
Imaging Features and Etiology of Acute Cerebral Infarction in Bilateral PICA Territory
-
摘要: 目的:探寻双侧小脑后下动脉(PICA)供血区急性梗死的MRI特征及病因。方法:回顾性分析首都医科大学附属北京友谊医院2019年1月至2022年1月间经临床与影像学确诊的双侧PICA供血区急性梗死患者38例及双侧小脑上动脉(SCA)供血区急性梗死患者40例,按梗死大小、有无其他后循环供血区病灶、有无前循环供血区病灶,比较两组患者MRI特征差异,分析双侧PICA供血区急性梗死累及范围及椎-基底动脉改变。结果:双侧PICA供血区急性梗死表现为一侧区域梗死伴对侧小梗死的比例明显高于双侧SCA供血区梗死(39.5% vs. 15%),而发生双侧小梗死的比例低于双侧SCA供血区梗死(44.7% vs. 72.5%),合并后循环其他供血区梗死发生率明显低于双侧SCA供血区(21% vs. 80%);双侧PICA供血区急性梗死常表现为一侧全供血区受累伴对侧PICA内侧支(mPICA)供血区受累(44.7%)或双侧mPICA供血区受累(39.5%);双侧PICA供血区急性梗死更常检出单侧椎动脉V4段或PICA局限性重度狭窄/闭塞(54.2%)。结论:双侧PICA供血区梗死主要表现为一侧全供血区受累伴对侧PICA供血区受累或双侧mPICA供血区受累,且区域性梗死常见,与解剖变异密切相关。Abstract: Objective: To investigate the MRI features and etiology of acute cerebral infarction in bilateral PICA territory. Methods: 38 patients with bilateral PICA and 40 patients with bilateral SCA diagnosed clinically and radiographically in Beijing Friendship Hospital of Capital Medical University from January 2019 to January 2022, were retrospectively analyzed. The difference of MRI features, were compared between the two groups, according to the size of the infarction, the distribution of infarcted lesions in posterior circulation or anterior circulation. The range of acute infarction in the bilateral PICA territory and the changes of vertebrobasilar artery were analyzed. Results: The proportion of the infarction model of one side regional infarction with the other side small infarct in bilateral PICA was significantly higher than that in bilateral SCA (39.5% vs. 15%), while the model of small infarction on both sides was lower than that in bilateral SCA (44.7% vs. 72.5%). The incidence of infarction in other blood supply areas of the combined posterior circulation was significantly lower than that in bilateral SCA (21% vs. 80%). The infarction models of bilateral PICA manifested as unilateral total infarct of PICA territory combined with the other unilateral infarct of mPICA territory (44.7%) or bilateral mPICA territory (39.5%). Unilateral vertebral artery V4 segment or PICA-localized severe stenosis/occlusion were more frequently detected in acute infarcts in bilateral PICA (54.2%). Conclusions: Bilateral PICA territory infarction mainly manifested as unilateral total infarct of PICA territory combined with the other unilateral or bilateral infarct of mPICA territory, and regional infarction was quite common, which was closely related to anatomical variation.
-
Keywords:
- MRI /
- cerebellar infarction /
- atherosclerosis /
- vascular variation
-
急性小脑梗死约占急性脑梗死的1.5%~20%[1],其临床症状不特异,包括头痛、眩晕、共济失调、构音障碍、恶心、呕吐等,容易漏诊或误诊。磁共振成像(magnetic resonance imaging,MRI),尤其是扩散加权成像(diffusion weighted imaging,DWI)的广泛应用,大大提高了急性小脑梗死的诊断率[2],在此基础上,临床专家开始关注急性双侧小脑梗死的特征及其病因。既往的文献报道中[3-4],研究者更多关注的是双侧小脑上动脉(superior cerebellar artery,SCA)供血区的急性梗死,并在此基础上分析急性双侧小脑梗死的发病原因。而在临床工作中,我们发现双侧小脑后下动脉供血区(posterior inferior cerebellar artery,PICA)急性脑梗死并不少见。
本研究对此类病变的MRI特征进行了回顾性分析,并与同期双侧SCA供血区急性梗死的MRI特征进行对比,探讨其发病原因,以期提高急性双侧小脑梗死的临床救治水平。
1. 资料与方法
1.1 一般资料
收集首都医科大学附属北京友谊医院2019年1月至2022年1月间,经临床和影像学确诊的双侧小脑PICA供血区急性梗死患者共38例,其中男性32例,女性6例,年龄21~89岁(中位年龄62岁);同期经临床和影像学确诊的双侧小脑SCA供血区急性梗死患者40例,其中男性32例,女性8例,年龄38~100岁(中位年龄69岁)。
本研究未纳入同时累及双侧小脑PICA+SCA供血区急性梗死患者。
1.2 影像检查
(1)78例患者均于发病72 h内接受MRI常规扫描,扫描设备包括GE Signa EXCITE HD 1.5 MR扫描仪、SIMENS Magnetom Prisma 3.0 T MR扫描仪、PHILIPS Ingenia 3.0 T MR扫描仪,序列包括横轴面T1 WI、T2 WI、FLAIR、DWI及矢状面T1 WI。25例患者同时进行了磁敏感加权成像(susceptibility weighted imaging,SWI)。
(2)15例患者接受头颅磁共振血管成像(magnetic resonance angiography,MRA)检查,37例患者接受头颈CT血管成像(CT angiography,CTA)检查,其中2例患者接受了MRA及CTA检查。
MRA成像序列:三维磁共振血管成像(3D time-of-flight magnetic resonance angiography,3D TOF-MRA),扫描范围:枕骨大孔至胼胝体顶。
CTA采用GE revolution CT或佳能Aquilion TM Vision CT扫描仪,双筒高压注射器(STELLANT,MEDRAD Inc.,USA),非离子对比剂选用碘普罗胺(370 mgI/mL,GE Inc.,USA)。扫描范围自主动脉弓至颅底。扫描方法:经肘正中静脉以5 mL/s的流率注入A筒60 mL对比剂,之后B筒追加30 mL生理盐水。选取主动脉根部为监测层面进行预扫描,当升主动脉CT值达150 HU时自动触发,3 s后启动正式扫描。扫描结束后将采集到的头颈CTA图像传至后处理工作站进行多平面重建及三维重建。
1.3 图像分析及分组
由两名神经影像医师双盲阅片,意见不一致时共同协商确定。进行以下分析:
(1)根据Amarenco's解剖图谱[5],对梗死累及部位进行确认。对双侧PICA供血区急性梗死病变按PICA外侧支(lateral branch of PICA,lPICA)供血区受累、PICA内侧支(medial branch of PICA,mPICA)供血区受累、分水岭区受累、全PICA供血区受累进行分类。
(2)按梗死大小对单支动脉供血区病灶进行分类[2],单个病灶大于1.5 cm定义为区域性梗死,单个病灶均小于1.5 cm定义为小梗死,将所有病例分为双侧区域性梗死、双侧小梗死、一侧区域性梗死+对侧小梗死。
(3)分别记录每个患者是否伴发其他后循环供血区、前循环供血区的急性梗死。
(4)基于头颈CTA或MRA,观察双侧PICA供血区梗死患者椎-基底动脉血管改变。
1.4 统计学分析
采用SPSS 23.0进行统计描述与分析。比较双侧PICA供血区及双侧SCA供血区影像特征,采用绝对值及百分比表示计数资料,两组间比较采用χ
${}^2 $ 检验。P<0.05为差异有统计学意义。2. 结果
2.1 双侧PICA供血区、双侧SCA供血区急性梗死MRI特征
按梗死大小、后循环其他部位及前循环受累情况分类,总结双侧PICA供血区、双侧SCA供血区急性梗死MRI特征(表1)。
表 1 双侧PICA供血区、双侧SCA供血区急性梗死MRI特征Table 1. MRI characteristics of bilateral PICA and SCA territory acute infarctionMRI特征 组别(例数(%)) χ2 P 双侧PICA梗死
(38例)双侧SCA梗死
(40例)双侧区域性梗死 6(15.8) 5(12.5) 0.174 0.677 一侧区域性梗死+对侧梗死 15(39.5) 6(15.0) 5.933 0.015 双侧小梗死 17(44.7) 29(72.5) 6.208 0.013 累及后循环其它部位 8(21.0) 32(80.0) 27.103 <0.001 累及前循环 2(5.2) 2(5.0) 0.003 0.958 2.2 双侧PICA供血区梗死累及范围
38例双侧PICA供血区急性梗死中,17例为一侧全供血区受累伴对侧PICA供血区受累,15例为双侧mPICA供血区受累,4例为双侧分水岭区受累,2例为一侧分水岭区伴对侧PICA供血区受累。
2.3 双侧PICA供血区、双侧SCA供血区急性梗死患者头颈CTA/MRA表现
38例双侧PICA供血区急性梗死患者,20例患者接受头颈CTA检查,6例患者接受头颅MRA检查,其中2例患者接受CTA及MRA检查。40例双侧SCA供血区急性梗死患者,17例患者接受头颈CTA检查,10例患者接受头颅MRA检查。
24例行血管检查诊断为双侧PICA供血区急性梗死患者,其中13例(54.2%)表现为单侧椎动脉V4段或PICA局限性重度狭窄/闭塞,8例(33.3%)表现为椎-基底动脉多节段或弥漫管腔狭窄、闭塞,3例(12.5%)椎-基底动脉未见管腔异常。27例行血管检查诊断为双侧SCA供血区急性梗死患者,其中8例(29.6%)表现为椎-基底动脉单一节段局限性重度狭窄,14例(51.9%)表现为椎-基底动脉多节段或弥漫管腔狭窄、闭塞,5例(18.5%)椎-基底动脉未见管腔异常。双侧PICA梗死中椎基底动脉单一节段局限性重度狭窄/闭塞的比例高于双侧SCA梗死,而椎基底动脉多处或弥漫管腔狭窄、闭塞的比例低于双侧SCA梗死,但二者均无统计学差异(表2)。
表 2 双侧PICA供血区、双侧SCA供血区急性梗死椎-基底动脉CTA/MRA表现特征Table 2. CTA/MRA features of acute infarcted vertebrobasilar artery in bilateral PICA territory and bilateral SCA territory椎-基底动脉CTA/MRA表现特征 组别(例数(%)) χ2 P 双侧PICA梗死
(24例)双侧SCA梗死
(27例)单一节段局限性重度狭窄/闭塞 13(54.2) 8(29.6) 3.158 0.076 多处或弥漫管腔狭窄、闭塞 8(33.3) 14(51.9) 1.776 0.183 未见管腔异常 3(12.5) 5(18.5) 0.348 0.555 2.4 双侧PICA供血区急性梗死患者椎-基底动脉改变与MRI特征对照
13例椎动脉V4段或PICA局限性病变患者,MRI表现为一侧区域性梗死伴对侧小梗死(图1)或双侧区域性梗死(图2);8例椎-基底动脉多处或弥漫病变患者,MRI表现为双侧小梗死(图3);3例椎-基底动脉未见管腔异常患者,MRI表现为双侧小梗死。
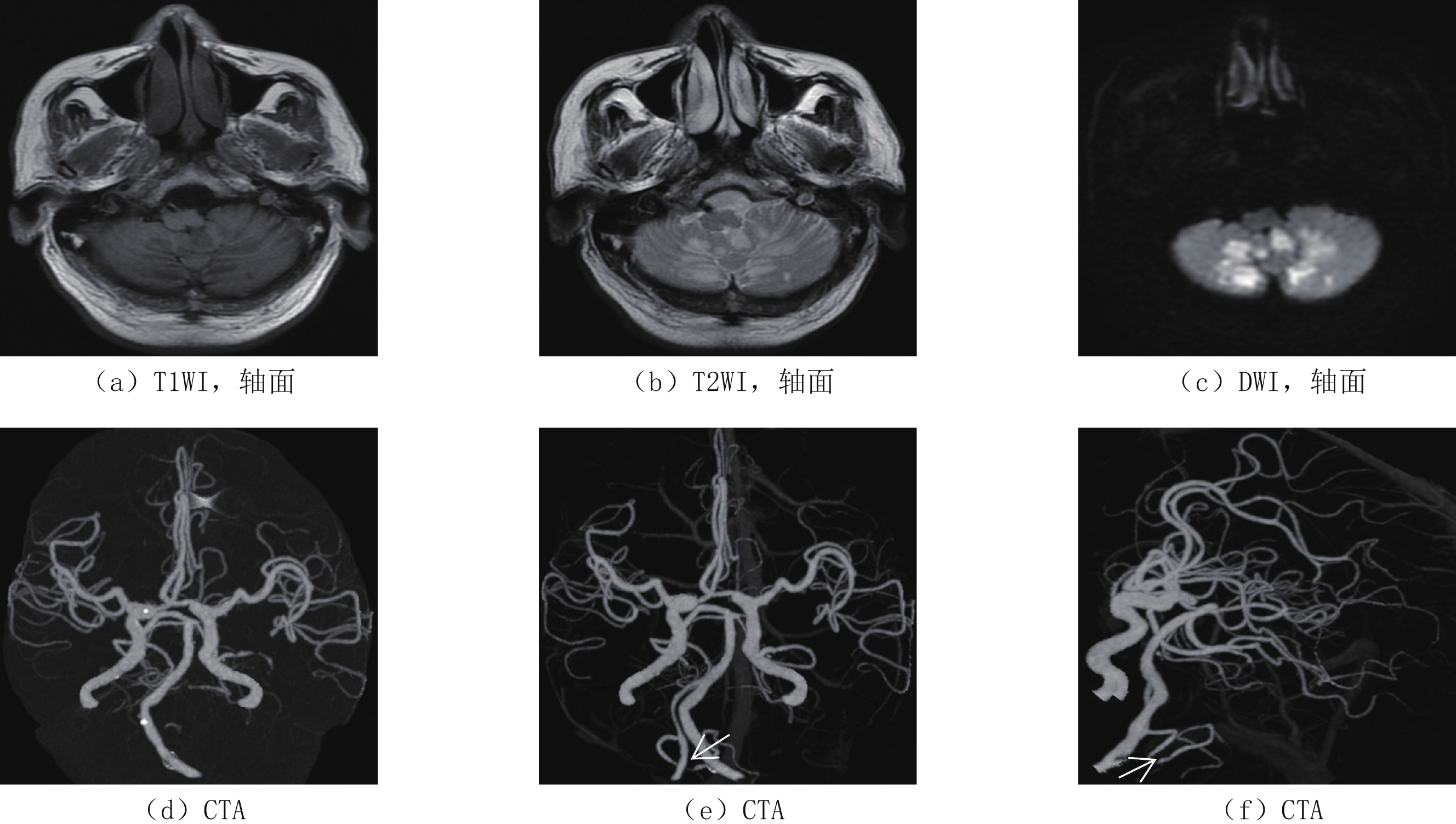
![]() 图 1 双侧PICA供血区急性梗死:一侧全供血区受累伴对侧PICA供血区受累男性,34岁,突发眩晕、行走不稳就诊。头颅MRI检查(a)T1 WI、(b)T2 WI、(c)DWI、(d)ADC,可见左侧全PICA供血区急性区域性梗死病灶及右侧mPICA供血区急性小梗死病灶;(e)CTA显示右侧PICA起源于基底动脉(白色弧形箭头),左侧PICA起始部闭塞(白色箭头);(f)SWI可见左侧PICA起始部低信号血栓形成(黑色箭头)。本例双侧小脑梗死由左侧PICA原位血栓形成引起,由于存在解剖变异,右侧mPICA供血区可能部分由左侧PICA供血,因此引起双侧小脑PICA供血区梗死。Figure 1. Acute infarction in bilateral PICA territory: Unilateral total infarct of PICA combined with the contralateral infarct of mPICA
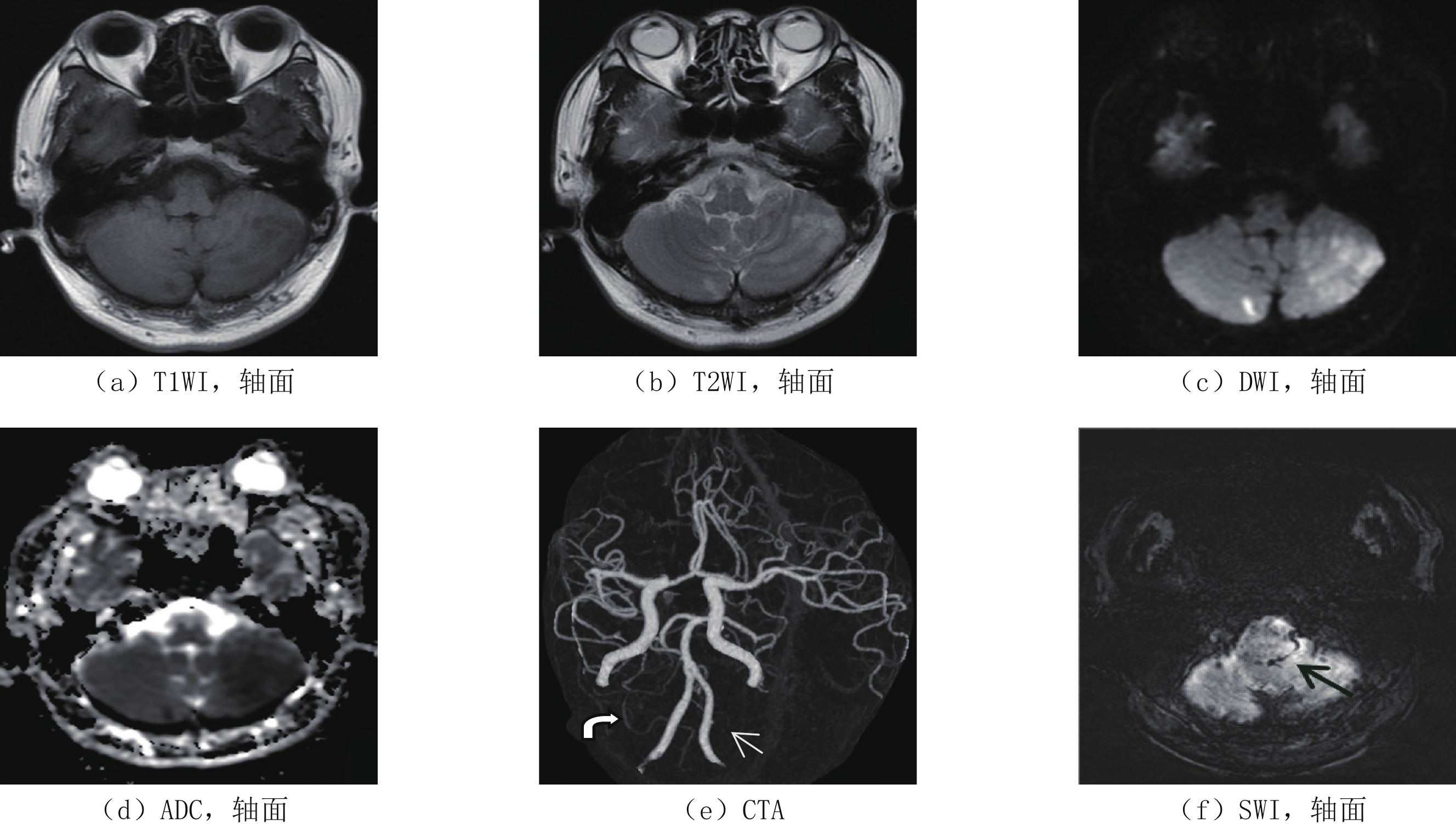
图 1 双侧PICA供血区急性梗死:一侧全供血区受累伴对侧PICA供血区受累男性,34岁,突发眩晕、行走不稳就诊。头颅MRI检查(a)T1 WI、(b)T2 WI、(c)DWI、(d)ADC,可见左侧全PICA供血区急性区域性梗死病灶及右侧mPICA供血区急性小梗死病灶;(e)CTA显示右侧PICA起源于基底动脉(白色弧形箭头),左侧PICA起始部闭塞(白色箭头);(f)SWI可见左侧PICA起始部低信号血栓形成(黑色箭头)。本例双侧小脑梗死由左侧PICA原位血栓形成引起,由于存在解剖变异,右侧mPICA供血区可能部分由左侧PICA供血,因此引起双侧小脑PICA供血区梗死。Figure 1. Acute infarction in bilateral PICA territory: Unilateral total infarct of PICA combined with the contralateral infarct of mPICA![]() 图 2 双侧PICA供血区急性梗死:双侧mPICA供血区受累男性,66岁,突发头晕就诊。头颅MRI检查(a)T1 WI、(b)T2 WI、(c)DWI,可见双侧mPICA供血区急性区域性梗死病灶,(d)头颅CTA右侧椎动脉V4段及双侧PICA均未见显示;该患者四年前头颅CTA(e)和(f)可见左侧PICA未发育,右侧PICA供应双侧小脑半球并可见局限性重度狭窄(白色箭头),本次右侧椎动脉及PICA闭塞引起双侧小脑半球急性梗死。Figure 2. Acute infarction in bilateral PICA territory: Bilateral mPICA involved
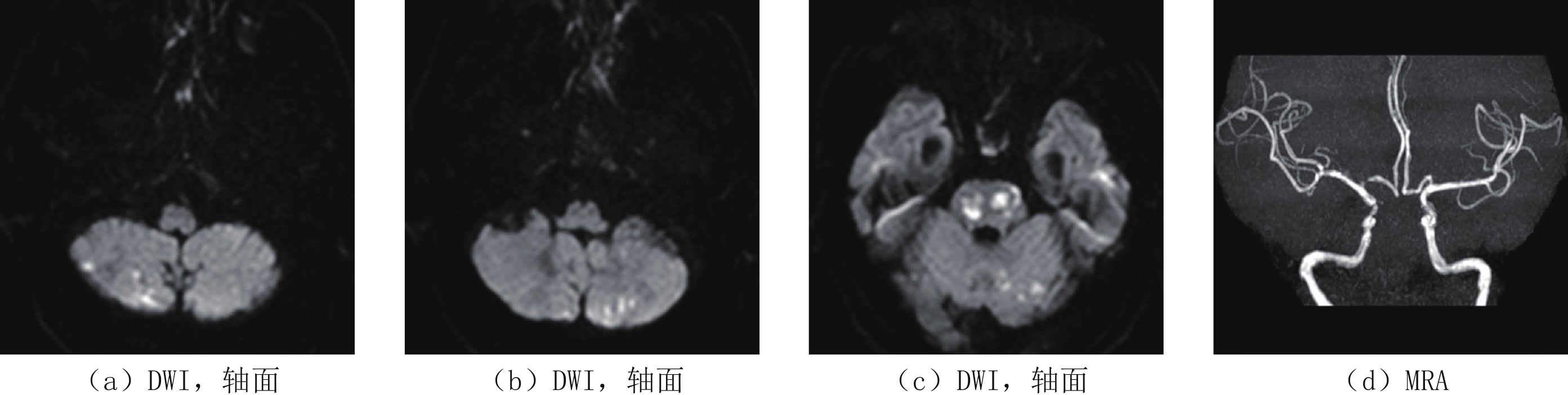
图 2 双侧PICA供血区急性梗死:双侧mPICA供血区受累男性,66岁,突发头晕就诊。头颅MRI检查(a)T1 WI、(b)T2 WI、(c)DWI,可见双侧mPICA供血区急性区域性梗死病灶,(d)头颅CTA右侧椎动脉V4段及双侧PICA均未见显示;该患者四年前头颅CTA(e)和(f)可见左侧PICA未发育,右侧PICA供应双侧小脑半球并可见局限性重度狭窄(白色箭头),本次右侧椎动脉及PICA闭塞引起双侧小脑半球急性梗死。Figure 2. Acute infarction in bilateral PICA territory: Bilateral mPICA involved![]() 图 3 双侧PICA供血区急性小梗死灶伴后循环其它供血区梗死男性,62岁,意识障碍。头颅MRI检查DWI示双侧PICA供血区(a)和(b)及左侧SCA供血区、桥脑(c)多发小梗死灶,TOF-MRA双侧椎动脉颅内段、基底动脉均未显示,提示可能为椎-基底动脉弥漫病变所致动脉-动脉栓塞。Figure 3. Acute small infarcts in bilateral PICA combined with other areas of the posterior circulation
图 3 双侧PICA供血区急性小梗死灶伴后循环其它供血区梗死男性,62岁,意识障碍。头颅MRI检查DWI示双侧PICA供血区(a)和(b)及左侧SCA供血区、桥脑(c)多发小梗死灶,TOF-MRA双侧椎动脉颅内段、基底动脉均未显示,提示可能为椎-基底动脉弥漫病变所致动脉-动脉栓塞。Figure 3. Acute small infarcts in bilateral PICA combined with other areas of the posterior circulation3. 讨论
在急性小脑梗死中,双侧小脑梗死约占20%~30%,与单侧小脑梗死比较,其临床症状更重、预后更差[6]。在发病机制上,既往研究认为,单侧小脑梗死多见于PICA供血区,多为原位动脉粥样硬化引起;而双侧小脑梗死多见于SCA供血区,且常合并小脑以外的急性梗死病灶,病因多为上一级动脉粥样硬化引起动脉-动脉栓塞或心源性栓塞。
需要注意的是,既往研究中,虽然双侧SCA供血区受累更多见,但双侧PICA供血区的受累仅略低于双侧SCA供血区[3-4],但在发病原因的探讨中并未对不同供血区受累进行独立分析,有一定的局限性。
在本组病例中,同时间段急性双侧小脑梗死中,双侧PICA供血区受累与双侧SCA供血区受累病例数量接近,而不同供血区受累的双侧小脑梗死影像特征并不相同。急性双侧PICA供血区梗死中,区域性梗死的发生率明显高于双侧SCA供血区梗死,而合并小脑以外病灶的发生率明显低于双侧SCA供血区梗死。不同的影像特征提示:与急性双侧SCA供血区梗死相比,急性双侧PICA供血区梗死有着不同的发病机制。
如前所述,双侧SCA供血区梗死病因多为动脉-动脉栓塞或心源性栓塞,因此小梗死灶的发生率更高,且更容易合并小脑以外的梗死灶;而双侧PICA供血区梗死中区域性梗死更为常见,头颈CTA/MRA分析结果表明双侧PICA供血区梗死患者多数由单侧椎动脉V4段或PICA局限性病变引起,提示其病因多为原位动脉粥样硬化引起、更容易发生区域性梗死[7]。
原位动脉粥样硬化引起双侧PICA供血区梗死的原因主要与PICA变异相关。小脑供血动脉中,PICA变异最为常见,包括几种类型[8-12]:①单侧优势型 PICA,优势侧动脉供应双侧小脑内侧区域;②双侧 PICA共干或分别起源于一侧椎动脉;③双侧 PICA起源于基底动脉;④双侧 PICA缺如,相应区域由小脑前下动脉供血。其中,单侧优势型PICA更为常见。本组中双侧PICA供血区梗死主要表现为一侧全供血区受累伴对侧mPICA供血区受累或双侧mPICA供血区受累,且区域性梗死常见,我们认为主要原因是优势侧PICA或起源椎动脉发生局限性动脉粥样硬化造成管腔狭窄或原位血栓形成,从而引起相应供血区梗死。
本组中双侧PICA供血区梗死还可表现为双侧小梗死、合并后循环其它部位梗死或前循环梗死,我们分析除了解剖变异因素,双侧PICA供血区梗死还可能有:①一侧大面积 PICA供血区梗死引起占位效应,压迫对侧mPICA分支血管引起相应供血区梗死;②血流动力学变化引起 PICA远端供血区低灌注引起梗死,此时多表现为分水岭梗死;③动脉-动脉栓塞或心源性栓塞,此时,往往合并后循环其它供血区梗死或前循环梗死。
本研究为回顾性分析,存在局限性:①样本量较小,且仅有65% 的患者接受了头颈CTA或头颅MRA检查,造成不同类型双侧小脑梗死椎-基底动脉变化特征未发现统计学差异,对责任动脉的改变评价不够充分;②临床随访资料不完善,未能对不同类型双侧小脑梗死临床预后进行对比分析。后期研究将采取前瞻性实验设计加大样本量与长期随访,对双侧小脑梗死的发病机理及预后进行更加深入研究。
综上所述,双侧小脑梗死病因复杂,累及不同供血动脉,其发病机制、影像特征有所不同,应区别分析。累及双侧PICA供血区不伴有小脑以外梗死灶时,应首先考虑原位动脉粥样硬化所致,血管成像(CTA、MRA或DSA)有助于显示椎动脉V4段或PICA的局限病变。由于PICA变异较大,血管成像可能无法准确判断有无异常,此时,磁共振磁敏感加权成像(SWI)有助于原位血栓的显示[13]。当梗死累及双侧PICA供血区同时合并后循环其它供血区梗死或前循环梗死时,应考虑动脉-动脉栓塞或心源性栓塞,此时应重点关注上一级动脉有无异常以及有无心源性栓子。针对不同病因进行个体化诊疗,将有助于改善病人预后、减少复发。
-
![]()
图 1 双侧PICA供血区急性梗死:一侧全供血区受累伴对侧PICA供血区受累
男性,34岁,突发眩晕、行走不稳就诊。头颅MRI检查(a)T1 WI、(b)T2 WI、(c)DWI、(d)ADC,可见左侧全PICA供血区急性区域性梗死病灶及右侧mPICA供血区急性小梗死病灶;(e)CTA显示右侧PICA起源于基底动脉(白色弧形箭头),左侧PICA起始部闭塞(白色箭头);(f)SWI可见左侧PICA起始部低信号血栓形成(黑色箭头)。本例双侧小脑梗死由左侧PICA原位血栓形成引起,由于存在解剖变异,右侧mPICA供血区可能部分由左侧PICA供血,因此引起双侧小脑PICA供血区梗死。
Figure 1. Acute infarction in bilateral PICA territory: Unilateral total infarct of PICA combined with the contralateral infarct of mPICA
![]()
图 2 双侧PICA供血区急性梗死:双侧mPICA供血区受累
男性,66岁,突发头晕就诊。头颅MRI检查(a)T1 WI、(b)T2 WI、(c)DWI,可见双侧mPICA供血区急性区域性梗死病灶,(d)头颅CTA右侧椎动脉V4段及双侧PICA均未见显示;该患者四年前头颅CTA(e)和(f)可见左侧PICA未发育,右侧PICA供应双侧小脑半球并可见局限性重度狭窄(白色箭头),本次右侧椎动脉及PICA闭塞引起双侧小脑半球急性梗死。
Figure 2. Acute infarction in bilateral PICA territory: Bilateral mPICA involved
![]()
图 3 双侧PICA供血区急性小梗死灶伴后循环其它供血区梗死
男性,62岁,意识障碍。头颅MRI检查DWI示双侧PICA供血区(a)和(b)及左侧SCA供血区、桥脑(c)多发小梗死灶,TOF-MRA双侧椎动脉颅内段、基底动脉均未显示,提示可能为椎-基底动脉弥漫病变所致动脉-动脉栓塞。
Figure 3. Acute small infarcts in bilateral PICA combined with other areas of the posterior circulation
表 1 双侧PICA供血区、双侧SCA供血区急性梗死MRI特征
Table 1 MRI characteristics of bilateral PICA and SCA territory acute infarction
MRI特征 组别(例数(%)) χ2 P 双侧PICA梗死
(38例)双侧SCA梗死
(40例)双侧区域性梗死 6(15.8) 5(12.5) 0.174 0.677 一侧区域性梗死+对侧梗死 15(39.5) 6(15.0) 5.933 0.015 双侧小梗死 17(44.7) 29(72.5) 6.208 0.013 累及后循环其它部位 8(21.0) 32(80.0) 27.103 <0.001 累及前循环 2(5.2) 2(5.0) 0.003 0.958  下载: 导出CSV
下载: 导出CSV
表 2 双侧PICA供血区、双侧SCA供血区急性梗死椎-基底动脉CTA/MRA表现特征
Table 2 CTA/MRA features of acute infarcted vertebrobasilar artery in bilateral PICA territory and bilateral SCA territory
椎-基底动脉CTA/MRA表现特征 组别(例数(%)) χ2 P 双侧PICA梗死
(24例)双侧SCA梗死
(27例)单一节段局限性重度狭窄/闭塞 13(54.2) 8(29.6) 3.158 0.076 多处或弥漫管腔狭窄、闭塞 8(33.3) 14(51.9) 1.776 0.183 未见管腔异常 3(12.5) 5(18.5) 0.348 0.555
下载: 导出CSV
-
[1] DZIADKOWIAK E, CHOJDAK-ŁUKASIEWICZ J, GUZIŃSKI M, et al. The usefulness of the toast classification and prognostic significance of pyramidal symptoms during the acute phase of cerebellar ischemic stroke[J]. Cerebellum, 2015, 15(2): 159−164.
[2] De COCKER L J, LÖVBLAD K O, HENDRIKSE J. MRI of Cerebellar Infarction[J]. European Neurology, 2017, 77(3/4): 137−146.
[3] WANG P Q, DING Z G, ZHANG G B, et al. A study on lesion pattern of bilateral cerebellar infarct[J]. European Review for Medical and pharmacological Sciences, 2015, 19(10): 1845−1851.
[4] 张伟晴, 蔡俊秀, 樊露, 等. 双侧小脑急性梗死模式观察与分析[J]. 中华老年心脑血管病杂志, 2019,21(4): 403−406. DOI: 10.3969/j.issn.1009-0126.2019.04.017. ZHANG W Q, CAI J X, FAN L, et al. Analysis of acute bilateral cerebellar infarction patterns[J]. Chinese Journal of Geriatric Heart Brain and Vessel Diseases, 2019, 21(4): 403−406. DOI: 10.3969/j.issn.1009-0126.2019.04.017. (in Chinese).
[5] AMARENCO P, LÉVY C, COHEN A, et al. Causes and mechanisms of territorial and nonterritorial cerebellar infarcts in 115 consecutive patients[J]. Stroke, 1994, 25(1): 105−112. doi: 10.1161/01.STR.25.1.105
[6] HONG J M, BANG O Y, CHUNG C S, et al. Frequency and clinical significance of acute bilateral cerebellar infarcts[J]. Cerebrovascular Diseases, 2008, 26(5): 541−548. doi: 10.1159/000160211
[7] PETTY G W, BROWN R D, WHISNANT J P, et al. Ischemic stroke subtypes: A population-based study of functional outcome, survival, and recurrence[J]. Stroke, 2000, 31(5): 1062−1068. DOI: 10.1161/01.STR.31.5.1062.
[8] BOUKOBZA M, LAISSY J P. Unusual pattern of bilateral cerebellar infarct and bihemispheric posterior-inferior cerebellar artery[J]. Journal of Neurology, Neurosurgery and Psychiatry, 2021, 17: 433−436.
[9] HAN S W, CHO G C, BAIK J S, et al. Bilateral cerebellar infarction caused by dominant medial posterior inferior cerebellar artery[J]. Neurology, 2006, 66(7): 1125−1126. doi: 10.1212/01.wnl.0000204293.27365.ec
[10] MARINKOVIĆ S, KOVACEVIĆ M, GIBO H, et al. The anatomical basis for the cerebellar infarcts[J]. Surgical Neurology, 1995, 44(5): 460−461.
[11] 李雯雯, 孙启英, 易芳, 等. 小脑后下动脉解剖变异致双侧小脑梗死2例报道并文献复习[J]. 卒中与神经疾病, 2017,24(4): 302−305. DOI: 10.3969/j.issn.1007-0478.2017.04.006. LI W W, SUN Q Y, YI F, et al. Clinical analysis of bilateral cerebellar infarction caused by anatomic variations of the posterior inferior cerebellar artery in two patients and literature review[J]. Stroke and Nervous Diseases, 2017, 24(4): 302−305. DOI: 10.3969/j.issn.1007-0478.2017.04.006. (in Chinese).
[12] 程敏, 李浩然, 朱洋洋, 等. 小脑后下动脉少见变异导致的双侧小脑半球梗死1例报告[J]. 中风与神经疾病杂志, 2015,32(6): 556−557. [13] FUJIMOTO M, SALAMON N, MAYOR F, et al. Characterization of arterial thrombus compostion by magnetic resonance imaging in a swine stroke model[J]. Stroke, 2013, 44(5): 1463. doi: 10.1161/STROKEAHA.111.000457
-
期刊类型引用(3)
1. 张丽丽,吴婧,董兰真. 急性小脑梗死患者认知功能变化及其与大脑结构网络的相关性研究. 临床和实验医学杂志. 2024(05): 449-453 .  百度学术
百度学术
2. 陈文静,沈龙山,朱越. 小脑梗死的影像评估及临床研究进展. 分子影像学杂志. 2024(07): 769-773 . 百度学术
3. 任宇虹. 螺旋CT血管造影和颈部血管超声对急性脑梗死患者颈动脉系统检查的影响. 影像研究与医学应用. 2022(22): 166-168 . 百度学术
其他类型引用(1)

计量
- 文章访问数: 288
- HTML全文浏览量: 169
- PDF下载量: 21
- 被引次数: 4


