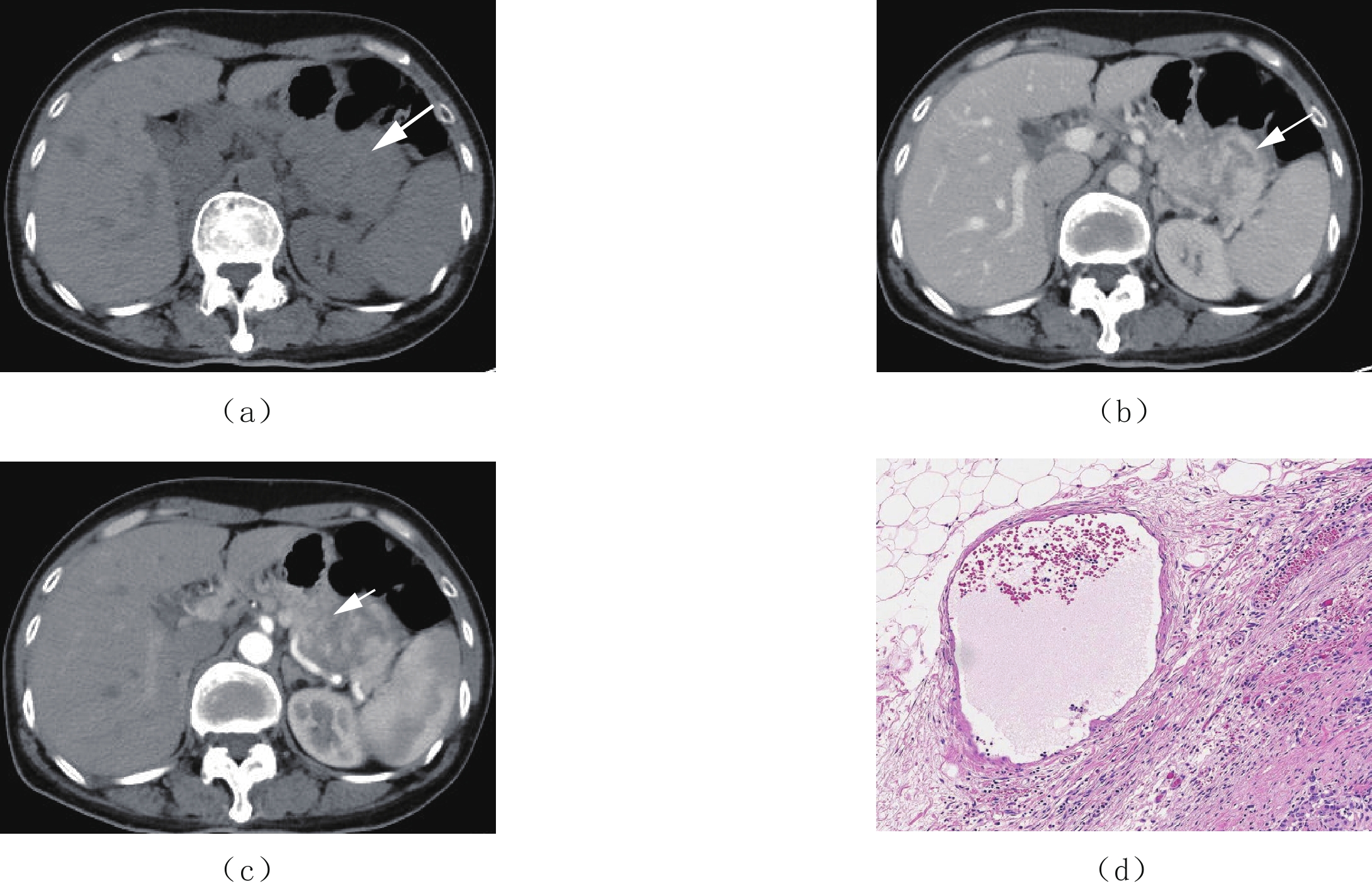
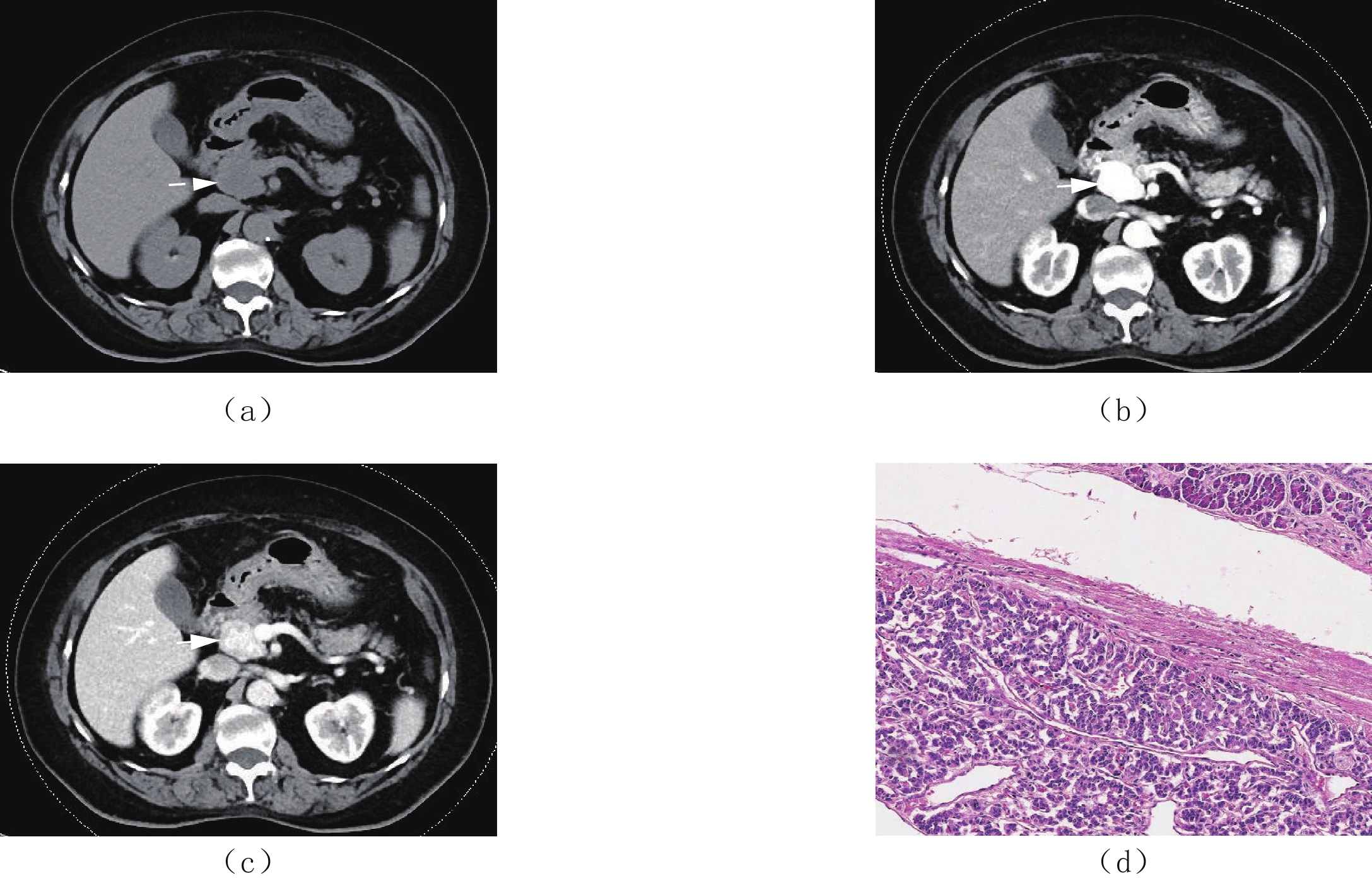
图 1 女,75岁,非侵袭性胰腺神经内分泌肿瘤
(a)为CT平扫,示胰头部见一类椭圆形稍低密度灶,密度均匀,边界清。(b)为增强扫描动脉期,示病灶重度强化,强化程度明显高于周围胰腺组织,病灶与胰腺交界面见肿瘤包膜。(c)为增强扫描门脉期,示病灶强化程度不均匀减低,实性部分密度仍高于胰腺组织,分界清,病灶为实性,无囊变坏死。(d)为病理图片,示肿瘤组织呈膨胀性生长,与胰腺组织分界清晰,肿瘤细胞呈器官样排列,细胞形态、大小较一致(HE染色×100)。
Figure 1. Female, 75 years old with a non-invasive pancreatic neuroendocrine tumor
![]()
图 2 女,55岁,侵袭性胰腺神经内分泌肿瘤
(a)为CT平扫,示胰尾部见一巨大不规则等密度肿块,密度不均匀,内可见条片低密度影,边界不清。(b)为增强扫描动脉期,示病灶中度不均匀强化,病灶与胰腺交界面未见肿瘤包膜,与周围血管、结肠壁、胃壁分界不清。(c)为增强扫描门静脉期,示病灶实性持续渐进性强化,内见囊变坏死不强化影,病灶以实性成分为主。(d)为病理图片,示肿瘤组织呈浸润性生长,侵犯胰腺周围纤维脂肪组织;肿瘤细胞呈片状排列,细胞大小不一致,部分细胞异型明显,核仁可见(HE染色×100)。
Figure 2. Female, 55 years old with a invasive pancreatic neuroendocrine tumor
![]()
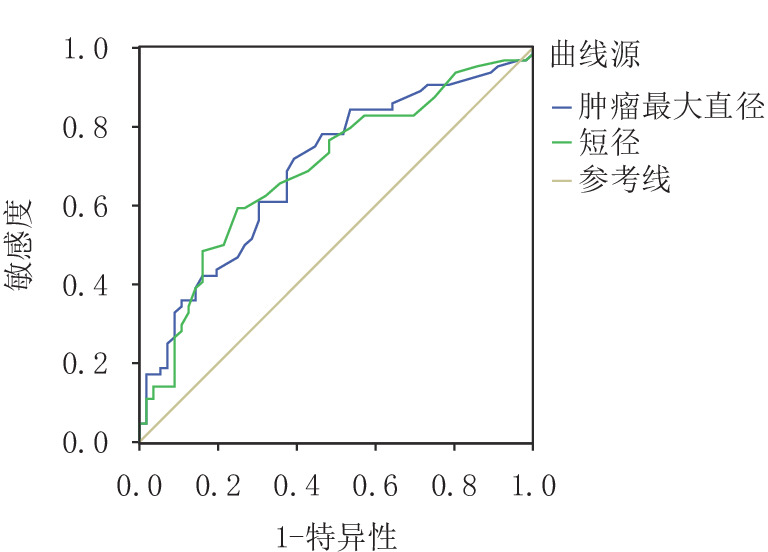
图 3 肿瘤最大径、最短径预测pNET侵袭性行为的受试者操作特征(ROC)曲线
Figure 3. ROC curves of maximum and minimum tumor diameters to predict invasive behavior of pNET
![]()
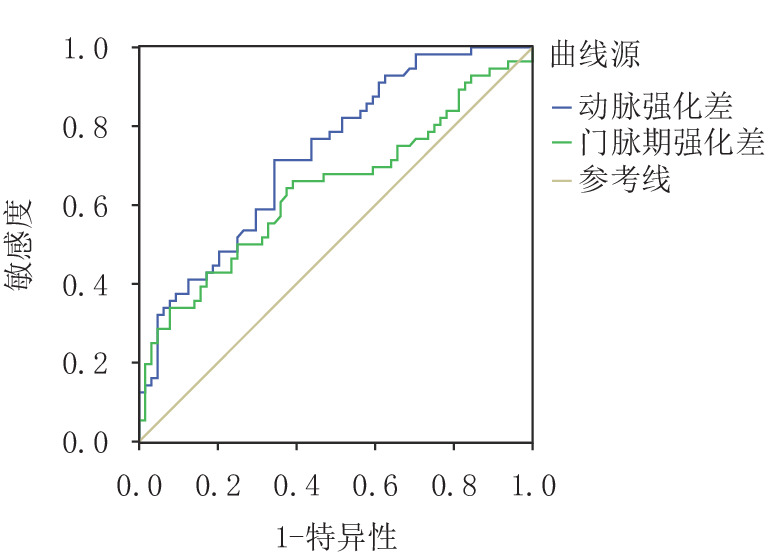
图 4 肿瘤实性成分的动脉期强化差值、门静脉期强化差值程度预测pNET侵袭性行为的受试者操作特征(ROC)曲线
Figure 4. ROC curves for predicting invasive behavior of pNET by arterial enhancement difference and portal enhancement difference of tumor solid component
![]()
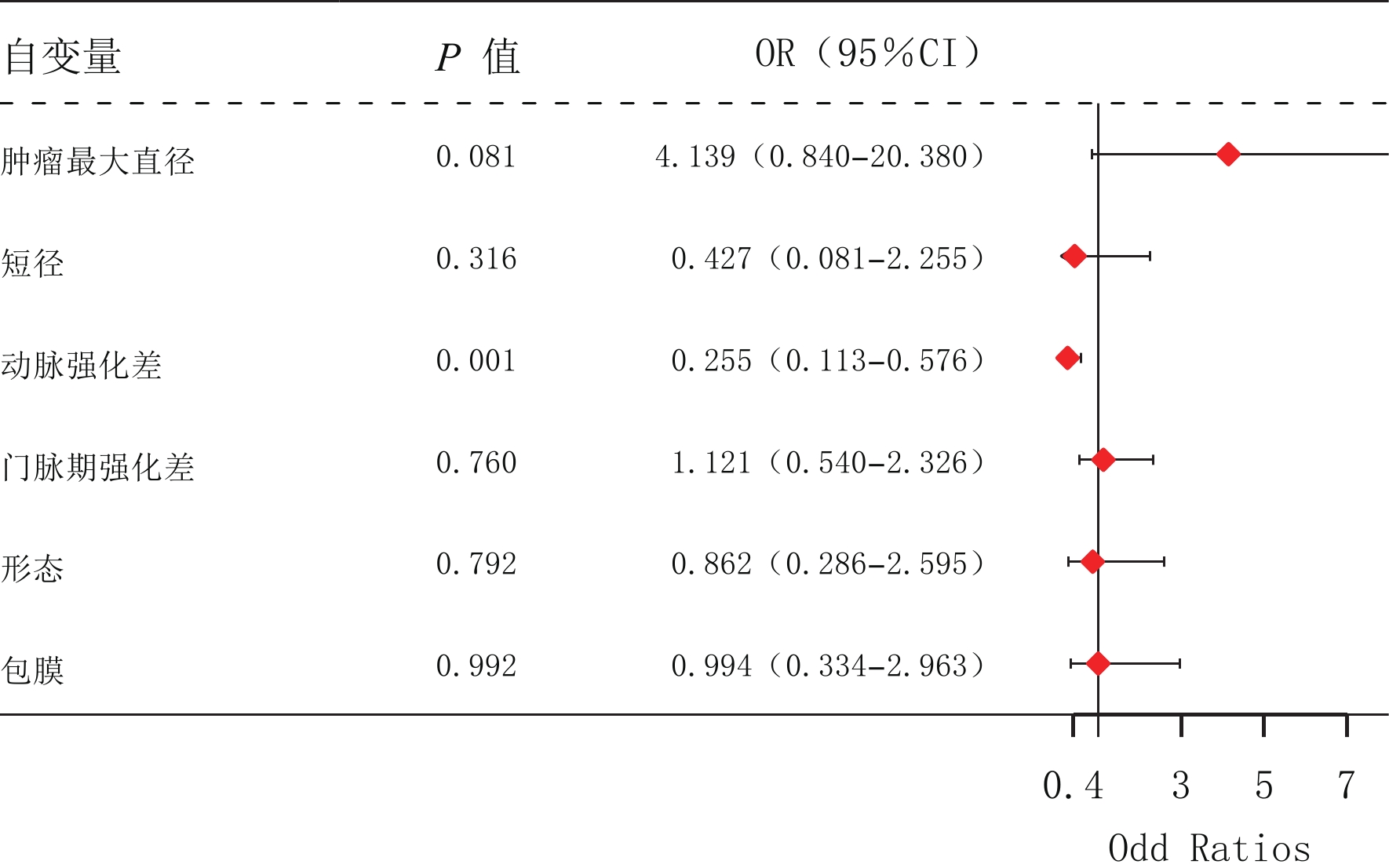
图 5 对6个有统计学意义的影像特征的多变量Logistic回归分析
Figure 5. Multivariate Logistic regression analysis of six statistically significant image features
表 1 侵袭组与无侵袭组pNET的临床特征比较
Table 1 Comparison of clinical characteristics of pNET between the invasive group and the non-invasive group
组别 例数 年龄/岁 性别/例 临床症状
/例基础疾病/例 血清神经元特
异性烯醇化酶
/(ng/mL)分泌功能
/例病理分级
/例男 女 有 无 无 1种 ≥2种 是 否 G1 G2 G3 侵袭组 64 53.72±12.89 33 31 31 33 43 17 4 18.93±6.82 31 33 20 34 10 无侵袭组 56 51.95±14.97 25 31 34 22 44 8 4 30.53±51.13 38 18 38 18 0 统计量 0.485a 0.573b 1.813b 2.730b -1.123 4.609b 20.065b P 0.487 0.470 0.202 0.255 0.261 0.042 <0.001 注:a:t值;b:χ2值。  下载: 导出CSV
下载: 导出CSV
表 2 侵袭组与无侵袭组pNET的CT影像学特征比较结果(例)
Table 2 Comparison of CT imaging features of pNET between the invasive group and the non-invasive group (cases)
组别 例数 位置 形态 包膜 胰管扩张 囊变 钙化 强化方式 头颈部 体部 尾部 规则 不规则 完整 不完整
或无有 无 有 无 有 无 均匀 不均匀 侵袭组 64 27 12 25 27 37 22 42 21 43 22 42 15 49 24 40 无侵袭组 56 25 15 16 47 9 49 7 13 43 15 41 8 48 25 31 统计值 1.861 22.013 34.889 1.355 0.807 1.615 0.933 P 0.394 <0.001 <0.001 0.311 0.430 0.249 0.354
下载: 导出CSV
表 3 侵袭组与无侵袭组pNET的CT影像学特征比较结果
Table 3 Comparison of CT imaging features of pNET between the invasive group and the non-invasive group
组别 例数 最大径/cm 最短径/cm 肿瘤实性成分强化差值/HU 动脉期差值 门脉期差值 侵袭组 64 4.051±2.920 3.062±2.051 80.933±48.281 73.801±28.912 无侵袭组 56 2.511±1.542 2.084±1.220 112.912±61.953 89.882±39.901 统计检验 统计值 12.518 9.905 10.071 6.501 P 0.001 0.002 0.002 0.012
下载: 导出CSV
-
[1] 吴文铭, 陈洁, 白春梅, 等. 中国胰腺神经内分泌肿瘤诊疗指南(2020)[J]. 中华外科杂志, 2021,59(6): 401−421. DOI: 10.3760/cma.j.cn112139-20210319-00135. WU W M, CHEN J, BAI C M, et al. The Chinese guidelines for the diagnosis and treatment of pancreatic neuroendocrine neoplasms (2020)[J]. Chinese Journal of Surgery, 2021, 59(6): 401−421. DOI: 10.3760/cma.j.cn112139-20210319-00135. (in Chinese).
[2] 敖炜群, 杨光钊, 王健, 等. 非典型胰腺神经内分泌肿瘤的影像学特征[J]. 中华胰腺病杂志, 2020,20(6): 458−461. doi: 10.3760/cma.j.cn115667-20200416-00054 [3] XU W, YAN H, XU L, et al. Correlation between radiologic features on contrast-enhanced CT and pathological tumor grades in pancreatic neuroendocrine neoplasms[J]. The Journal of Biomedical Research, 2020, 35(3): 179−188. DOI: 10.7555/JBR.34.20200039.
[4] OHKI K, IGARASHI T, ASHIDA H, et al. Usefulness of texture analysis for grading pancreatic neuroendocrine tumors on contrast-enhanced computed tomography and apparent diffusion coefficient maps[J]. Japanese Journal of Radiology, 2021, 39(1): 66−75. DOI: 10.1007/s11604-020-01038-9.
[5] KANG J, RYU J K, SON J H, et al. Association between pathologic grade and multiphase computed tomography enhancement in pancreatic neuroendocrine neoplasm[J]. Journal of Gastroenterology and Hepatology, 2018. DOI: 10.1111/jgh.14139.
[6] BELOUSOVA E, KARMAZANOVSKY G, KRIGER A, et al. Contrast-enhanced MDCT in patients with pancreatic neuroendocrine tumours: Correlation with histological findings and diagnostic performance in differentiation between tumour grades[J]. Clinical Radiology: Journal of the Royal College of Radiologists, 2017, 72(2): 150−158. DOI: 10.1016/j.crad.2016.10.021.
[7] BICCI E, COZZI D, FERRARI R, et al. Pancreatic neuroendocrine tumours: Spectrum of imaging findings[J]. Gland Surgery, 2020, 9(6): 2215−2224. DOI: 10.21037/gs-20-537.
[8] PENITENTI F, LANDONI L, SCARDONI M, et al. Clinical presentation, genotype-phenotype correlations, and outcome of pancreatic neuroendocrine tumors in Von Hippel-Lindau syndrome[J]. Endocrine, 2021, 74(1): 180−187. DOI: 10.1007/s12020-021-02752-8.
[9] YANG M, TIAN B, ZHANG Y, et al. Epidemiology, diagnosis, surgical treatment and prognosis of the pancreatic neuroendocrine tumors: Report of 125 patients from one single center[J]. Indian Journal of Cancer, 2015, 52(3): 343−349. DOI: 10.4103/0019-509X.176746.
[10] LI W X, MIAO F, XU X Q, et al. Pancreatic neuroendocrine neoplasms: CT spectral imaging in grading[J]. Academic Radiology, 2021, 28(2): 208−216. DOI: 10.1016/j.acra.2020.01.033.
[11] OKABE H, HASHIMOTO D, CHIKAMOTO A, et al. Shape and enhancement characteristics of pancreatic neuroendocrine tumor on preoperative contrast-enhanced computed tomography may be prognostic indicators[J]. Annals of Surgical Oncology, 2017, 24(5): 1399−1405. DOI: 10.1245/s10434-016-5630-4.
[12] CANELLAS R, BURK K S, PARAKH A, et al. Prediction of pancreatic neuroendocrine tumor grade based on CT features and texture analysis[J]. American Journal of Roentgenology, 2018, 210(2): 341−346. DOI: 10.2214/AJR.17.18417.
[13] GAO H, WANG W, ZHANG W, et al. The distinctive characteristics of the micro-vasculature and immune cell infiltration in cystic pancreatic neuroendocrine tumors[J]. Journal of Endocrinological Investigation, 2021, 44(5): 1011−1019. DOI: 10.1007/s40618-020-01396-1.
[14] JAYSON G C, KERBEL R, ELLIS L M, et al. Antiangiogenic therapy in oncology: Current status and future directions[J]. Lancet, 2016, 388(10043): 518−529. DOI: 10.1016/S0140-6736(15)01088-0.
[15] CHU X, GAO X, JANSSON L, et al. Multiple microvascular alterations in pancreatic islets and neuroendocrine tumors of a Men1 mouse model[J]. American Journal of Pathology, 2013, 182(6): 2355−2367. DOI: 10.1016/j.ajpath.2013.02.023.
[16] WORHUNSKY D J, KRAMPITZ G W, POULLOS P D, et al. Pancreatic neuroendocrine tumours: Hypoenhancement on arterial phase computed tomography predicts biological aggressiveness[J]. The Official Journal of the International Hepato Pancreato Biliary Association, 2014, 16(4): 304−311. DOI: 10.1111/hpb.12139.
-
期刊类型引用(5)
1. 马海豹. 机场智能旅检线系统设计及关键技术研究. 信息与电脑(理论版). 2024(01): 108-110 .  百度学术
百度学术
2. 吴桐. 民航安检新技术应用与效能提升策略. 科技视界. 2024(21): 62-65 . 百度学术
3. 杨栋,朱建生,唐雯. 基于智能调度技术的铁路客运安检集中判图系统研究. 铁道运输与经济. 2023(10): 133-141 . 百度学术
4. 常敏,李光飞,吝特高,刘勇,张宽,徐小波. 智能旅检通道模式下机场旅客安检效率研究. 中国民航大学学报. 2022(04): 49-53 . 百度学术
5. 陈昶卓,陈志强. 痕量探测技术在航空安检的应用及前景展望. 民航学报. 2022(06): 106-115 . 百度学术
其他类型引用(6)
计量
- 文章访问数: 206
- HTML全文浏览量: 72
- PDF下载量: 21
- 被引次数: 11


