
Spectral CT Multi-material Decomposition in Evaluation of Secondary Lower Extremity Lymphedema: A Prospective Study
-
摘要: 目的:探讨能谱CT多物质解析算法在继发性下肢淋巴水肿分级评价中的应用价值。材料及方法:前瞻性收集2019年6月至2020年6月因继发性下肢淋巴水肿入我院就诊并行能谱CT断层扫描的患者,由两名具有5年以上CT诊断经验的医师共同对能谱CT图像进行分析,采用阈值法测量患侧与健侧下肢体积,计算(患侧下肢体积 - 健侧下肢体积)/健侧下肢体积的百分比,根据2016版国际淋巴学会共识,将入组患者分为轻度、中度、重度;使用能谱CT多物质解析算法分别测量患侧与健侧下肢脂肪含量,得出脂肪体积分数,采用配对<i<t</i<检验分别分析轻、中、重度患者患侧与健侧下肢脂肪体积分数之间的差异;采用秩和检验分别分析轻、中、重度患者两两之间患侧下肢脂肪体积分数的差异。结果:最终入组患者 40例,女/男(36/4),年龄范围32~71岁,中位年龄(53±10)岁,病程(3±5)年,轻度8例,中度14例,重度18例。轻、中、重度患者的患侧与健侧下肢脂肪体积分数之间差异均有统计学意义;轻、中、重度患者两两之间患侧下肢脂肪体积分数差异无统计学意义。结论:能谱CT多物质解析算法可以量化继发性下肢淋巴水肿的脂肪含量比,但不能单独用于下肢病变的分级评价中。Abstract: Objective: To explore the application value of spectral CT multi-material decomposition (MMD) algorithm in the grading of secondary lower extremity Lymphedema. Materials and methods: Prospective collection of patients who underwent spectral CT admitted to our hospital from June 2019 to June 2020 were prospectively collected. The spectral CT images were analyzed by two radiologists with more than five years of experience in CT diagnosis. The volume of the both lower limbs were measured using the threshold value software. Based on the percentage increase in the volume of the affected side compared to the healthy side, the enrolled patients were divided into three grades: mild, moderate, and severe. Percentage fat volume fraction (FVF) images were generated by using the MMD algorithm on spectral CT to measure the fat content of the affected and healthy lower limbs respectively. Paired <i<t</i< test were used to analyze the difference of the percentage FVF between the affected and healthy side in mild, moderate, severe patients. Results: Forty patients (female/male, 36/4 cases, with age range of 32-71 years old, median age of (53±10) years) were finally enrolled, and the course of disease was (3±5) years. There were 8 cases in mild group, 14 cases in moderate group and 18 cases in severe group. There were statistical differences in the percentage FVF between the affected and healthy side in mild, moderate and severe patients. There was no statistical difference in the percentage FVF of the affected side among mild, moderate and severe patients.Conclusion: The spectral CT MMD algorithm can quantify the percentage FVF of Secondary Lower Extremity Lymphedema, but it cannot be used alone in the grading of secondary lower extremity lymphedema.
-
Keywords:
- spectrum CT /
- MMD /
- lower extremity lymphedema /
- grade
-
继发性下肢淋巴水肿作为一种慢性致残性疾病,多由腹盆腔恶性肿瘤切除和/或放射治疗损伤淋巴系统所致,患者常伴有下肢肿胀、疼痛、活动受限等症状,继发于妇科恶性肿瘤术后的下肢淋巴水肿发生率可高达60%[1-2],严重影响癌症幸存者心理健康与生活质量,但是目前临床上并没有理想的治疗方式适用于所有继发性下肢淋巴水肿的患者[3],因此明确下肢淋巴水肿诊断与分级对癌症幸存者意义深远。
仅依据2016版国际淋巴学会共识[4]中患肢体积较健肢体积增大的百分比将患者分为轻、中、重3级,不足以明确疾病进展程度,这主要是因为继发性淋巴水肿患者肢体体积增大的成分多样,包括脂肪及纤维化等[5],即使体积增大比例一致,以脂肪为主型和纤维化为主型的不同患者手术的难度和风险也大相径庭[6]。此外,处于不同分级的患者组织增加的成分也可能相同。
能谱CT不仅可通过阈值测量法量化体积,还可利用不同物质在不同X线能量下的吸收情况提供比常规CT更多的信息[7],本研究通过能谱CT多物质解析算法量化淋巴水肿肢体脂肪含量比,以期为临床提供更多的分级诊断信息。
1. 材料与方法
1.1 一般资料
本研究通过医院伦理委员会批准,搜集2019年6月至2020年6月因继发性下肢淋巴水肿入我院就诊的40例患者。
入组标准:①恶性肿瘤根治性切除术后和/或放射治疗后出现单侧下肢淋巴水肿的患者;②于下肢淋巴水肿治疗前行能谱CT检查的患者;③签署知情同意书的患者。排除标准:①原发性下肢淋巴水肿患者以及其它任何原因如心源性、血管源性、肝肾功能不全、代谢性疾病等导致的下肢水肿患者;②合并恶性肿瘤复发和/或淋巴结转移的患者。
1.2 能谱CT成像与后处理
所有检查均在GE Revolution CT完成,扫描范围自盆腔至双足,患者双腿保持解剖学定位,双脚稍微分开。扫描参数:管电压80/140 kVp快速切换,管电流自动调节模式100~200 mA,噪声指数12,Asir比例40%,球管旋转时间0.5 s,螺距0.992∶1,探测器宽度8 cm,矩阵512×512,SFOV 50 cm。
所得原始数据均以2.5 mm层厚,2.5 mm层间隔进行三维重组,所得能谱CT图像均导入GE AW 4.7工作站,使用水-脂肪作为基物质对进行后处理,将原始图像处理为水基和脂肪基物质图,将所得脂肪基物质图分别重组为轴面、冠状面、矢状面图像。
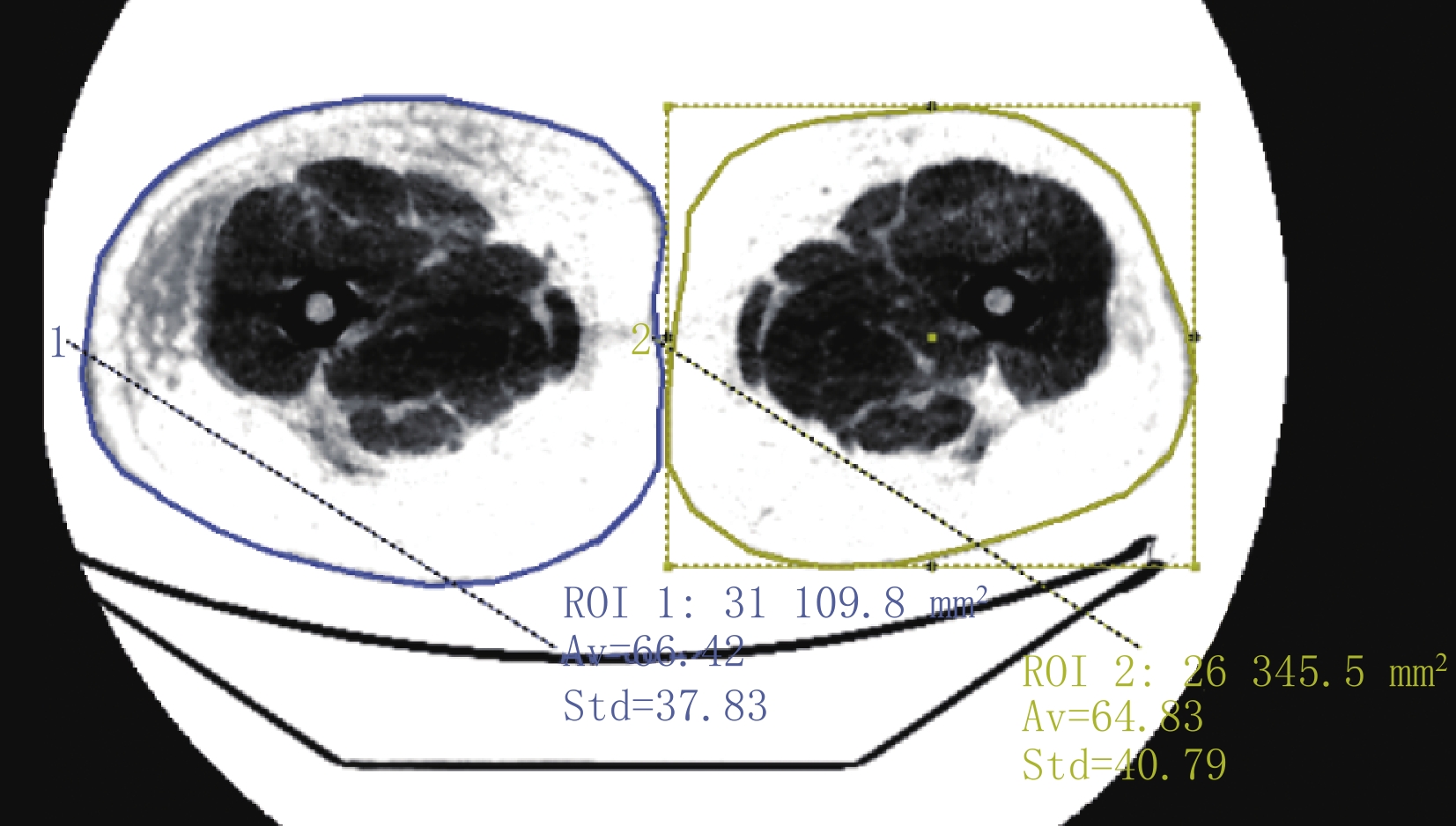
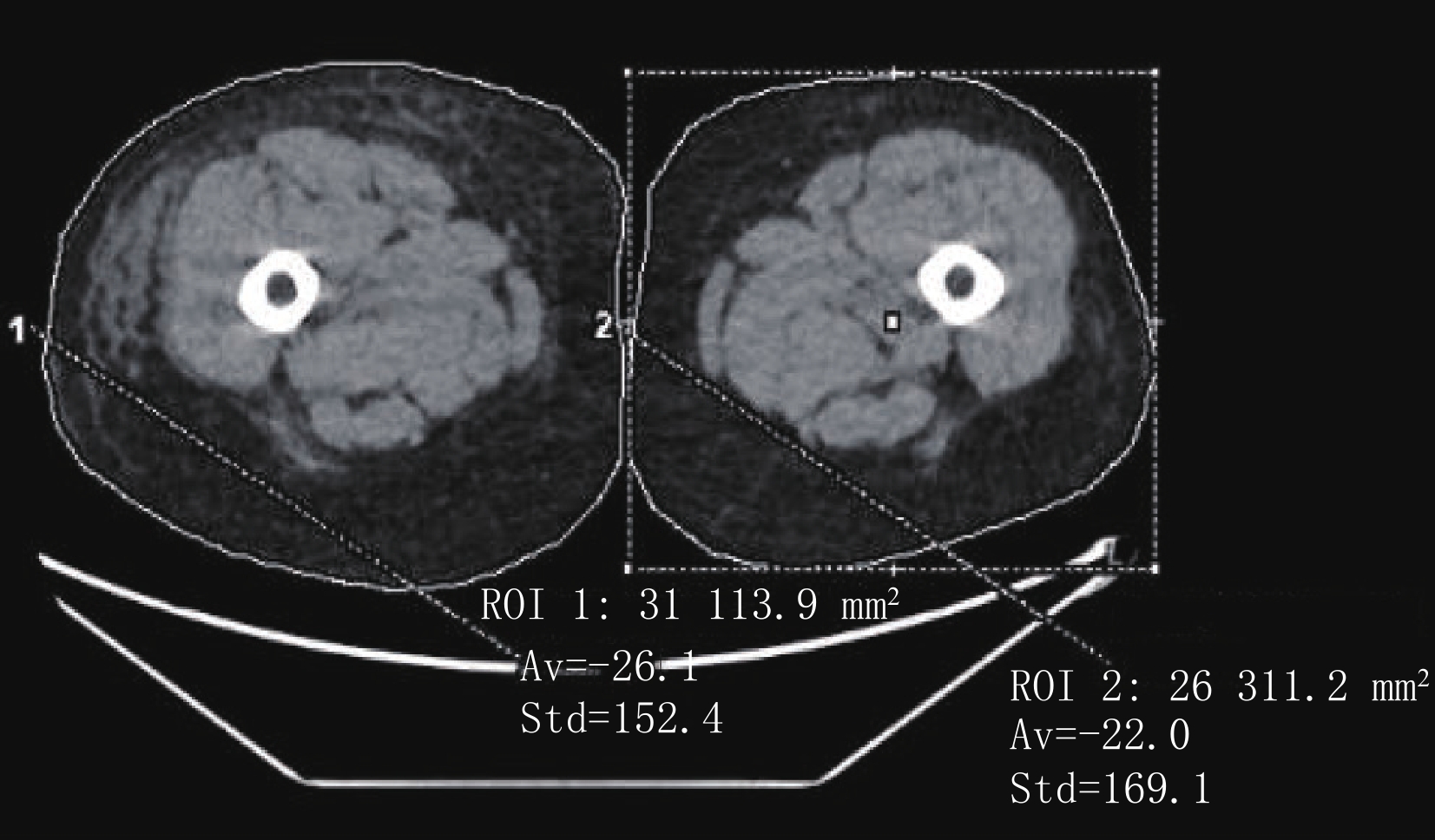
采用CT阈值法分别测量患侧与健侧下肢体积(图 1)。基于多物质解析的脂肪量化算法显示2.5 mm层厚的脂肪体积分数图像(图 2),对下肢脂肪含量进行定量评估,分别选取患侧及健侧全下肢作为感兴趣区域,记录患侧及健侧全下肢脂肪体积分数值。为了确保观察者间和观察者内的一致性,所有能谱CT图像均由两名5年以上工作经验的放射科医生共同测量。
![]() 图 1 能谱CT平扫下肢轴面图像,分别选取患侧与健侧同层面为感兴趣区,该截面患侧和健侧肢体脂肪体积(cm3)分别为26.1±152.4和22.0±169.1Figure 1. The axial image of lower extremity by spectral CT plain scan. The same section of the affected and healthy side were selected as the ROIs, the fat volume of the affected and healthy side on this section (cm3) is 26.1±152.4 and 22.0±169.1, respectively
图 1 能谱CT平扫下肢轴面图像,分别选取患侧与健侧同层面为感兴趣区,该截面患侧和健侧肢体脂肪体积(cm3)分别为26.1±152.4和22.0±169.1Figure 1. The axial image of lower extremity by spectral CT plain scan. The same section of the affected and healthy side were selected as the ROIs, the fat volume of the affected and healthy side on this section (cm3) is 26.1±152.4 and 22.0±169.1, respectively![]() 图 2 下肢轴面脂肪体积分数CT图像,分别选取患侧与健侧同层面为感兴趣区,该截面患侧和健侧肢体脂肪体积分数(%)分别为:66.42±37.83和64.83±40.79Figure 2. The axial FVF image of the lower extremity. The same section of the affected and healthy side were selected as the ROIs, the percentage FVF of the affected and healthy side on this section is 66.42±37.83 and 64.83±40.79, respectively
图 2 下肢轴面脂肪体积分数CT图像,分别选取患侧与健侧同层面为感兴趣区,该截面患侧和健侧肢体脂肪体积分数(%)分别为:66.42±37.83和64.83±40.79Figure 2. The axial FVF image of the lower extremity. The same section of the affected and healthy side were selected as the ROIs, the percentage FVF of the affected and healthy side on this section is 66.42±37.83 and 64.83±40.79, respectively1.3 统计学分析
所有数据均采用SPSS 25.0版软件进行统计分析,分别计算CT阈值测量法所得患侧与健侧下肢体积的中位数及标准差。计算(患侧下肢体积 - 健侧下肢体积)/健侧下肢体积的结果,参照2016版国际淋巴协会共识分级标准,将入组患者分为轻、中、重度3级。
采用配对 t 检验分别分析轻、中、重度患者患侧与健侧下肢脂肪体积分数之间的差异。采用秩和检验分析轻、中、重度患者之间患侧下肢脂肪体积分数的差异。P<0.05认为差异有统计学意义。
2. 结果
2.1 患者一般资料
最终入组患者40例,女/男(36/4),年龄范围32~71岁,中位年龄(53±10)岁,病程(3±5)年,主要临床表现为单侧下肢肿胀(左侧24例,右侧16例)、疼痛、活动受限。其中继发于子宫内膜癌7例,宫颈癌22例,卵巢癌4例,腹股沟肿瘤4例,阴茎癌1例,下肢皮肤病变2例。轻度8例,中度14例,重度18例。
2.2 测量结果及统计学分析
CT阈值法测得全组、轻度、中度以及重度患者的患侧与健侧下肢体积值见表1,全组、轻度、中度以及重度患者患侧与健侧下肢体积差异均有统计学意义。
表 1 能谱CT阈值法测量患侧与健侧下肢体积Table 1. The volume of the affected and healthy side by spectral CT threshold value software分级\部位 体积/cm3 统计检验 患侧 健侧 t P 全组(n=40) 9962±2261 6762±1422 11.302 0.000 轻度(n=8) 8358±2213 7379±1862 8.126 0.000 中度(n=14) 8705±1701 6547±1314 15.460 0.000 重度(n=18) 10684±1864 6927±1376 15.487 0.000 能谱CT多物质解析算法测得全组、轻度、中度以及重度患者患侧与健侧下肢脂肪体积分数见表2,全组、轻度、中度以及重度患者的患侧下肢脂肪体积分数与健侧差异均有统计学意义。
表 2 能谱CT多物质解析算法测量患侧与健侧下肢脂肪体积分数Table 2. The percentage FVF of the affected and healthy side by spectral CT MMD algorithm分级\部位 脂肪体积分数/% 统计检验 患侧 健侧 t P 全组(n=40) 58.00±6.98 54.96±8.71 5.195 0.000 轻度(n=8) 57.98±5.96 55.37±7.53 2.430 0.045 中度(n=14) 58.20±9.08 54.36±10.19 3.987 0.002 重度(n=18) 57.86±5.84 55.25±8.42 2.693 0.015 能谱CT阈值测量法显示入组患者的患侧下肢体积均大于健侧下肢体积,这一差异在轻、中、重度组均存在,下肢体积增大百分比最大的患者患侧和健侧下肢体积分别为10071 cm3和4764 cm3,体积增大百分比高达 111%。
能谱CT多物质解析算法显示入组患者的患侧脂肪体积分数均大于健侧脂肪体积分数,这一差异同时存在于轻、中、重度组患者中,体积增大百分比最大的患者患侧和健侧脂肪体积分数分别为48.46% 和 45.04%。
轻、中、重度3组患者两两之间患侧下肢脂肪体积分数的差异均无统计学意义,提示脂肪体积分数这一单一参数不能用于区分轻、中、重度下肢淋巴水肿。
3. 讨论
继发性下肢淋巴水肿是由外伤、感染、放疗和/或手术等引起淋巴回流机械阻塞,患侧下肢淋巴液积聚、脂肪及纤维化等多种成分的增加导致患侧肢体进行性肿胀[8],不同疾病进程的治疗方式不同,淋巴静脉吻合术对继发性下肢淋巴水肿轻度患者更有效,中度和重度患者需联合下肢脂肪抽吸手术[9]。目前临床上主要依据2016版国际淋巴学会共识中体积增大百分比对继发性下肢淋巴水肿患者进行分级诊断,常采用软尺测量下肢多径线,将所得数据代入圆锥体公式计算下肢体积,但是该方法受测量者主观因素影响较大,且是估值数据[10]。
CT阈值法已广泛应用于乳突气房、颅内血肿、肌肉、脏器脂肪等的测量中[11-13],本研究的前期研究已证实CT阈值法与临床多径线测量法对继发性下肢淋巴水肿肢体体积测量的一致性非常好[14]。
研究[15]证明肥胖是发生淋巴水肿的危险因素,并且该风险与体重成正比,与此同时淋巴水肿也可引起功能失调的脂肪细胞肥大和增生,从而导致继发性局部脂肪沉积,这两个过程通过正反馈不断维持和加强。下肢脂肪抽吸术[1,6]可去除过多的皮下脂肪组织,适用于淋巴管功能丧失的患者,可有效缓解患肢肿胀,改善肢体塑性,但是不同脂肪含量患者的手术难度不同。目前临床上急需有效的脂肪体积量化工具,帮助临床医生进行术前预警及术后疗效评价。
文献[7, 16-18]报道中主要的脂肪体积测量方法有:质子磁共振波谱和能谱CT多物质解析算法等,其中质子磁共振波谱是基于组织中脂肪和水的质子密度比来测得脂肪含量的,不是体积测量,应用于脂肪肝患者时还存在脂肪含量高估的情况[7],且磁共振扫描时间长、价格昂贵等也加重了患者负担。相较之下,CT扫描时间短,更具价格优势,快速管电压切换的能谱CT可以生成多个参数并提供定性和定量分析,尤其是能谱CT多物质解析算法,可以区分 3 种甚至更多种不同的物质,生成脂肪体积分数图像对脂肪含量进行定量和可视化评估,尤其适用于成分复杂的人体器官,如血液、脂肪、水和骨骼等,既往的研究证实能谱CT的肝脏脂肪体积分数值准确且可重复[7,17],能谱CT多物质解析技术还可有效识别骨骼、肺和软组织[18],但是目前尚没有应用于淋巴水肿类疾病的报道。
本研究首次将能谱CT多物质解析算法应用于继发性下肢淋巴水肿患者下肢脂肪含量的测量中,与健侧相比,轻、中、重度患者患侧下肢的脂肪体积分数均大于健侧。这符合继发性下肢淋巴水肿患者皮下脂肪沉积的病理生理特征[5,8]。但是轻、中、重度患者两两之间患侧下肢脂肪体积分数的差异无统计学意义,这主要是由于脂肪体积分数是感兴趣区范围内下肢的脂肪占据全下肢的比例,不是绝对量,要受到患侧下肢本体基线体积、增生程度和纤维化程度等多种因素影响[8]。因此,只依据单一参数不具备完全量化分析能力,需结合上述多因素,才能进行准确评价。
本研究的不足:①除了脂肪含量外,纤维化的程度对于评估继发性下肢淋巴水肿严重程度也很重要,下一步的研究需进一步加入纤维化含量的分析;②本研究样本量较小,下一步需要增大样本量,进一步探讨处于同一分级患者的脂肪体积分数是否存在差异;③本次研究中我们没有进行治疗前后脂肪体积分数变化的对比,下一步的研究可将治疗前后进行对照分析,进行疗效评价;④CT扫描具有辐射,但是本研究主要针对恶性肿瘤患者,且辐射剂量远低于多时相腹盆腔CT扫描。
4. 结论
能谱CT多物质解析算法可以量化继发性下肢淋巴水肿的脂肪含量比,但不能单独用于继发性下肢淋巴水肿的分级评价中。
-
![]()
图 1 能谱CT平扫下肢轴面图像,分别选取患侧与健侧同层面为感兴趣区,该截面患侧和健侧肢体脂肪体积(cm3)分别为26.1±152.4和22.0±169.1
Figure 1. The axial image of lower extremity by spectral CT plain scan. The same section of the affected and healthy side were selected as the ROIs, the fat volume of the affected and healthy side on this section (cm3) is 26.1±152.4 and 22.0±169.1, respectively
![]()
图 2 下肢轴面脂肪体积分数CT图像,分别选取患侧与健侧同层面为感兴趣区,该截面患侧和健侧肢体脂肪体积分数(%)分别为:66.42±37.83和64.83±40.79
Figure 2. The axial FVF image of the lower extremity. The same section of the affected and healthy side were selected as the ROIs, the percentage FVF of the affected and healthy side on this section is 66.42±37.83 and 64.83±40.79, respectively
表 1 能谱CT阈值法测量患侧与健侧下肢体积
Table 1 The volume of the affected and healthy side by spectral CT threshold value software
分级\部位 体积/cm3 统计检验 患侧 健侧 t P 全组(n=40) 9962±2261 6762±1422 11.302 0.000 轻度(n=8) 8358±2213 7379±1862 8.126 0.000 中度(n=14) 8705±1701 6547±1314 15.460 0.000 重度(n=18) 10684±1864 6927±1376 15.487 0.000  下载: 导出CSV
下载: 导出CSV
表 2 能谱CT多物质解析算法测量患侧与健侧下肢脂肪体积分数
Table 2 The percentage FVF of the affected and healthy side by spectral CT MMD algorithm
分级\部位 脂肪体积分数/% 统计检验 患侧 健侧 t P 全组(n=40) 58.00±6.98 54.96±8.71 5.195 0.000 轻度(n=8) 57.98±5.96 55.37±7.53 2.430 0.045 中度(n=14) 58.20±9.08 54.36±10.19 3.987 0.002 重度(n=18) 57.86±5.84 55.25±8.42 2.693 0.015
下载: 导出CSV
-
[1] 常鲲, 夏松, 孙宇光, 等. 联合应用抽吸减容术与淋巴静脉吻合术治疗下肢继发性淋巴水肿的临床效果[J]. 中华外科杂志, 2017,55(4): 274−278. DOI: 10.3760/cma.j.issn.0529-5815.2017.04.008. CHANG K, XIA S, SUN Y G, et al. Liposuction combined with lymphatico-venous anastomosis for treatment of secondary lymphedema of the lower limbs: A report of 49 cases[J]. Chinese Journal of Surgery, 2017, 55(4): 274−278. DOI: 10.3760/cma.j.issn.0529-5815.2017.04.008. (in Chinese).
[2] 中国妇幼保健协会妇科肿瘤防治专业委员会. 妇科肿瘤治疗后下肢淋巴水肿专家共识[J]. 中国临床医生杂志, 2021,49(2): 149−155. DOI: 10.3969/j.issn.2095-8552.2021.02.006. Professional Committee of Gynecological Cancer Prevention and Treatment of China Maternal and Child Health Association. Expert consensus on lower limb lymphedema after treatment of gynecological tumors[J]. Chinese Journal for Clinicians, 2021, 49(2): 149−155. DOI: 10.3969/j.issn.2095-8552.2021.02.006. (in Chinese).
[3] FORTE A J, KHAN N, HUAYLLANI M T, et al. Lymphaticovenous anastomosis for lower extremity lymphedema: A systematic review[J]. Indian Journal of Plastic Surgery, 2020, 53(1): 17−24. DOI: 10.1055/s-0040-1709372.
[4] Executive Committee. The diagnosis and treatment of peripheral lymphedema: 2016 consensus document of the international society of lymphology[J]. Lymphology, 2016, 49(4): 170−184.
[5] MACLELLAN R A, GREENE A K. Lymphedema[J]. Seminars in Pediatric Surgery, 2014, 23(4): 191−197. DOI: 10.1053/j.sempedsurg.2014.07.004.
[6] 信建峰, 孙宇光, 夏松, 等. 淋巴脂肪抽吸减容术在下肢原发性淋巴水肿中的治疗及分析[J]. 中华整形外科杂志, 2019,35(2): 142−147. DOI: 10.3760/cma.j.issn.1009-4598.2019.02.009. XIN J F, SUN Y G, XIA S, et al. Application of liposuction in treating the primary end-stage lymphedema of lower extremities[J]. Chinese Journal of Plastic Surgery, 2019, 35(2): 142−147. DOI: 10.3760/cma.j.issn.1009-4598.2019.02.009. (in Chinese).
[7] HYODO T, YADA N, HORI M, et al. Multimaterial decomposition algorithm for the quantification of liver fat content by using fast-kilovolt-peak switching dual-energy CT: Clinical evaluation[J]. Radiology, 2017, 283(1): 108−118. DOI: 10.1148/radiol.2017160130.
[8] YAMADA K, SHINAOKA A, KIMATA Y. Three-dimensional imaging of lymphatic system in lymphedema legs using interstitial computed tomography-lymphography[J]. Acta Medica Okayama, 2017, 71(2): 171−177. DOI: 10.18926/AMO/54986.
[9] OLSZEWSKI W L. Lymphovenous microsurgical shunts in treatment of lymphedema of lower limbs: A 45-year experience of one surgeon/one center[J]. European Journal of Vascular and Endovascular Surgery, 2013, 45(3): 282−290. DOI: 10.1016/j.ejvs.2012.11.025.
[10] DELTOMBE T, JAMART J, RECLOUX S, et al. Reliability and limits of agreement of circumferential, water displacement, and optoelectronic volumetry in the measurement of upper limb lymphedema[J]. Lymphology, 2007, 40(1): 26−34.
[11] TSUKADA A, UCHIDA K, AIKAWA J, et al. Unilateral-dominant reduction in muscle volume in female knee osteoarthritis patients: Computed tomography-based analysis of bilateral sides[J]. Journal of Orthopaedic Surgery and Research, 2020, 15(1): 543. DOI: 10.1186/s13018-020-02074-x.
[12] 杨献峰, 杨尚文, 胡安宁, 等. 基于CT值阈值法测量骨骼肌体积[J]. 中国医学计算机成像杂志, 2017,23(3): 287−291. DOI: 10.3969/j.issn.1006-5741.2017.03.019. YANG X F, YANG S W, HU A N, et al. Measurement of skeletal muscle volume based on CT value threshold method[J]. Chinese Journal of Medical Computer Imaging, 2017, 23(3): 287−291. DOI: 10.3969/j.issn.1006-5741.2017.03.019. (in Chinese).
[13] 张国来, 包强, 陈光辉, 等. CT阈值法测量乳突气房体积与面神经管垂直段位置的相关性[J]. 中国医学影像学杂志, 2016,24(3): 175−178. DOI: 10.3969/j.issn.1005-5185.2016.03.004. ZHANG G L, BAO Q, CHEN G H, et al. Correlation between the volume of the mastoid air chamber and the position of the vertical segment of the facial nerve canal measured by the CT threshold method[J]. Chinese Journal of Medical Imaging, 2016, 24(3): 175−178. DOI: 10.3969/j.issn.1005-5185.2016.03.004. (in Chinese).
[14] 郭佳, 沈文彬, 信建峰, 等. CT评价继发性下肢淋巴水肿分级的价值研究[J]. CT理论与应用研究, 2022,31(2): 237−244. DOI: 10.15953/j.ctta.2021.039. GUO J, SHEN W B, XIN J F, et al. CT imaging in secondary lower extremity lymphedema: A prospective study[J]. CT Theory and Applications, 2022, 31(2): 237−244. DOI: 10.15953/j.ctta.2021.039. (in Chinese).
[15] CUCCHI F, ROSSMEISLOVA L, SIMONSEN L, et al. A vicious circle in chronic lymphedema pathophysiology? An adipocentric view[J]. Obesity Reviews, 2017, 18(10): 1159−1169. DOI: 10.1111/obr.12565.
[16] CAO Q, YAN C, HAN X, et al. Quantitative evaluation of nonalcoholic fatty liver in rat by material decomposition techniques using rapid-switching dual energy CT[J]. Academic Radiology, 2021, S1076-6332(21): 00365−2. DOI: 10.1016/j.acra.2021.07.027.
[17] MENDONCA P R, LAMB P, SAHANI D V, et al. A flexible method for multi-material decomposition of dual-energy CT images[J]. IEEE IEEE Transactions on Medical Imaging, 2014, 33(1): 99−116. DOI: 10.1109/TMI.2013.2281719.
[18] WU X, HE P, LONG Z, et al. Multi-material decomposition of spectral CT images via fully convolutional densenets[J]. Journal of X-ray Science and Technology, 2019, 27(3): 461−471. DOI: 10.3233/XST-190500.
-
期刊类型引用(1)
1. 陈宗桂,肖瑶,钟志明,唐琦,曹湘玉,黄民江. 能谱CT单能量成像联合去金属伪影算法可减少颅内动脉瘤栓塞术后伪影. 分子影像学杂志. 2025(02): 229-234 .  百度学术
百度学术
其他类型引用(0)
计量
- 文章访问数: 270
- HTML全文浏览量: 87
- PDF下载量: 16
- 被引次数: 1


