
Quantitative CT Analysis of Body Composition in Maintenance Hemodialysis Patients
-
摘要: 目的:分析维持性血液透析患者的体成分信息,探讨QCT技术的应用价值。方法:选取本院维持性血液透析患者共62例,根据不同的透析时长分为3组,运用定量CT技术测定患者的骨密度值、腹部脂肪及肌肉含量,同时选取性别及年龄相匹配的健康体检人群62例进行对比分析。结果:透析组骨质疏松者占17.70%(11例),骨量减少者占30.60%(19例),而在健康对照组中,骨质疏松及骨量减少者分别占6.50%(4例)和16.10%(10例),两组间的差异具有统计学意义;透析组的腹内脂肪和皮下脂肪含量分别为(113.70±63.29)cm<sup<2</sup<、(80.65±59.67)cm<sup<2</sup<,均低于健康对照组(135.90±58.80)cm<sup<2</sup<、(122.26±54.94)cm<sup<2</sup<,透析组L3-SMA<对照组 L3-SMA,(107.00±30.70)cm<sup<2</sup<<(121.37±32.87)cm<sup<2</sup<,均具有统计学差异;在不同性别透析患者中,男性透析患者的腰椎骨密度值为(156.11±51.94)(mg/cm<sup<3</sup<),与女性(124.29±50.89)(mg/cm<sup<3</sup<)比较,差异有统计学意义;女性患者的皮下脂肪含量要高于男性,而男性和女性的腹腔内脂肪含量差异无统计学意义;透析组的骨密度值和L3-SMA变化与透析时间长短无差异。结论:维持性血液透析患者的骨质疏松症发病率高于健康人群,腹部脂肪及肌肉含量低于健康人群,定量CT对体质成分监测的准确性和敏感性较高。Abstract: This study analyzes body composition information in patients on maintenance hemodialysis and explores the application value of QCT technology. Methods: A total of 62 patients on maintenance hemodialysis were selected and divided into three groups according to different dialysis durations. The bone density value, abdominal fat, and muscle content of patients were determined by quantitative CT technology and 62 cases of the health examination population matched by sex and age were selected for comparative analysis. Results: In the dialysis group, osteoporosis accounted for 17.70% (11 cases) and bone loss accounted for 30.60% (19 cases), while in the healthy control group, osteoporosis and bone loss accounted for 6.50% (4 cases) and 16.10% (10 cases), respectively. The difference between these two groups was statistically significant. Moreover, the intra-abdominal and subcutaneous fat content in the dialysis group were (113.70±63.29)cm² and (80.65±59.67)cm², respectively, which were lower than that of the healthy control group ((135.90±58.80)cm² and (122.26±54.94)cm², respectively). Additionally, the dialysis group had a significantly lower L3-SMA (107.00±30.70)cm² than the control group (121.37±32.87)cm², and the lumbar vertebral bone density value was significantly lower in male dialysis patients (156.11±51.94)mg/cm³ than in female dialysis patients (124.29±50.89)mg/cm³. Moreover, the subcutaneous fat content was significantly higher in females than in males; however, the difference in intraperitoneal fat content between males and females was not statistically significant. Additionally, the difference between bone density values and L3-SMA changes in the dialysis group and the length of dialysis time were not statistically significant. Conclusion: The incidence of osteoporosis is higher in patients on maintenance hemodialysis than in healthy people, and the amount of abdominal fat and muscle content are lower than that in healthy people. Moreover, quantitative CT body composition monitoring has high accuracy and sensitivity.
-
Keywords:
- quantitative CT /
- hemodialysis /
- bone mineral density /
- abdominal fat
-
维持性血液透析(maintenance hemodialysis,MHD)是尿毒症患者主要的治疗方法,随着科技及各种血液净化技术的发展,有效的延长了尿毒症患者的生存期,但与此同时骨质疏松与骨折的发生率随之上升(46%~64%)[1],严重影响患者的生活质量及预后,受到国内外学者的高度重视。骨密度(bone mineral density,BMD)测量是当前骨质疏松症的首要诊断方法。
研究发现肥胖和超重与心脑血管病的发生,阻塞性睡眠呼吸暂停及某些癌症密切相关,加重了病人的死亡风险,尤其是内脏型肥胖。肥胖不仅通过高血糖、高血压以及动脉粥样硬化等其他因素,间接加重慢性肾损伤,也可以直接导致慢性肾脏病的发生。腹型肥胖也是维持性血液透析患者死亡的危险因素[2]。肌肉减少症多发生于老年人,是一种以肌肉质量和力量丢失为特点的疾病,在透析患者中,肌肉减少症能够增加患者跌倒及骨折的风险,影响预后,增加病人死亡率。因此监测维持性血液透析患者体质成分,并及时采取干预及治疗措施意义重大。
本文采用定量CT(quantitative computed tomography,QCT)技术分析维持性血液透析患者的体质成分,旨在探讨QCT的临床应用价值。
1. 资料与方法
1.1 一般资料
血透组:2013年7月至2021年11月年弋矶山医院维持性血液透析的尿毒症患者共62例,其中男33例,女29例,年龄23~84(55.0±13.1)岁,按照不同的透析时长分为3组。I组血透<2年,男9例,女10例,共19例;Ⅱ组血透2~5年,男13例,女10例,共23例;Ⅲ 组血透>5年,男11例,女9例,共20例。所有被检患者每周透析3次,每次3~4 h。肿瘤、外伤、急性感染患者;长期服用激素,免疫抑制剂,化疗药物患者;其他影响体质的相关疾病,如库欣综合征、甲状腺及甲状旁腺疾病等患者被排除在外。
对照组:同期本院62例与血液透析组年龄、性别相匹配的健康体检者,年龄21~81(54.7±12.8)岁,其中男34例,女28例。
1.2 仪器与方法
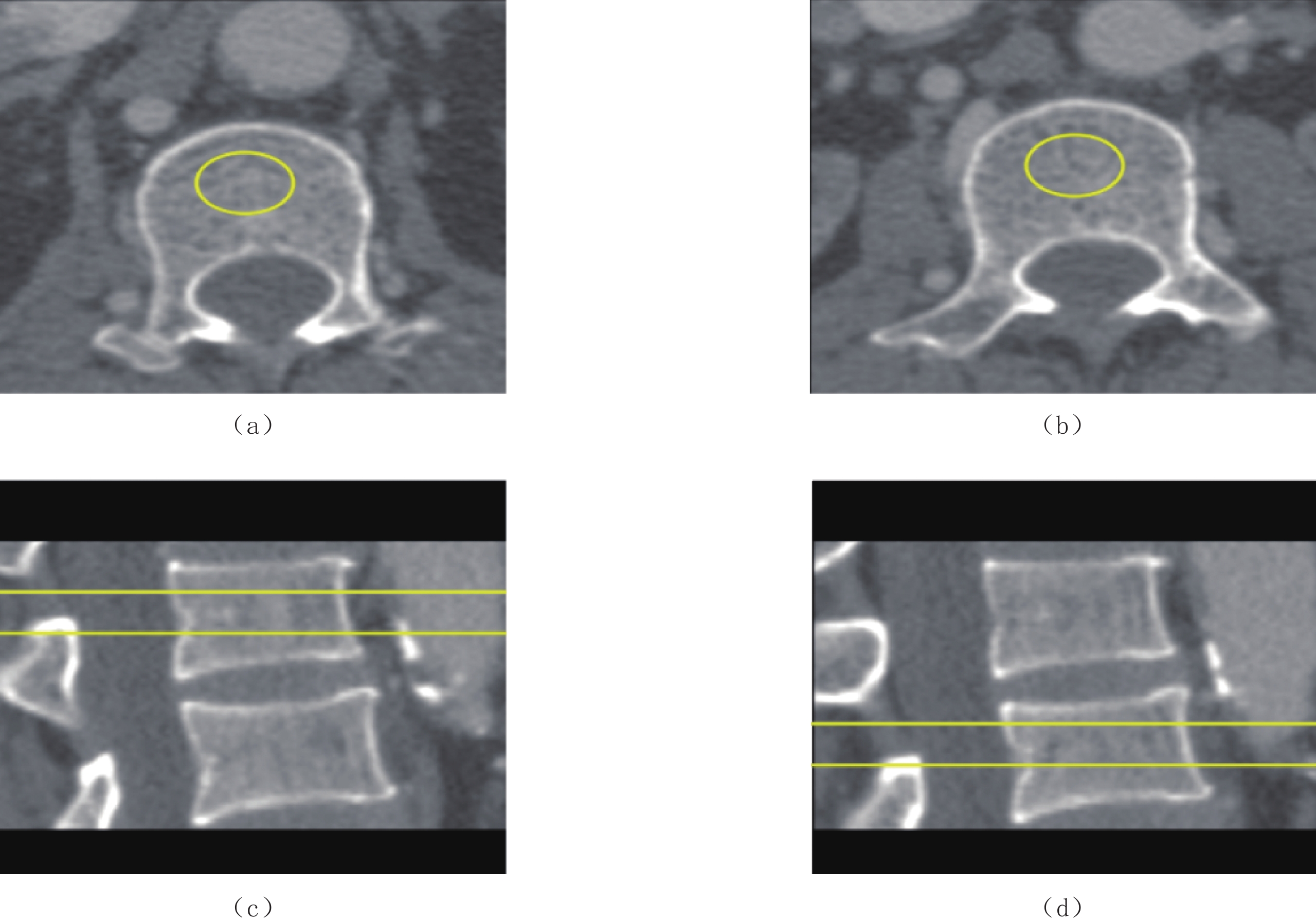
采用Philips Brilliance 64 CT机,Mindways软件公司开发研制的QCT骨密度检测软件,将所获得的CT图像传送至QCT-PRO工作站,利用软件中的“tissue composition”模块,选取腰3层面,自动得出结果(图1)。按照中国定量CT骨质疏松症诊断指南(2018)[3],采用“骨密度”模块测量腰1和腰2的椎体骨密度,测量感兴趣区(ROI)放置于椎体的中心区域,注意避开皮质骨和骨岛等,最后取其平均值(图2)。
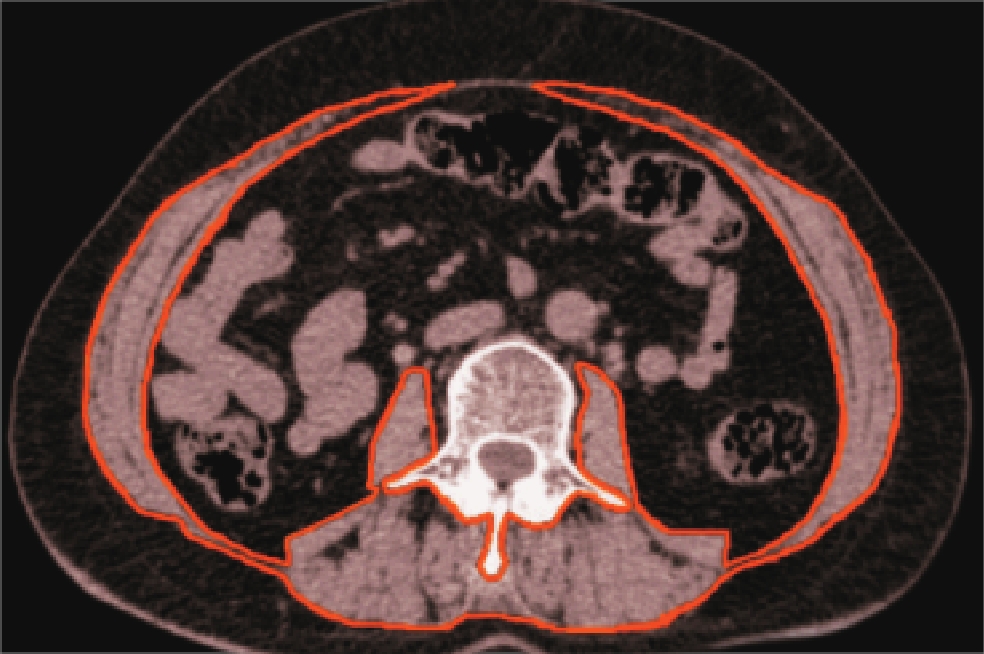
![]() 图 1 QCT测量L3中心层面腹部脂肪绿色光圈外蓝色代表皮下脂肪含量,光圈内则代表腹腔内脂肪含量。Figure 1. QCT measures abdominal fat at the center level of L3
图 1 QCT测量L3中心层面腹部脂肪绿色光圈外蓝色代表皮下脂肪含量,光圈内则代表腹腔内脂肪含量。Figure 1. QCT measures abdominal fat at the center level of L3![]() 图 2 测量L1、L2椎体松质骨骨密度值Figure 2. The measurement of the bone density values of the L1 and L2 vertebral bodies’ cancellous bone
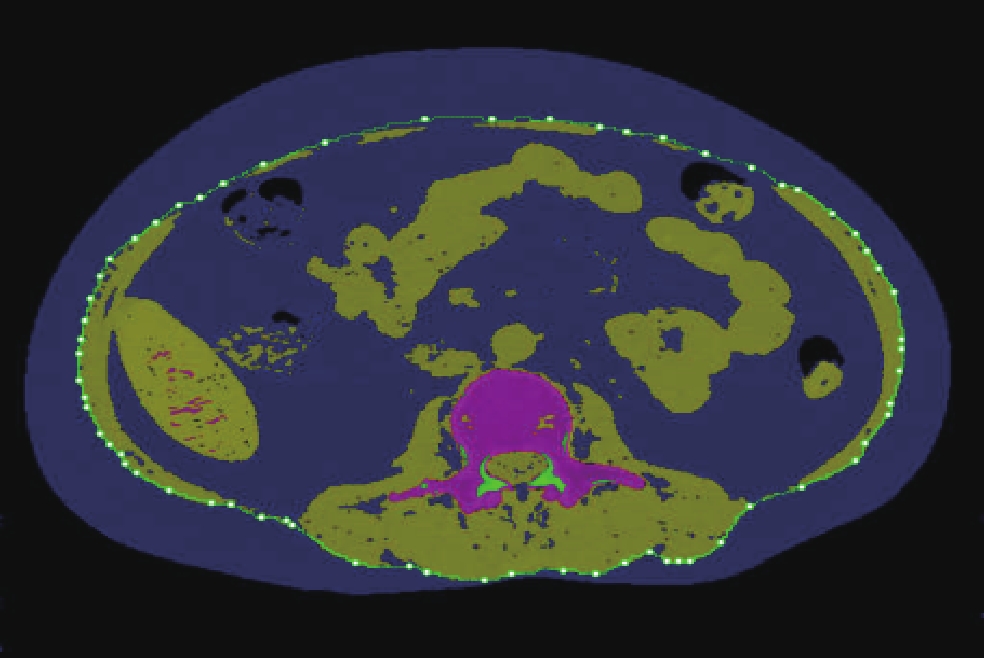
图 2 测量L1、L2椎体松质骨骨密度值Figure 2. The measurement of the bone density values of the L1 and L2 vertebral bodies’ cancellous bone与测量腹部脂肪相同,软件自动区分L3椎体中心层面脂肪和肌肉的边界。为了确保测量结果的准确性,本研究分别测量椎旁后肌群和腹肌、腰大肌肌群,最后求和得到L3水平横断面总的肌肉面积(L3-SMA)(图3和图4)。
![]() 图 3 示意图,图中勾画的彩色区域即为L3-SMAFigure 3. Schematic diagram of the L3-SMA (colored outlined area)
图 3 示意图,图中勾画的彩色区域即为L3-SMAFigure 3. Schematic diagram of the L3-SMA (colored outlined area)![]() 图 4 实测图,绿色光圈内的区域面积相加即得到L3-SMAFigure 4. In this measured diagram, the area of the region within the green aperture is added together and the L3-SMA is obtained
图 4 实测图,绿色光圈内的区域面积相加即得到L3-SMAFigure 4. In this measured diagram, the area of the region within the green aperture is added together and the L3-SMA is obtained1.3 骨质疏松症诊断标准
骨质疏松症诊断标准:BMD>120 mg/cm3为骨量正常,80~120 mg/cm3为骨量减低,<80 mg/cm3为骨质疏松[3]。
1.4 统计学分析
采用SPSS 26.0统计分析软件。计量资料以均数±标准差表示,计数资料采用卡方检验;多样本均数比较采用F检验,两样本均数比较用t检验。P<0.05为差异有统计学意义。
2. 结果
2.1 两组骨量状况比较
在透析组中,骨质疏松者占17.70%(11例),骨量减少者占30.60%(19例),而在健康对照组中,骨质疏松及骨量减少者分别占6.50%(4例)和16.10%(10例),两组间的差异具有统计学意义(表1)。
表 1 健康人群与透析患者骨量状况比较Table 1. Comparison of bone mass status between the healthy population and dialysis patients组别 骨量状况 总计 骨量正常 骨量减少 骨质疏松 对照组 48(77.40%) 10(16.10%) 4(6.5%) 62(100%) 透析组 32(51.60%) 19(30.60%) 11(17.70%) 62(100%) 2.2 两组腹部脂肪含量及L3水平横断面肌肉面积比较
透析组的腹内脂肪和皮下脂肪含量分别为(113.70±63.29)cm2、(80.65±59.67)cm2,均低于健康对照组(135.90±58.80)cm2、(122.26±54.94)cm2,差异具有统计学意义;分析两组间L3水平横断面肌肉面积得出;透析组L3-SMA<对照组L3-SMA,(107.00±30.70)cm2<(121.37±32.87)cm2,差异有统计学意义(表2)。
表 2 健康人群与透析患者腹部脂肪及L3水平横断面肌肉面积比较($\bar x \pm s $ )Table 2. Comparison of abdominal fat and L3-SMA between the healthy population and dialysis patients($\bar x \pm s $ )项目 透析组 对照组 P 腹内脂肪/cm2 113.70±63.29 135.90±58.80 <0.05 皮下脂肪/cm2 80.65±59.67 122.26±54.94 <0.05 L3水平横断面肌肉面积/cm2 107.00±30.70 121.37±32.87 <0.05 2.3 不同性别透析患者腹部脂肪和骨密度比较
在不同性别的透析患者中,我们发现男性的骨密度要高于女性的骨密度,而女性的皮下脂肪含量要高于男性,具有统计学差异;男性和女性的腹腔内脂肪含量差异无统计学意义(表3)。
表 3 不同性别血透患者骨密度及腹部脂肪比较($\bar x \pm s $ )Table 3. Comparison of bone density and abdominal fat in hemodialysis patients of different sexes ($\bar x \pm s $ )组别 骨密度/(mg/cm3) 腹内脂肪/cm2 皮下脂肪/cm2 男(n=33) 156.11±51.94 100.97±58.81 63.47±54.02 女(n=29) 124.29±50.89 128.18±66.07 100.20±60.34 P <0.05 >0.05 <0.05 2.4 不同透析时间骨密度及L3水平横断面肌肉面积比较
透析组的骨密度和L3水平横断面肌肉面积变化与透析时间长短差异无统计学意义(表4)。
表 4 透析患者骨密度及L3水平横断面肌肉面积与透析时间的变化规律($\bar x \pm s $ )Table 4. Variation of bone density, L3-SMA, and dialysis time in dialysis patients ($\bar x \pm s $ )项目 透析时间 <2年(n=19) 2~5年(n=23) >5年(n=20) 骨密度/(mg/cm3) 132.17±52.21 134.14±58.36 157.99±47.10 L3水平横断面肌肉面积/cm2 115.91±42.16 103.10±23.65 103.03±24.07 3. 讨论
骨质疏松症是指各种原因导致的骨密度下降,骨微结构被破坏,造成骨脆性增加,从而容易发生骨折的全身性骨病,是威胁中、老年人生存质量的重要疾病之一[4]。骨质疏松症的患者骨强度下降,即抵抗外力或者骨折的能力下降,75% 是由骨密度下降决定的,与双能X线吸收法(dual energy X-ray absorptiometry,DXA)相比,QCT可选择性地测定椎体骨松质骨密度且不受各种无关因素的影响,能够更准确和更早的反映骨密度值的变化情况[5]。维持性血液透析患者由于继发性甲旁亢、营养不良,内分泌紊乱等原因,常导致骨质疏松,造成骨折,且发病率较高,对患者的预后水平及生活质量造成巨大影响。
本研究结果显示MHD患者的骨质疏松和骨量减少发病率要高于正常人群,这与国内外多项研究一致。血液透析组骨质疏松及骨量减少分别为17.7% 和30.6%,而对照组的正常人群为6.5% 和16.1%;骨量正常两组分别为51.6% 和71.4%。胡耀等[5]在2012年报道,维持性血液透析患者骨质疏松患病率为25%,高于健康人群;女性血液透析患者骨密度值要低于男性患者。提示其需要更加积极地监测骨密度,及时发现骨质疏松并采取一定的干预性措施,减少骨折的发生。
肾脏作为人体中最为重要的器官之一,具有多种功能及作用,血液透析作为重要的肾脏替代治疗,虽然可以很好地改善尿毒症患者的水、电解质及酸碱平衡紊乱,但是并不能像肾移植一样完全替代肾脏的功能。在进行血液透析后,虽然患者的生存期延长了,但引起尿毒症的基础病因仍然存在,患者的残余肾功能仍然在持续下降,肾脏的合成和内分泌功能是血液透析技术无法替代的,水、电解质及酸碱失衡,透析液中较低的钙浓度等等原因,最终导致了维持性血液透析患者继发性甲状旁腺功能亢进的发生,表现为破骨细胞活跃、骨密度值下降,血液透析患者低钙高磷进一步加重,甲状旁腺激素水平持续升高,加速骨质疏松的发生[6]。
血液透析往往会出现高镁血症,加速了骨吸收,同时透析的患者需要长期使用抗凝剂治疗,对骨代谢也有负性作用,以上最终导致MHD患者骨质疏松的发生。以往多项研究显示,随着透析时间的延长,患者骨密度值越低[7-8]。本研究发现长期维持血液透析患者的骨密度改变与透析时间长短无关,分析产生此现象的原因可能与本研究样本量不足、部分患者透析龄偏短等有关。
以往人们常常以体质量指数(body mass index,BMI)作为诊断肥胖的指标,其代表着个体整体的肥胖情况,但现在人们大都认为不同的脂肪分布水平比单纯的BMI值具有更加重要的临床意义,腹型肥胖比起周围脂肪型肥胖危害性更大,与患者的心脑血管病死亡和预后有更加直接的联系。而通常所说的“腹型肥胖”、“向心性肥胖”指的就是腹腔内脂肪过多。QCT是目前公认的定量测量腹部脂肪的“金标准”[9],L1/L2~L3/4区域脂肪含量能够较好地反映全腹部的脂肪含量,其中评估全腹部脂肪含量最佳层面是L2/L3[10]。与一般人群相同,高腹腔内脂肪成为行血液透析治疗的终末期肾病(end-stage renal disease,ESRD)患者死亡的危险因素[2]。
慢性肾脏病患者往往由于体液潴留,水电解质失衡及胰岛素抵抗,体质量及肥胖程度高于正常人,而肥胖反过来又进一步加重肾脏损伤,长此以往形成恶性循环,增加患者的死亡率。本研究比较了维持性血液透析患者和健康体检者的腹部脂肪含量,得出MHD患者的腹内脂肪及皮下脂肪均小于健康体检者,差异具有统计学意义,提示维持性血液透析患者与肥胖相关的死亡风险可能较正常人低。一方面,维持性血液透析患者由于长期的治疗,往往会出现厌食,抑郁,食欲减退,造成患者营养摄入不足;另一方面,维持性血液透析治疗可以改善患者体质量,减轻病人的肥胖程度,这与丁奕等[11]关于肾脏病与肥胖关系的描述相一致。血液透析通过对尿毒症患者体内毒素的清除,患者的肾脏负荷减轻,水、电解质紊乱得到缓解,内分泌稳定,胰岛素抵抗减轻,胰岛素水平降低,降低了体脂的集聚作用,从而减轻内脏脂肪沉积[12]。也有研究认为血液透析可通过对肾脏功能的恢复作用来减轻血清总胆固醇的表达,减轻患者体脂集聚,降低患者体脂量[13]。
本研究得出的另外一条结论是女性MHD患者的皮下脂肪含量高于男性MHD患者,这和正常女性皮下脂肪较男性高一样,可能是雌激素水平差异导致的。
肌肉减少症的研究与测量一直是热点问题,定量CT由于在常规CT扫描的基础上加装了样本体模,校正了线束伪影,排除了CT值对测量造成的影响,是目前公认的测量肌肉含量的金标准[14],测量肌肉含量即准确又便捷。目前定量CT诊断肌少症缺乏较为统一的标准,但是已有研究证实第3腰椎水平横断面肌肉面积(L3-SMA)与全身肌肉质量密切相关,反映全身肌肉质量既准确又安全[15]。
本研究对比分析了维持性血液透析患者和健康体检患者的L3-SMA,得出透析组L3-SMA低于体检组。MHD患者肌肉含量比正常人少,这在以往的多项研究中已得到证实。MHD病人肌少症的发生除了与能量摄入减少、体力活动减少、各种激素减少以及肌抑素过度表达、透析中营养成分丢失等因素外,还与其体内存在的微炎症状态等其他多种因素相关[16]。相比于正常人,肌肉减少症对于维持性血液透析患者危害性更大,严重影响患者的生存质量。因此,需要及时监测肌少症的发生,早期采取一定的营养治疗及干预措施,增加肌肉含量,减少相关并发症,提高患者生存率,改善生存质量。
以往有大样本研究提出L3-SMI(L3-SMA除以身高的平方)诊断肌少症的标准为男性小于52.4 cm2/m2,女性38.5 cm2/m2[17],得到了一定的认可,但是目前仍亟待通过更加深入的研究,形成较为统一的QCT诊断标准。本研究得出不同透析时间患者的L3-SMA差异无统计学意义,可能是与样本量不足等其他相关因素有关。
定量CT技术作为一项新技术,在病人完成CT扫描后对图像进行后处理,不增加病人辐射剂量,即可得到病人的体成分信息(骨密度,腹部脂肪,肌肉含量),准确性和敏感性较高,不仅是测量体成分的金标准,而且较为便捷。QCT体成分测量具有重要的临床前景和应用价值,需要积极推广和研究。维持性血液透析患者的QCT体成分分析在于早期发现患者体成分变化,早期干预,早期治疗,改善透析患者生存质量,延长患者生存时间。
-
![]()
图 1 QCT测量L3中心层面腹部脂肪
绿色光圈外蓝色代表皮下脂肪含量,光圈内则代表腹腔内脂肪含量。
Figure 1. QCT measures abdominal fat at the center level of L3
![]()
图 2 测量L1、L2椎体松质骨骨密度值
Figure 2. The measurement of the bone density values of the L1 and L2 vertebral bodies’ cancellous bone
![]()
图 3 示意图,图中勾画的彩色区域即为L3-SMA
Figure 3. Schematic diagram of the L3-SMA (colored outlined area)
![]()
图 4 实测图,绿色光圈内的区域面积相加即得到L3-SMA
Figure 4. In this measured diagram, the area of the region within the green aperture is added together and the L3-SMA is obtained
表 1 健康人群与透析患者骨量状况比较
Table 1 Comparison of bone mass status between the healthy population and dialysis patients
组别 骨量状况 总计 骨量正常 骨量减少 骨质疏松 对照组 48(77.40%) 10(16.10%) 4(6.5%) 62(100%) 透析组 32(51.60%) 19(30.60%) 11(17.70%) 62(100%)  下载: 导出CSV
下载: 导出CSV
表 2 健康人群与透析患者腹部脂肪及L3水平横断面肌肉面积比较(
$\bar x \pm s $ )Table 2 Comparison of abdominal fat and L3-SMA between the healthy population and dialysis patients(
$\bar x \pm s $ )项目 透析组 对照组 P 腹内脂肪/cm2 113.70±63.29 135.90±58.80 <0.05 皮下脂肪/cm2 80.65±59.67 122.26±54.94 <0.05 L3水平横断面肌肉面积/cm2 107.00±30.70 121.37±32.87 <0.05
下载: 导出CSV
表 3 不同性别血透患者骨密度及腹部脂肪比较(
$\bar x \pm s $ )Table 3 Comparison of bone density and abdominal fat in hemodialysis patients of different sexes (
$\bar x \pm s $ )组别 骨密度/(mg/cm3) 腹内脂肪/cm2 皮下脂肪/cm2 男(n=33) 156.11±51.94 100.97±58.81 63.47±54.02 女(n=29) 124.29±50.89 128.18±66.07 100.20±60.34 P <0.05 >0.05 <0.05
下载: 导出CSV
表 4 透析患者骨密度及L3水平横断面肌肉面积与透析时间的变化规律(
$\bar x \pm s $ )Table 4 Variation of bone density, L3-SMA, and dialysis time in dialysis patients (
$\bar x \pm s $ )项目 透析时间 <2年(n=19) 2~5年(n=23) >5年(n=20) 骨密度/(mg/cm3) 132.17±52.21 134.14±58.36 157.99±47.10 L3水平横断面肌肉面积/cm2 115.91±42.16 103.10±23.65 103.03±24.07
下载: 导出CSV
-
[1] ZAYOUR D, DAOUK M, MEDAWAR W, et al. Predictors of bone mineral, density in patients on hemodialysis[J]. TranspIanlation Proceedings, 2004, 36(5): 1297−1301. doi: 10.1016/j.transproceed.2004.05.069
[2] WU C C, LIOU H H, SU P F, et al. Abdominal obesity is the most significant metabolic syndrome component predictive of cardiovascular events in chronic hemodialysis patients[J]. Nephrol Dial Transplant, 2011, 26: 3689−3695. doi: 10.1093/ndt/gfr057
[3] 程晓光, 王亮, 曾强, 等. 中国定量CT (QCT)骨质疏松症诊断指南(2018)[J]. 中国骨质疏松杂志, 2019,25(6): 733−737. CHENG X G, WANG L, ZENG Q, et al. The China guideline for the diagnosis criteria of oste oporosis with quantitative computed tomography (QCT) (2018)[J]. Chinese Journal of Osteoporosis, 2019, 25(6): 733−737. (in Chinese).
[4] 夏维波, 章振林, 林华, 等. 原发性骨质疏松症诊疗指南(2017)[J]. 中国骨质疏松杂志, 2019,25(3): 281−309. doi: 10.3969/j.issn.1006-7108.2019.03.001 XIA W B, ZHANG Z L, LIN H, et al. Guidelines for the diagnosis and management of primary osteoporosis (2017)[J]. Chinese Journal of Osteoporosis, 2019, 25(3): 281−309. (in Chinese). doi: 10.3969/j.issn.1006-7108.2019.03.001
[5] 胡耀, 黄朝莉, 徐秀蓉. 维持性血液透析患者骨密度测定与相关指标分析[J]. 现代临床医学, 2012,38(1): 13−14. doi: 10.3969/j.issn.1673-1557.2012.01.005 HU Y, HUANG Z L, XU X R. To analysis bone mineral density and related indicators in patients of maintaining hemodialysis[J]. Journal of Modern Clinical Medicine, 2012, 38(1): 13−14. (in Chinese). doi: 10.3969/j.issn.1673-1557.2012.01.005
[6] MOSCOVICI A, SPRAGUE S M. Osteoprosis and chronic kidney disease[J]. Seminars in Dialysis, 2007, 20(5): 423−430. doi: 10.1111/j.1525-139X.2007.00319.x
[7] 刘铁滨, 王维. 长期血液透析患者腰椎骨密度定量CT的检测及意义[J]. 实用放射学杂志, 2004,20(12): 1104−106. doi: 10.3969/j.issn.1002-1671.2004.12.014 LIU T B, WANG W. Measurement of lumbar bone mineral density with quantitative computed tomography in hemodialysis patients[J]. Journal of Practical Radiology, 2004, 20(12): 1104−106. (in Chinese). doi: 10.3969/j.issn.1002-1671.2004.12.014
[8] MIRFAKHRAEE S, SAKHAEE K, ZERWEKH J, et al. Risk factors for diminished bone mineral density among male hemodialysis patients: A cross-sectional study[J]. Arch Osteoporos, 2012, 7(1/2): 283−290. doi: 10.1007/s11657-012-0110-3
[9] SHEU Y, MARSHALL L M, HOLTON K F, et al. Abdominal body composition measured by quantitative computed tomography and risk of non-spine fractures: The osteoporotic fractures in men (MrOS) study[J]. Osteoporosis International, 2013, 24(8): 2231−2241. doi: 10.1007/s00198-013-2322-9
[10] CHENG X, ZHANG Y, WANG C, et al. The optimal anatomic sitefor a single slice to estimate the total volume of visceraladipose tissue by using the quantitative computed tomography (QCT) in Chinese population[J]. European Journal of Clinical Nutrition, 2018, 72(11): 1567−1575. doi: 10.1038/s41430-018-0122-1
[11] 丁奕, 田娜, 周晓玲, 等. 肥胖与IgA肾病患者独立肾脏风险因子的相关性分析[J]. 中华肾脏病杂志, 2017,33(5): 321−326. doi: 10.3760/cma.j.issn.1001-7097.2017.05.001 DING Y, TIAN N, ZHOU X L, et al. Correlation analysis of obesity with independent renal risk factors in patients with IgA nephropathy[J]. Chinese Journal of Nephrology, 2017, 33(5): 321−326. (in Chinese). doi: 10.3760/cma.j.issn.1001-7097.2017.05.001
[12] 刘建强, 贾冶, 许钟镐, 等. 肥胖与慢性肾脏疾病: 脂肪组织与肾脏炎症及纤维化的关系[J]. 中华肾脏病杂志, 2017, 33(12): 956-960. LIU J Q, JIA Y, XU Z H, et al. Obesity and chronic kidney disease: The relationship between adipose tissue and kidney inflammation and fibrosis[J]. Chinese Journal of Nephrology, 2017, 33(12): 956-960. (in Chinese).
[13] 罗文荣, 姚书东, 孙梅琴. 血液透析对肾病肥胖女性患者内分泌相关指标的影响[J]. 中国妇幼保健, 2021,36(14): 3195−3198. DOI: 10.19829/j.zgfybj.issn.1001-4411.2021.14.009. LUO W R, YAO S D, SUN M Q. Effect of hemodialysis on endocrine-related indicators in obese women with kidney disease[J]. Maternal and Child Health Care of China, 2021, 36(14): 3195−3198. DOI: 10.19829/j.zgfybj.issn.1001-4411.2021.14.009. (in Chinese).
[14] 晏乘曦, 唐光才, 程晓光. 肌少症的定量测量现状及研究进展[J]. 中国骨质疏松杂志, 2018,24(6): 814−819. doi: 10.3969/j.issn.1006-7108.2018.06.021 YAN C X, TANG G C, CHENG X G. State of the art of quantitative me asurement of sarcopenia[J]. Chinese Journal of Osteoporosis, 2018, 24(6): 814−819. (in Chinese). doi: 10.3969/j.issn.1006-7108.2018.06.021
[15] 耿楠, 孔明, 陈煜, 等. 第三腰椎骨骼肌指数在终末期肝病营养诊断中的应用价值[J]. 临床肝胆病杂志, 2021,37(10): 2493−2496. doi: 10.3969/j.issn.1001-5256.2021.10.050 GENG N, KONG M, CHENG Y, et al. Value of L3 skeletal muscle index in nutritional diagnosis of end-stage liver disease[J]. Journal of Clinical Hepatology, 2021, 37(10): 2493−2496. (in Chinese). doi: 10.3969/j.issn.1001-5256.2021.10.050
[16] FAHAL I H. Uraemic sareopenia: Aetiology and implications[J]. Nephml Dial Transplant, 2014, 29(9): 1655−1665. doi: 10.1093/ndt/gft070
[17] PRADO C M, LIEFFERS J R, MCCARGAR L J, et al. Prevalence andclinical implications of sarcopenic obesity in patients with solidtumours of the respiratory and gastrointestinal tracts: Apopulation-based study[J]. Lancet Oncology, 2008, 9(7): 629. doi: 10.1016/S1470-2045(08)70153-0
-
期刊类型引用(1)
1. 詹昊,陈其春,刘田田,王龙胜. 基于QCT分析维持性血液透析患者体质成分变化及骨密度的影响因素. 中国CT和MRI杂志. 2023(12): 158-160 .  百度学术
百度学术
其他类型引用(1)







计量
- 文章访问数: 354
- HTML全文浏览量: 77
- PDF下载量: 23
- 被引次数: 2


