
Correlation between Carotid Atherosclerotic Plaques and Acute Ischemic Stroke
-
摘要: 目的:运用颈动脉CTA分析颈动脉粥样硬化斑块,探讨斑块性质及部分因素与急性缺血性脑卒中的相关性,从而为急性缺血性脑卒中的预防和治疗提供参考和依据。方法:回顾性分析行颈动脉CTA检查、且在颈动脉CTA检查前或后一周内行磁共振DWI检查的患者,根据磁共振DWI判断有无前循环急性缺血性脑卒中,将患者分为急性缺血性脑卒中组(95例)和非急性缺血性脑卒中组(102例);对两组患者的临床资料、实验室资料和CTA显示的颈动脉斑块性质、斑块表面形态进行分析,比较两组之间有无统计学差异,对P<0.05的指标纳入急性缺血性脑卒中发生的多因素Logistic回归分析。结果:两组间在年龄、高血压病史、TC、TG、HDL、HCY、CysC、HbA1c指标中差异有统计学意义;两组间在斑块性质及斑块表面形态间差异有统计学意义,在颈动脉管腔狭窄程度间差异无统计学意义;多因素回归分析提示年龄≥65岁、高血压、TC、HDL、HCY及脂质斑块是急性缺血性脑卒中发生的危险因素。结论:颈动脉粥样硬化与急性缺血性脑卒中发生相关,脂质斑块是急性缺血性脑卒中发生的危险因素;颈动脉CTA可以对斑块性质进行判断,结合部分实验室指标,可以为急性缺血性脑卒中的防治提供参考和依据。Abstract: Objective: Carotid artery computed tomography angiography (CTA) was used to analyze carotid atherosclerotic plaques and explore the correlation of plaque properties and other factors with the occurrence of acute ischemic stroke. The aim was to provide a basis for the prevention and treatment of acute ischemic stroke. Methods: Patients who underwent carotid artery CTA and magnetic resonance diffusion-weighted imaging (DWI) within 2 weeks before or after carotid artery CTA were analyzed retrospectively. Based on magnetic resonance DWI data, these patients were divided into the acute ischemic stroke group (n=95) and non-acute ischemic stroke group (n=102). The clinical data, laboratory data, and nature and surface morphology of the carotid plaques on CTA were compared between the two groups. Variables with P<0.05 were included in a multivariate logistic regression analysis to determine the risk factors of acute ischemic stroke. Results: Age, hypertension history, and levels of total cholesterol (TC), triglyceride (TG), high-density lipoprotein (HDL), homocysteine (Hcy), cystatin C (Cys-C), and glycated hemoglobin (HbA1c) differed significantly between the two groups. Multivariate regression analysis revealed that age ≥65 years (odds ratio [OR]: 4.95), hypertension (OR: 9.91), high TC (OR: 2.78), high Hcy (OR: 3.07), high HbA1c (OR: 4.60), and lipid plaque (OR: 4.89) were the independent risk factors for acute ischemic stroke. A high HDL level (OR of 0.13) was identified as a protective factor for the development of acute ischemic stroke. Conclusion: Carotid atherosclerosis is related to acute ischemic stroke occurrence. Furthermore, the presence of lipid plaques is a risk factor for acute ischemic stroke. Combined with some laboratory indicators, carotid artery CTA can judge the nature of carotid plaques and provide a basis for the prevention and treatment of acute ischemic stroke.
-
Keywords:
- carotid CTA /
- carotid plaque /
- acute ischemic stroke
-
肺癌是全世界最常见的恶性肿瘤之一,在我国肺癌发病率和死亡率均居于首位[1],严重危害我国国民的健康和生命,给家庭和社会带来巨大经济负担。提高肺癌生存率最有效的方法是二级预防,即早发现、早诊断和早治疗,筛查是早期发现肺癌和癌前病变的重要途径[2]。2011年,美国国家肺癌检测试验(National Lung Screening Trial,NLST)首次提出低剂量螺旋计算机断层扫描(low-dose computed tomography,LDCT)检测在高危人群中的应用可显著降低肺癌的死亡率[3],当LDCT上出现异常时可以进一步选择常规CT、高分辨率CT及靶扫描方式对病灶进行甄别。
肺癌的早期常表现为肺部结节病灶,然而肺结节的成因有多种多样,同一对象的CT图像上常有多个肺结节,且表现不一,这对影像诊断医师的筛检和鉴别能力提出了较高的要求。人工智能(artificial intelligence,AI)辅助诊断系统的加入担负了大量枯燥重复的工作,大大提升了影像医师的阅片速度,与医师诊断相比,其具有不受医师的主观性、经验差异及疲劳等人为因素影响的优越性[4]。
鉴于此,本研究回顾性分析113例入组病例的筛检情况来比较AI软件和影像医师的阅片能力,旨在探讨AI辅助诊断系统在肺结节的检测及良恶性判断中的应用价值。
1. 资料与方法
1.1 病例资料
本研究为回顾性研究,选择内蒙古自治区人民医院2022年3月至2023年3月行胸部CT检查,并跟踪随访行CT引导下穿刺活检术或外科手术明确肺结节病理结果的患者作为研究对象。共收集患者113例,其中:男性68例,女性45例。年龄38~77岁,中位约65.20岁。
纳入标准:①在我院至少行 1次胸部CT扫描,并且CT检查前未行干预治疗措施;②符合《肺结节诊治中国专家共识(2018年版)》[5]中肺结节诊断标准且图像质量良好;③涉及结节良恶性判断部分的肺结节均有明确病理诊断。排除标准:①病灶直径>3 cm;②其他部位恶性肿瘤所致转移瘤;③患者患有严重的基础性疾病,无法进行病理诊断;④患者资料信息不完整或失访。
1.2 检查技术
(1)扫描设备:GE LightSpeed750 64排CT;GE LightSpeedVCT 64排CT;西门子Definition Flash 双64排CT;东芝 TSX-301A 320排CT。
(2)扫描范围:扫描前由专人对每位受检者进行呼吸训练,所有受检者均取仰卧位、双臂上举、头先进、深吸气末屏气扫描,扫描范围由肺尖到后肋膈角(包括全部肺)。
(3)扫描参数:管电压120 kV,自动管电流。层间距0.625 mm,层厚1.25 mm,采用标准算法及高分辨算法进行重建并且将扫描原始数据上传至工作站。肺窗参数设置为:肺窗窗宽1500~2000 HU、窗位 -600~-450 HU;纵隔窗宽250~350 HU、窗位30~50 HU。
1.3 图像分析
影像医师阅片。一名住院医师在ImageFileName.dcm工作站上参阅原始图像(1.25 mm层厚)及重建图像(5 mm层厚),阅片过程中常规参考多平面重建技术多角度分析图像,阅片结果由一名临床经验丰富的主治医师审核后发布,以二者报告一致视为有效,否则与另一名主治医师进行探讨后得出最终结论。
AI软件阅片。应用AI辅助分析软件InferRead CTR12.2,由北京推想医疗科技股份有限公司提供。将原始图像导入系统之后,软件自动识别并标记结节病灶,提供结节位置、大小、性质等信息,同时模型根据这些信息计算恶性概率预测值,当恶性概率预测值>70% 时判断为恶性结节。
真阳性结节判断标准。结合两名医师及AI软件图像分析结果,参考多平面重建、三维重建等图像,共同确定肺结节存在,以二者报告一致视为有效。
1.4 数据处理
采用SPSS 25.0软件分析数据,计数资料以(n(%))表示,比较采用卡方检验或Fisher精确概率法,计量资料以
$ \left(\overline{x}\pm s\right) $ 表示。使用Kappa值评价AI、影像医师与病理结果的一致性,0.0~0.20极低的一致性、0.21~0.40一般的一致性、0.41~0.60 中等的一致性、0.61~0.80高度的一致性和0.81~1几乎完全一致。以P<0.01为差异有统计学意义。2. 结果
2.1 总体检出情况
113名患者中,AI软件检出1337个结节,医师检出774个结节,经验证存在1079个真阳性结节。AI软件对于真阳性结节的检出率(98.98%)高于医师(71.27%),漏检率(1.02%)较医师(28.27%)低,误检率(23.91%)较医师(0.46%)高,以上差异均具有统计学意义(表1)。
表 1 AI软件及医师对结节的总体检出情况Table 1. AI software and radiologists’ overall detection of nodules组别 AI 医师 $\chi^2 $ P 共检出(%) 1337(123.91) 774(71.73) 真阳性结节(%) 1068(98.98) 769(71.27) 假阴性结节(%) 11(1.02) 305(28.27) 398.766 <0.001 假阳性结节(%) 258(23.91) 5(0.46) 128.199 <0.001 2.2 AI软件及医师对不同直径真阳性结节的检出价值
AI软件对直径<5 mm及5~10 mm真阳性结节的检出率(98.69%,100.00%)均高于医师(60.59%,80.25%),差异具有统计学意义;对于直径>10 mm真阳性结节的检出率(98.08%)稍高于医师(94.87%),但差异不具有统计意义(表2)。
表 2 AI软件及医师对不同直径真阳性结节的检出价值Table 2. The value of AI software and radiologists in detecting true positive nodules of different diameters组别 真阳性 AI 医师 $\chi^2 $ P <5(%) 609 601(98.69) 369(60.59) 272.521 <0.001 5~10(%) 314 314(100.00) 252(80.25) 68.792 <0.001 >10(%) 156 153(98.08) 148(94.87) 2.356 0.125 2.3 AI软件及医师对不同性质真阳性结节的检出价值
AI软件对磨玻璃、实性、混合磨玻璃及钙化结节的检出率(98.47%,98.79%,100.00%,100.00%)均高于医师(75.52%,68.02%,72.73%,84.66%),差异具有统计学意义(表3)。
表 3 AI软件及医师对不同性质真阳性结节的检出价值Table 3. The value of AI software and radiologists in detecting true positive nodules of different nature组别 真阳性 AI 医师 $\chi^2 $ P 磨玻璃(%) 131 129(98.47) 95(72.52) 35.582 <0.001 实性(%) 741 732(98.79) 504(68.02) 253.375 <0.001 混合磨玻璃(%) 44 44(100.00) 32(72.73) 13.895 <0.001 钙化(%) 163 163(100.00) 138(84.66) 27.076 <0.001 2.4 AI软件及医师对结节良恶性的判断价值
113名患者中共有115个结节经病理检查确诊,其中98例在我院行干预手术或CT引导下穿刺活检取得病理,17例经随访外院诊疗情况确定。
115个结节的大小和性质见表4,AI软件及医师对结节良恶性的判断价值(表5和表6),两种阅片方法对结节良恶性判断的效能比较(表7)。
表 4 115个结节的大小和性质Table 4. Size and nature of the 115 nodules组别 磨玻璃结节个数 实性结节个数 混合磨玻璃结节个数 钙化结节个数 总和 <5 mm 4 9 3 0 16 5~10 mm 6 24 6 1 37 >10 mm 6 41 12 3 62 总和 16 74 21 4 115 表 5 AI软件对结节良恶性的判断价值Table 5. The value of AI software in judging benign and malignant nodulesAI 病理 总计 恶性 良性 恶性 74 12 86 良性 5 24 29 总计 79 36 115 表 6 医师对结节良恶性的判断价值Table 6. The value of radiologists in judging benign and malignant nodulesAI 病理 总计 恶性 良性 恶性 77 7 84 良性 2 29 31 总计 79 36 115 表 7 两种方法对结节良恶性判断的效能比较Table 7. Comparison of efficacy of the two methods in judging benign and malignant nodules组别 灵敏度/% 特异度/% 准确度/% AI 93.67 66.67 85.22 医师 97.47 80.56 92.17 P >0.01 >0.01 <0.01 经SPSS 25.0计算,AI的Kappa一致性是0.637,高度一致;医师的Kappa一致性是0.811,几乎完全一致(P<0.01)。
3. 讨论
本研究对比了AI及影像医师从肺结节的检出到良恶性判断的诊断全过程,真实的反映了AI在实际工作中对于高效诊断的辅助作用,同时该研究在市级三甲医院进行,得到的结果可以大致反映当地的诊疗水平及对新技术的应用程度。
研究结果显示AI软件对真阳性结节的检出率明显高于影像医师,但是误检率较高,与之前研究报道结果基本一致[6-9]。结合误检图像分析,我们考虑是其对于诊断为结节的阈值过低,常将血管、局部增厚的胸膜、肺门淋巴结、肺内索条等饱满结构误认为是肺结节;影像医师的漏检率相对较高,是由于其对于微、小结节的辨识度低,在肺组织背景较杂乱时,难以将肺结节从中检出(图1(a)~图1(c))。医师对于混合磨玻璃结节及钙化结节的检出能力与AI相差不大,但是对于磨玻璃结节和实性结节的检出能力较差,常将边缘欠清晰的磨玻璃结节及较小的实性结节漏检,因此我们应该积极参考AI软件对于不同性质结节的检出结果。
![]() 图 1 部分漏诊及误诊病例影像资料注:(a)右肺下叶血管旁结节,医师检出,AI漏检;(b)右肺下叶胸膜下实性微结节,AI检出,医师漏检;(c) 左侧局部增厚的胸膜,医师检出,AI误检为结节。(d) 右肺上叶实性结节,伴有分叶征,AI及医师均诊断为恶性,病理结果提示错构瘤;(e) 右肺下叶实性结节,形态略欠规整,周围伴有晕征,AI诊断为恶性,医师结合图像及患者痰培养、血象、查体等诊断为良性,病理结果提示肉芽肿;(f)右肺中叶实性结节,有浅分叶和毛刺征象,周围伴有点条状渗出、炎性改变,AI诊断为恶性,医师诊断为良性,病理结果提示浸润性腺癌。Figure 1. Imaging data of some missed and misdiagnosed cases
图 1 部分漏诊及误诊病例影像资料注:(a)右肺下叶血管旁结节,医师检出,AI漏检;(b)右肺下叶胸膜下实性微结节,AI检出,医师漏检;(c) 左侧局部增厚的胸膜,医师检出,AI误检为结节。(d) 右肺上叶实性结节,伴有分叶征,AI及医师均诊断为恶性,病理结果提示错构瘤;(e) 右肺下叶实性结节,形态略欠规整,周围伴有晕征,AI诊断为恶性,医师结合图像及患者痰培养、血象、查体等诊断为良性,病理结果提示肉芽肿;(f)右肺中叶实性结节,有浅分叶和毛刺征象,周围伴有点条状渗出、炎性改变,AI诊断为恶性,医师诊断为良性,病理结果提示浸润性腺癌。Figure 1. Imaging data of some missed and misdiagnosed cases另外,AI软件对于不同直径的肺结节均有很高的检出价值,尤其是在直径小于5 mm及5~10 mm的结节中检出率显著高于医师,但李欣菱等[10]研究认为,AI对较小结节(特别是<5 mm的结节)诊断的临床意义有待商榷,若完全按照AI的结果进行临床干预会增加医疗负担及造成过度治疗。对于直径大于10 mm的肺结节,医师和AI的检出率相近,二者差异不具有统计学意义,刘亚斌等[11]研究得出专业医师 CT扫描对不同直径真阳性结节检出率均低于基于AI技术CT扫描,但专业医师CT扫描对直径>10 mm真阳性结节检出率可达95.12%。提示虽然医师可能会将部分微、小结节漏检,但其对于恶性程度可能较高的直径大于10 mm结节的检出率也高,伴随着较低的误检率,医师对肺结节的检出更灵活、更有意义。
同时本研究就AI软件及医师对于肺结节良恶性的判断效能做出对比,结果显示医师对肺结节良恶性判断的灵敏度、特异度、准确度均较AI高,与既往研究结果基本一致[12-15],但灵敏度和特异度的差异不具有统计学意义,可能与样本选择偏差有关。AI软件的判断结果与病理高度一致,医师的判断结果与病理几乎完全一致。
仔细分析误诊病例(图1(d)~图1(f))后我们考虑AI是根据既定的算法来判断结节的良恶性,无法结合患者的临床信息如肿瘤标记物,特殊病原体培养结果,年龄、性别、工作经历、是否吸烟等个人史,因此得出的结论存在一定的片面性,造成误诊率的上升。影像医师判断的准确性与参加工作时间、学习进修经历和学历等有直接关系,再加上肺结节本身的多变性和复杂性,日常工作中误诊是无法彻底避免的[16]。我们应尽可能提高AI和影像医师甄别同病异影、同影异病的能力,将误诊降到最低,提出对患者更加有利的诊疗方案。
综上所述,AI软件辅助诊断对于肺结节确有较高的检出率,能大大降低漏检率,但误检率也随之上升;在肺结节良恶性鉴别中可为临床诊断提供辅助参考,但其准确性无法取代影像医师。计算机的输出结果是定量分析影像资料获得的,而医生面对的病例却是立体的、变化的。因此在将AI软件作为人工检测辅助手段、代替枯燥工作的同时,影像医师需要不断提升自己的辩证能力,充分结合患者临床信息来提高诊断的特异性,使AI软件更好地为诊断服务;且影像医师最能知道如何将来自互补成像技术的信息与临床数据相结合,这对软件的设计开发及数据库扩展至关重要。
本研究还存在局限性,这项回顾性研究的病理结果已经在临床诊断和治疗中得到确认,因此样本选择方面会存在偏差,这些偏差将在后续的前瞻性试验中得到校正;由于试验样本量较小、设备无法统一及对部分病例失访等问题。我们得到的结论还亟待在更多地区、更多医院的大样本中进一步验证。
-
![]()
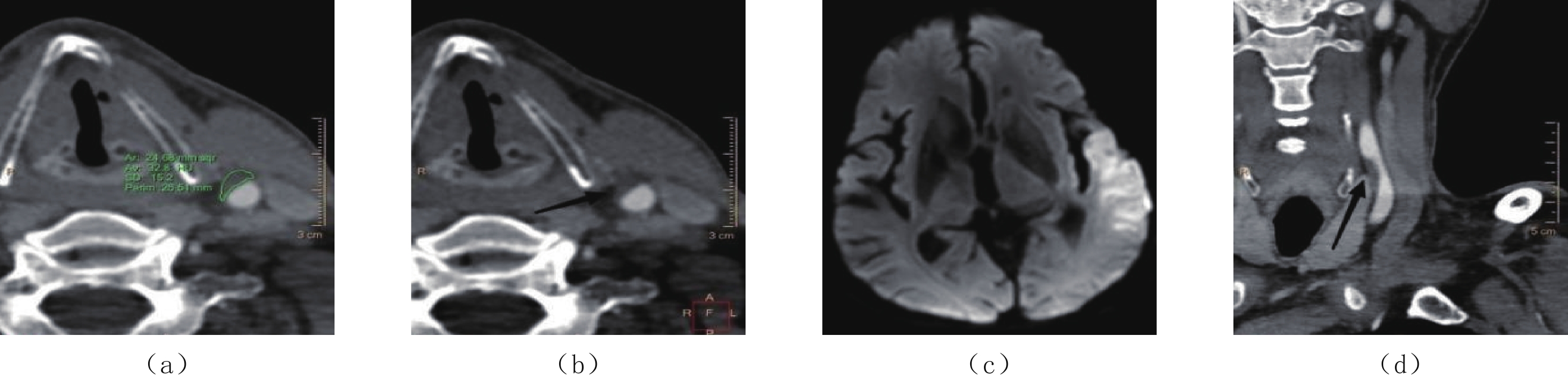
图 1 同一患者:(a)和(b)显示右侧颈总动脉脂质、溃疡斑块,(c)显示右侧基底节区及颞顶叶急性大面积脑梗塞,(d)显示右侧颈总动脉脂质斑块所致管腔中度狭窄(黑箭头所示)
Figure 1. In the same patient: (a) and (b) show lipid and ulcerative plaques in the right common carotid artery, respectively; (c) shows acute massive cerebral infarction of the right basal ganglia and temporo-parietal lobe; and (d) shows moderate stenosis of the right common carotid artery due to lipid plaques (black arrow)
![]()
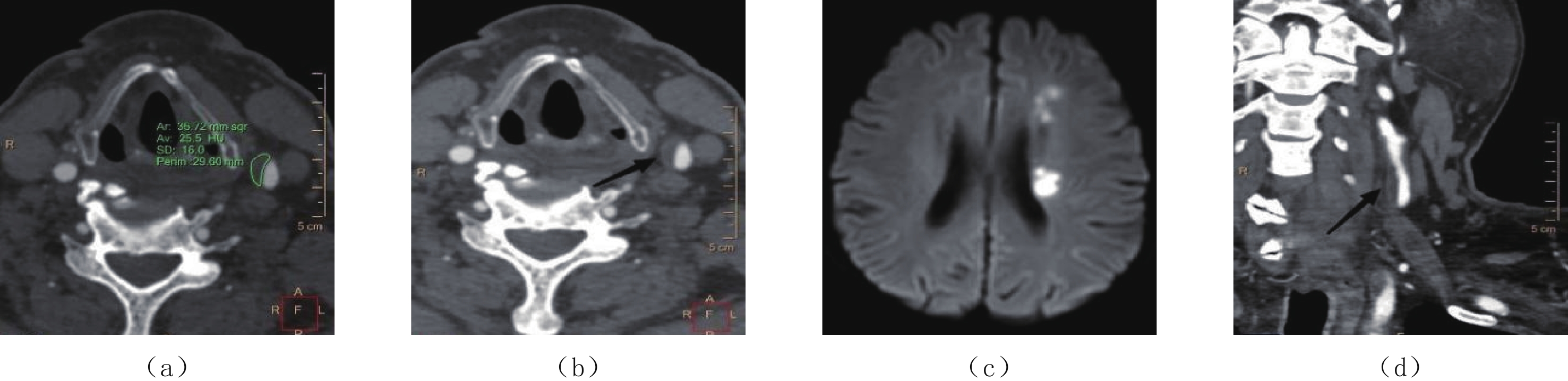
图 2 同一患者:(a)和(b)显示左侧颈总动脉脂质、不规则斑块,(c)显示左侧颞顶叶急性脑梗塞,(d)显示左侧颈总动脉脂质斑块所致管腔中度狭窄(黑箭头所示)
Figure 2. In the same patient: (a) and (b) show lipid and irregular plaques in the left common carotid artery, respectively; (c) shows acute cerebral infarction of the left temporo-parietal lobe; and (d) shows moderate stenosis of the left common carotid artery lumen due to lipid plaques (black arrow)
![]()
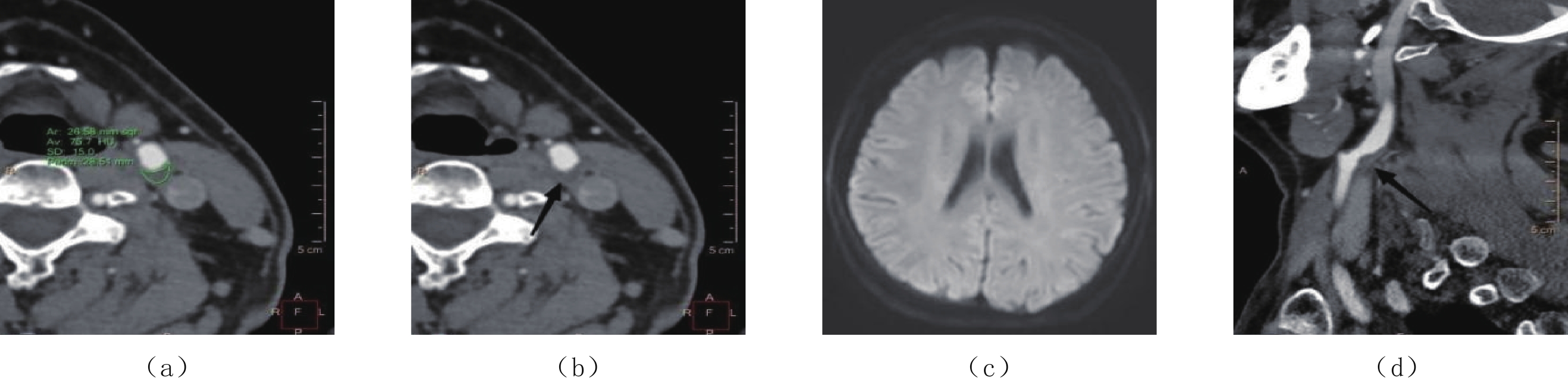
图 3 同一患者。(a)和(b)显示左侧颈总动脉脂质、光滑斑块,(c)显示左侧侧脑室旁小片状急性脑梗塞,(d)显示左侧颈总动脉脂质斑块所致管腔轻度狭窄(黑箭头所示)
Figure 3. In the same patient: (a) and (b) show lipid and smooth plaques in the left common carotid artery, respectively; (c) shows small patchy acute cerebral infarction near the left lateral ventricle; and (d) shows mild stenosis of the left common carotid artery lumen due to lipid plaques (black arrow)
![]()
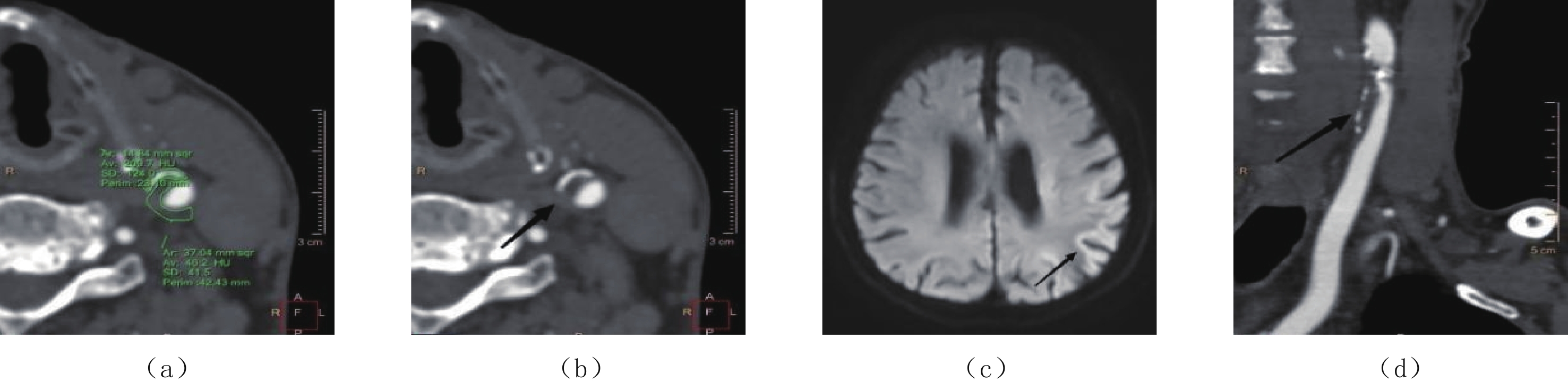
图 4 为同一患者:(a)和(b)显示左侧颈动脉分叉处纤维斑块,(c)显示该患者DWI未见明显急性脑梗塞,(d)显示左侧颈动脉分叉处纤维斑块所致管腔中度狭窄(黑箭头所示)
Figure 4. In the same patient: (a) and (b) show fibrous plaques at the left carotid bifurcation, (c) shows no significant acute cerebral infarction on DWI, and (d) shows moderate stenosis of the lumen at the left carotid bifurcation due to fibrous plaques (black arrow)
![]()
图 5 同一患者:(a)和(b)显示为左侧颈总动脉混合斑块、脂质成分为主,(c)显示左侧顶叶皮层下急性脑梗塞(黑箭头所示),(d)显示左侧颈总动脉混合斑块所致管腔中度狭窄(黑箭头所示)
Figure 5. In the same patient: (a) and (b) show mixed plaques in the left common carotid artery with a predominance of lipid components, (c) shows left parietal subcortical acute cerebral infarction (black arrow), and (d) shows moderate stenosis of the left common carotid artery lumen due to mixed plaques (black arrow)
表 1 病例组与对照组一般临床资料和实验室指标比较
Table 1 Comparison of general clinical data and laboratory indicators between the case and control groups
项目 参数 组别 统计检验 病例组(n=95)
例(%)或$\bar x \pm s$对照组(n=102)
例(%)或$\bar x \pm s$t/χ2 P 性别 男 71(81.4) 83(74.7) 1.269 0.260 女 24(18.6) 19(25.3) 年龄/岁 <50 5(5.3) 25(24.5) 32.672 <0.001 50~64 25(26.3) 25(24.5) ≥65 65(68.4) 52(51.0) 高血压* 是 66(69.5) 35(34.3) 24.339 <0.001 否 29(30.5) 67(65.7) 糖尿病 是 26(27.4) 17(16.7) 3.301 0.069 否 69(72.6) 85(83.3) 吸烟 是 14(14.7) 9(8.8) 1.668 0.197 否 81(85.3) 93(91.2) 饮酒 是 13(13.7) 7(6.9) 2.509 0.133 否 82(86.3) 95(93.1) TC/(mmol/L) 6.417±3.681 5.050±2.447 3.047 0.002 TG/(mmol/L) 2.235±1.849 1.742±1.504 2.043 0.042 HDL/(mmol/L) 1.241±0.344 1.086±0.302 3.337 0.001 LDL/(mmol/L) 2.609±0.837 2.385±0.918 1.789 0.075 HCY/(umol/L) 20.502±11.495 16.614±9.592 2.567 0.011 CysC/(mg/L) 1.143±0.251 1.073±0.245 1.978 0.049 HbA1c/% 正常 47(49.5) 81(79.4) 19.372 <0.001 不正常 48(50.5) 21(20.6)  下载: 导出CSV
下载: 导出CSV
表 2 病例组与对照组颈动脉斑块检出情况和颈动脉管腔狭窄程度比较
Table 2 Comparison of the features of carotid plaques and carotid artery stenosis
项目 参数 组别 统计检验 病例组(n=95)
例(%)或$\bar x \pm s$对照组(n=102)
例(%)或$\bar x \pm s$t/χ2 P 斑块类型* 无斑块 14a(14.7) 16a(15.7) 28.109 <0.001 钙化斑块 17a(17.9) 37a(36.3) 脂质斑块 46a(48.4) 15b(14.7) 纤维斑块 13a(13.7) 23a(22.5) 混合斑块 5a(5.3) 11a(10.8) 斑块表面形态* 无斑块 14a(14.7) 16a(15.7) 9.136 0.028 光滑斑块 34a(35.8) 56b(54.9) 不规则斑块 30a(31.6) 18b(17.6) 溃疡斑块 17a(17.9) 12a(11.8) 斑块数量/个* 4.37±3.252 3.00±2.325 3.415 0.001 管腔狭窄程度 无狭窄 15(15.8) 16(15.7) 1.153 0.679 轻度狭窄 47(49.5) 44(43.1) 中度狭窄 30(31.6) 40(39.2) 重度狭窄 3(3.2) 2(2.0) 注:* 表示P<0.05;a和b表示该因素在两组间经两两比较后存在统计学差异,字母相同则不存在统计学差异。
下载: 导出CSV
表 3 急性缺血性脑卒中发生的多因素相关Logistic回归分析
Table 3 Multivariate logistic regression analysis of the risk factors for acute ischemic stroke
因素 β $S_{\bar {\rm{x}}} $ χ2 P OR(95%CI) 年龄/岁 <50 1.000 50~65 1.294 0.946 1.871 0.171 3.647(0.571~23.281) ≥65* 1.892 0.799 5.600 0.018 6.632(1.384~31.777) 高血压* 否 1.000 是 2.341 0.507 21.309 <0.001 10.395(3.847~28.090) TC* 0.169 0.076 4.920 0.027 1.184(1.020~1.375) HDL* 1.803 0.797 5.144 0.024 6.067(1.272~28.940) HCY* 0.062 0.023 7.125 0.008 1.064(1.017~1.114) 脂质斑块* 否 1.000 是 1.328 0.494 7.217 0.007 3.773(1.432~9.938) 注:* 为P<0.05,差异有统计学意义。
下载: 导出CSV
-
[1] 彭斌, 吴波. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018,51(9): 666−682. doi: 10.3760/cma.j.issn.1006-7876.2018.09.004 PENG B, WU B. Chincese guidlines for dingnosis and treatment of acute ischemic stroke 2018[J]. Chinese Journal of Neurology, 2018, 51(9): 666−682. (in Chinese). doi: 10.3760/cma.j.issn.1006-7876.2018.09.004
[2] de WEERT T T, OUHLOUS M, MEIJERING E, et al. In vivo characterization and quantification of atherosclerotic carotid plaque components with multidetector computed tomography and histopathological correlation[J]. Arteriosclerosis, Thrombosis, and Vascular Biology, 2006, 26(10): 2366−2372. doi: 10.1161/01.ATV.0000240518.90124.57
[3] SABA L, ANZIDEI M, MARINCOLA B C, et al. Imaging of the carotid artery vulnerable plaque[J]. Cardiovasc Intervent Radiol, 2014, 37(3): 572−585. doi: 10.1007/s00270-013-0711-2
[4] RAFAILIDIS V, CHRYSSOGONIDIS I, TEGOS T, et al. Imaging of the ulcerated carotid atherosclerotic plaque: A review of the literature[J]. Insights Imaging, 2017, 8(2): 213−225. doi: 10.1007/s13244-017-0543-8
[5] WANG W, JIANG B, SUN H, et al. Prevalence, incidence, and mortality of stroke in China: Results from a nationwide population-based survey of 480687 adults[J]. Circulation, 2017, 135(8): 759−771. doi: 10.1161/CIRCULATIONAHA.116.025250
[6] CUI B, YANG D, ZHENG W, et al. Plaque enhancement in multi-cerebrovascular beds associates with acute cerebral infarction[J]. Acta Radiologica, 2021, 62(1): 102−112. doi: 10.1177/0284185120915604
[7] HYAFIL F, SCHINDLER A, SEPP D, et al. High-risk plaque features can be detected in non-stenotic carotid plaques of patients with ischaemic stroke classified as cryptogenic using combined 18F-FDG PET/MR imaging[J]. European Journal of Nuclear Medicine and Molecular Imaging, 2016, 43(2): 270−279. doi: 10.1007/s00259-015-3201-8
[8] DAI Y, QIAN Y, ZHANG M, et al. Associations between local haemodynamics and carotid intraplaque haemorrhage with different stenosis severities: A preliminary study based on MRI and CFD[J]. Journal of Clinical Neuroscience, 2019, 66: 220−225. doi: 10.1016/j.jocn.2019.05.041
[9] SAXENA A, NG E, LIM S T. Imaging modalities to diagnose carotid artery stenosis: Progress and prospect[J]. Biomedical Engineering Online, 2019, 18(1): 66. DOI: 10.1186/s12938-019-0685-7.
[10] ZHU G, LI Y, DING V, et al. Semiautomated characterization of carotid artery plaque features from computed tomography angiography to predict atherosclerotic cardiovascular disease risk score[J]. Journal of Computer Assisted Tomography, 2019, 43(3): 452−459. doi: 10.1097/RCT.0000000000000862
[11] LEE J, KIL J, KIM D W, et al. Usefulness of plaque magnetic resonance imaging in identifying high-risk carotid plaques irrespective of the degree of stenosis[J]. Journal of Cerebrovascular and Endovascular Neurosurgery, 2017, 19(4): 291−300. doi: 10.7461/jcen.2017.19.4.291
[12] COLLURA S, MORSIANI C, VACIRCA A, et al. The carotid plaque as paradigmatic case of site-specific acceleration of aging process: The microRNAs and the inflammaging contribution[J]. Ageing Research Reviews, 2020, 61: 101090. doi: 10.1016/j.arr.2020.101090
[13] PAN J, LIU J, WANG H, et al. Association of carotid atherosclerosis with lipid components in asymptomatic low-income Chinese: A population-based cross-sectional study[J]. Frontiers in Neurology, 2020, 11: 276. DOI: 10.3389/fneur.2020.00276.
[14] GARDENER H, DELLA M D, ELKIND M S, et al. Lipids and carotid plaque in the Northern Manhattan study (NOMAS)[J]. BMC Cardiovascular Disorders, 2009, 9: 55. DOI: 10.1186/1471-2261-9-55.
[15] 何爽, 江海强. 进展期脑卒中病人颈动脉斑块性质与生化指标的相关性分析[J]. 蚌埠医学院学报, 2017,42(12): 1630−1633. doi: 10.13898/j.cnki.issn.1000-2200.2017.12.018 HE S, JIANG H Q. The correlation analysis between carotid plaque nature and biochemical indicator in progressive stroke[J]. Journal Bengbu Medical College, 2017, 42(12): 1630−1633. (in Chinese). doi: 10.13898/j.cnki.issn.1000-2200.2017.12.018
[16] 刘杰, 吴东峰, 廖钦晨, 等. 颈动脉粥样硬化斑块性质与血清总同型半胱氨酸、血脂水平的相关性研究[J]. 内科, 2018,13(4): 544−546. doi: 10.16121/j.cnki.cn45-1347/r.2018.04.02 LIU J, WU D F, LIAO Q C, et al. Correlation between carotid atherosclerotic vulnerable plaque and serum total homocysteine and blood lipid levels[J]. Internal Medicine, 2018, 13(4): 544−546. (in Chinese). doi: 10.16121/j.cnki.cn45-1347/r.2018.04.02
-
期刊类型引用(4)
1. 张彩云,韩志海. 2024年版肺结节诊治中国专家共识解读. 河北医科大学学报. 2025(04): 373-378 .  百度学术
百度学术
2. 王皓,白卓杰. 基于CT的人工智能技术在肺结节诊断中的应用进展. 中国临床研究. 2025(05): 667-671+676 . 百度学术
3. 刘洋,孙旭,王涟. 国内医疗健康领域人工智能研究热点及趋势分析. 中国医药导报. 2024(25): 191-196 . 百度学术
4. 康文文,韩贺东,吕镗烽,宋勇. 精准医疗时代下肺癌筛查的难点与对策. 中华结核和呼吸杂志. 2024(12): 1211-1216 . 百度学术
其他类型引用(1)



计量
- 文章访问数: 304
- HTML全文浏览量: 94
- PDF下载量: 25
- 被引次数: 5


