
Development of Motion Artifact Correction Solutions for the Cone-beam CT Images during Pancreatic Cancer Image-guided Radiotherapy
-
摘要:
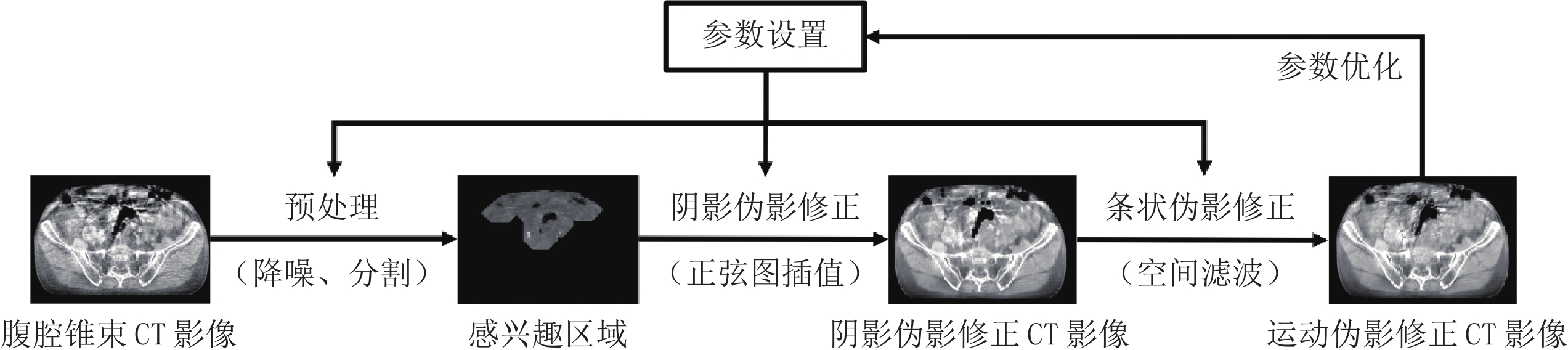
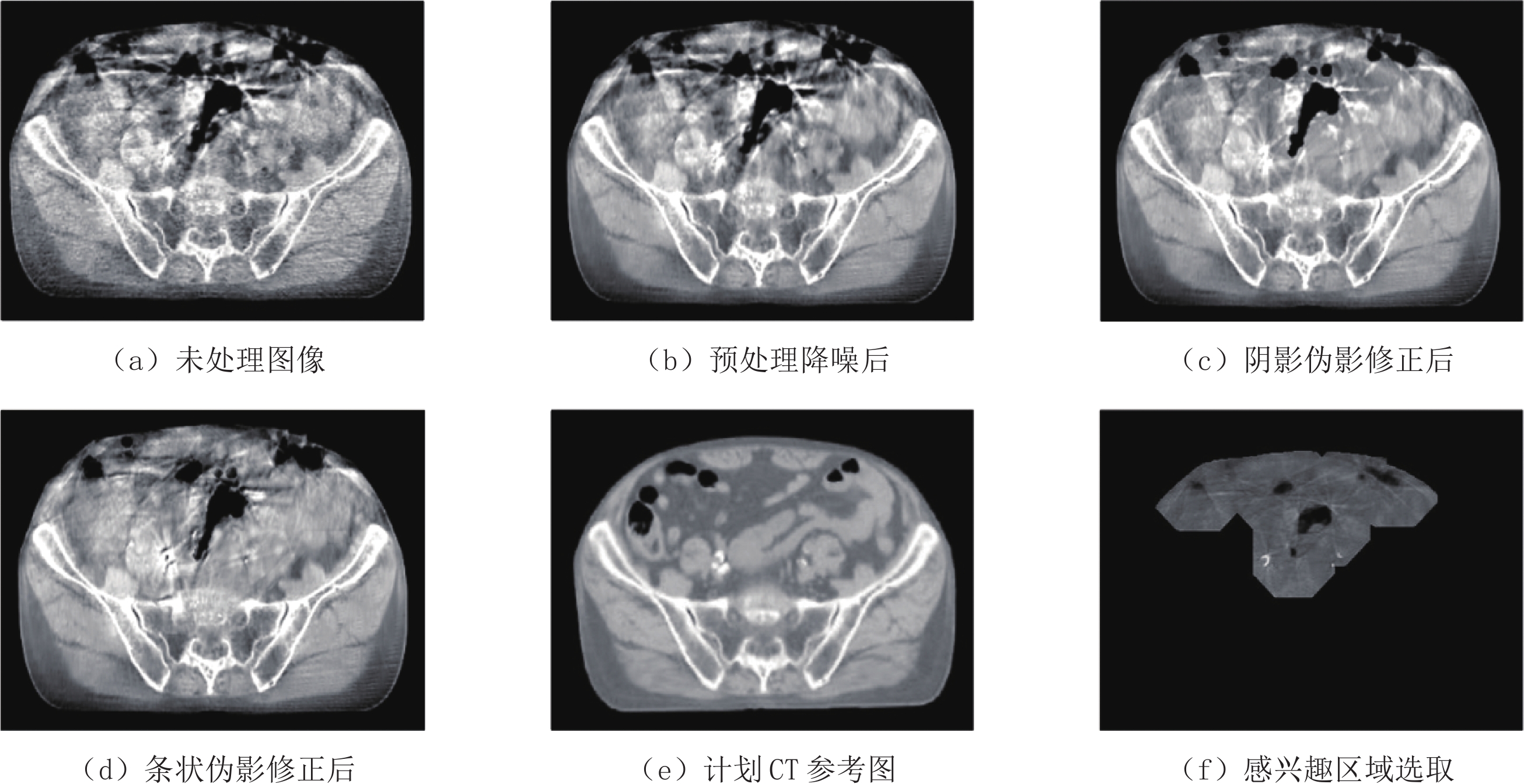
基于二维平板探测器技术的锥束CT系统广泛应用于放射治疗前的摆位验证,但在以胰腺癌为代表的腹腔肿瘤放疗应用中会遇到呼吸运动和肠道蠕动导致的严重阴影与条状伪影问题,难以从CT影像中分辨病灶区域。由于胰腺等柔性脏器在呼吸运动作用下会存在非刚性形变,体表运动监测结果和实际脏器运动间存在难以量化的偏差,也难以监测以肠道蠕动为代表的不规则运动,故腹腔锥束CT运动伪影修正问题缺乏有效解决方案。本文基于生物动力学理论和人体生理学常识,提出全新的无需运动监测或体内标记物植入的放疗图像引导锥束CT运动伪影修正方法,设计基于伪影图像特征、融合各类CT图像域处理算法的伪影修正策略。将该策略应用于临床腹腔锥束CT影像处理后所得结果表明锥束CT图像质量有显著改善,典型软组织区域的平均CT数误差从90 HU降到30 HU,肠道空腔边界和周边软组织信息得到部分恢复。本文开发的伪影修正策略无需呼吸门控或增加投影数,避免标记物植入手术,可集成到现有工作流,为胰腺癌放疗图像引导提供肿瘤定位信息。
Abstract:The cone-beam CT (CBCT) system based on the two-dimensional flat-panel detector technology is widely applied in patient location verification before radiotherapy. However, during the application of intraperitoneal tumor radiotherapy, severe shading and streaking artifacts caused by respiratory movement and intestinal peristalsis make it difficult to distinguish tumor areas from the CBCT images. Due to the non-rigid deformation of flexible organs such as the pancreas under the action of respiratory motion, it is hard to quantify deviation between the body surface motion monitoring results and the actual organ motion, and it is also difficult to monitor irregular motion represented by intestinal peristalsis. There is no effective solution to motion artifact correction in CBCT. Based on theory of biodynamics and common knowledge of human physiology, in this paper we propose a brand new radiotherapy image-guided cone-beam CT motion artifact correction method without motion monitoring or implantation of in-vivo markers. The proposed artifact correction strategy is designed based on the features of the artifact images and fusion of various CT image domain processing algorithms. The results suggest that the image quality of cone beam CT has been significantly improved after the application of this strategy in the clinical abdominal CBCT image processing. The average CT number error in typical soft tissue areas reduces from 90 HU to 30 HU, and the boundary of the intestinal cavity and surrounding soft tissue information are partially recovered. The proposed artifact correction strategy does not require respiratory gating or increase of projections, which can be integrated into existing workflows without marker implantation surgery. The motion-artifact-corrected CBCT images provide more accurate tumor localization information for image-guided radiotherapy of pancreatic carcinoma. The proposed method is proved practical and efficient for clinical applications
-
肺癌作为世界范围内常见的恶性肿瘤,也是癌症死亡的主要原因[1]。随着低剂量CT筛查的开展,越来越多肺部病变得以发现,但部分病灶新旧交替,影像学特征存在重叠,为良恶性鉴别带来困难,因此评估病灶性质、对患者的预后和生活质量有重要的意义。
CT引导下经皮穿刺活检(percutaneous transthoracic needle biopsy,PTNB)于1976年被初次描述,依据活检针类型不同,可分为细针抽吸活检(fifine needle aspiration,FNA)和切割针活检(core needle biopsy,CNB)两大类,是诊断肺部病变,尤其是周围型病变的微创方法,以诊断成功率高、并发症发生率低在临床广泛应用;但部分病灶取材不充分,存在假阴性的情况,为其带来一定局限性[2]。如何早期、快速地判断病变组织是否穿刺成功是一个亟待解决的问题。
快速现场评价(rapid on site evaluation,ROSE)技术于1981年被提出,可对检查过程中样本获得的充分性给予即时反馈,指导操作者修改取样技术,如取样的部位和深度,还可以进行快速诊断。但关于ROSE能否提高诊断准确率目前尚有争议,例如:Liu等[3]回顾研究认为C-ROSE有助于指导EBUS-TBNA操作进程,但并未提高TBNA的病理诊断率;Monaco等[4]研究认为,C-ROSE对EBUS-TNBA的诊断率无明显影响,但有助于保障标本的有效性和充足度,能为流式细胞、免疫染色和分子病理学等后继检测提供优选标本。
1. 研究目的
CT引导下穿刺活检联合快速现场评价对肺部病灶的诊断是否具有指导意义是未知的,因此本研究总结现有文章,通过定量系统评价的方法,主要目标是研究CT引导下穿刺活检联合ROSE对肺部病变的诊断价值,次要目标是研究此项操作的并发症,为临床选择合理的诊断方法提供依据。
2. 材料和方法
本次系统评价根据PRISMA(系统评价和荟萃分析的首选报告项目)的指南[5]进行,以评估CT引导下穿刺活检联合快速现场评价对肺部病变诊断价值。
2.1 纳入标准与排除标准
纳入标准。①研究类型:诊断性实验,以评价CT引导下联合ROSE对肺部病变诊断价值为目标,语种为英语,可以直接或间接计算出四格表值。②研究对象:CT引导下穿刺活检前已知有肺部病变的患者。③诊断标准:因ROSE是细胞涂片的快速染色,缺乏组织学形态,因此它在诊断中不能有效区分肺癌的病理类型,只能初步判断良恶性。所以CT引导下穿刺活检联合ROSE的最终结果与金标准,即外科手术、组织病理学检查结果进行比较判断。④评价指标:可以从原始研究中找到或计算出足够的数据,如TP(真阳性率)、TN(真阴性率)、FP(假阳性率)、FN(假阴性率)、并发症的数量及类型、取材充分性。
排除标准。①未经上述金标准确诊;②评论文章、信件、动物实验、案例报告。
2.2 检索策略
我们搜索了PubMed和EMBASE,截至2022年10月,在数据库中搜索了以下关键词及其相关MeSH术语:“Biopsy,Needle”、“Tomography”、“X-ray Computed”、“Rapid On-site Evaluation”、“Lung Neoplasms”、“sensitivity and specificity”,只考虑英文出版物,同时通过以下途径获取已发表、未发表和在研研究:
①通过Pubmed的“Related Articles”功能获取已纳入研究的相关研究;②通过Science Citation Index获取已纳入研究的引用的研究;③追查已纳入研究的参考文献。
2.3 数据提取与质量评价
两位独立作者首先审查所有标题与摘要,以确定潜在的相关文章。按设计好的资料提取表提取资料,并通过讨论解决分歧。提取以下数据:
①纳入研究基本特征:第一作者、发表日期、标题、刊名、国家等。②研究对象:研究设计、样本量、诊断方法、参考实验等。③评价指标:四格表数据(真阳性、假阳性、真阴性、假阴性)。采用更新的诊断准确性研究质量评价工具(QUADAS-2)[6],对纳入的每个研究按“是”、“否”、“不清楚”评价,对应偏倚风险等级判定为“低”、“高”或“不确定”。
3. 统计分析
在诊断性试验Meta分析中,阈值效应是引起精确研究异质性的主要原因之一,对于阈值效应通过计算灵敏度(真阳性)与特异度(真阴性的)Spearman相关系数进行判断,若二者之间Spearman相关系数呈现强负相关,且P<0.05,提示存在阈值效应,则拟合SROC曲线和计算AUC。
当纳入研究间不存在阈值效应时,进一步采用
$\chi^2 $ 检验分析纳入研究结果间的统计学异质性,并结合$I^2 $ 定量判断异质性的大小。若$I^2 $ <50%,采用固定效应模型进行合并分析,反之则采用随机效应模型进行合并分析,并通过亚组分析确定异质性来源。最后计算合并的灵敏度、特异度、诊断优势比(diagnostic odds ratio,DOR)、综合受试者工作特征(summary receiver operating characteristics,SROC)曲线下面积(area under curve,AUC)和Q指数。Q指数越大,表示诊断试验的准确性越大。运用Deek漏斗图评价发表偏倚。使用Stata13、Rev Man(版本5.3)和Meta-disc(版本1.4)软件对本系统评价中的所有统计数据进行分析,P<0.05被认为具有统计学意义。
4. 结果
4.1 文献的筛查与纳入
通过Pubmed、Embase主题词相关检索共发现文献19篇,通过参考文献发现文献4篇,浏览题目及摘要后排除文献11篇。通篇阅读后排除文献6篇,最后6篇文章符合标准纳入Meta分析,文献流程图见图1。
4.2 研究特点归纳
6项研究[7-12]均以英文发表,共计1179例受试者被纳入,951例接受了最终病理学检查(Fassina 等[8]在311例受试者中最终86例接受了组织病理学检查,Santambrogio等[11]对3例患者活检后接受15~21个月的放射学随访,因病灶没有变化被包括在真阴性组中)。前瞻性研究4项、回顾性研究2项,4项研究设置了对照组。
取材方式5项为细针抽吸活检,1项为切割针活检,ROSE染色多样(3项采用迪夫试剂,1项为甲苯胺蓝试剂,1项为亚甲基蓝试剂,1项为姬姆萨试剂)。
快速现场判读人员均为细胞病理学家。原始数据汇总见表1。纳入研究的方法学质量评价见图2。
表 1 纳入研究文献的基本资料汇总Table 1. Study characteristics and demographicsAuthor-year Country Study design No. of
patientsNo. of biopsy Main sampling
sitesRose reagent Rose reporter Sampling
methodAnila et al, 2018 India PCS 50 50 masses toluidine blue pathologist FNA Fassina et al,
2011Italy PCS 311 86 - Giemsa pathologist FNA Liu et al, 2022 China RCT 108 108 nodules Diff-quik pathologist FNA Peng et al, 2020 China RCS 205 205 nodules/masses Diff-quik pathologist FNA Santambrogio et al, 1997 Italy RCT 220 207 nodules Giemsa pathologist FNA Yiminniyaze et al, 2022 China RCS 285 285 nodules/masses Diff-quik pathologist CNB Author-year No. of patients Adequacy Complication(n) Tp Fp Fn Tn R NR R NR R NR Anila et al, 2018 50 - 39 - Pneumothorax(3) - 31 0 3 16 Fassina et al,
2011311 - 305 - Pneumothorax(13)
haemoptysis (4)
Chest pain(3)- 77 0 3 6 Liu et al, 2022 56 52 52 41 Pneumothorax(6)
haemoptysis (10)Pneumothorax(7)
haemoptysis (11)28 2 4 22 Peng et al, 2020 132 102 - - Pneumothorax(9)
haemoptysis (2)Pneumothorax(15)
haemoptysis (2)57 4 7 64 Santambrogio et al, 1997 110 110 110 97 Pneumothorax(29) Pneumothorax(23) 63 1 7 26 Yiminniyaze et al, 2022 163 122 160 105 Pneumothorax(34)
haemoptysis (21)Pneumothorax(16)
haemoptysis (11)150 0 3 6 注:RCT为随机对照试验;RCS为回顾性研究;PCS为前瞻性研究;ROSE为快速现场评价;NR为未进行快速现场评价。 ![]() 图 2 QUADAS-2质量评价表Figure 2. Assessment of reporting quality by the QUADAS-2 scoring system
图 2 QUADAS-2质量评价表Figure 2. Assessment of reporting quality by the QUADAS-2 scoring system4.3 阈值效应
观察ROC曲线图发现其不呈“肩臂状”分布,计算灵敏度对数与1-特异度对数Spearman相关系数,其结果为0.83(P>0.05),表明本研究不存在阈值效应。
4.4 Meta分析结果
异质性检验显示各研究间灵敏度之间存在轻度异质性(
$\chi^2 $ =12.90,P=0.02,$I^2 $ =61.20),采用随机效应模型进行效应量合并;特异度($\chi^2 $ =3.54,P=0.62,$I^2 $ =0)、诊断比值比($\chi^2 $ =1.81,P=0.88,$I^2 $ =0)间不存在异质性,采用固定效应模型进行效应量合并,最后得到95% 置信区间的敏感度、特异度、DOR分别为0.94(95% CI:0.91~0.96)、0.95(95% CI:0.90~0.98)、159.05(95% CI:69.59~363.49)。SROC AUC为0.98,Q指数为 0.93,具体数据见图3。![]() 图 3 CT引导下穿刺活检联合ROSE的汇总灵敏度、特异度、诊断比值比及SRCOC曲线的森林图Figure 3. Forest plot showing the sensitivity (SEN), specificity (SPE), diagnostic odds ratio (DOR), and summary receiver operating characteristic curve (SROC) of the six studies and the pooled estimates
图 3 CT引导下穿刺活检联合ROSE的汇总灵敏度、特异度、诊断比值比及SRCOC曲线的森林图Figure 3. Forest plot showing the sensitivity (SEN), specificity (SPE), diagnostic odds ratio (DOR), and summary receiver operating characteristic curve (SROC) of the six studies and the pooled estimates4.5 亚组分析
以研究类型:前瞻性研究与回顾性研究。发表国家:中国与非中国。发表年限:2010年之前与2010年之后为亚组进行分析。分析显示灵敏度研究间异质性来源与研究类型有关,回顾性研究灵敏度高于前瞻性研究,差异有统计学意义,具体数据分析见图4。
4.6 取材充分性、诊断准确率与并发症
共有4项研究设立了对照[9-12],1项研究未提及取材充分性与诊断准确率[10]。图5显示了满足条件的3组研究中,R0SE组与非ROSE取材充分性与诊断准确性的结果,应用ROSE后,Meta分析显示取材充分性提高了12%(95% CI:0.08~0.16,
$I^2 $ =0),诊断准确性提高了13%(95% CI:0.06~0.19,$I^2 $ =41)。ROSE与非ROSE组并发症没有统计学意义。![]() 图 5 (A)ROSE组与非ROSE组取材充分性的森林图;(B)ROSE组与非ROSE组诊断准确性的森林图;(C)ROSE组与非ROSE组的并发症发生率;RD,风险差异;ROSE,快速现场评价Figure 5. (A) Forest plot comparing the adequacy rate with or without ROSE in the included studies; (B) Forest plot comparing the accuracy with or without ROSE in the included studies; (C) Forest plot comparing the incidence of complication with or without in the included studies. RD, risk difference; ROSE, rapid on-site evaluation
图 5 (A)ROSE组与非ROSE组取材充分性的森林图;(B)ROSE组与非ROSE组诊断准确性的森林图;(C)ROSE组与非ROSE组的并发症发生率;RD,风险差异;ROSE,快速现场评价Figure 5. (A) Forest plot comparing the adequacy rate with or without ROSE in the included studies; (B) Forest plot comparing the accuracy with or without ROSE in the included studies; (C) Forest plot comparing the incidence of complication with or without in the included studies. RD, risk difference; ROSE, rapid on-site evaluation4.7 发表偏移
应用Deeks'漏斗图进行分析,P>0.1,表示不存在发表偏移(图6)。
![]() 图 6 针对6项研究的发表偏倚检测Figure 6. Deeks' funnel plot asymmetry test for publication bias of the six studies included in the Meta-analysis
图 6 针对6项研究的发表偏倚检测Figure 6. Deeks' funnel plot asymmetry test for publication bias of the six studies included in the Meta-analysis5. 讨论
ROSE在肺穿刺活检中的诊断价值:CT引导下穿刺活检是肺部病灶取材常见的方法,由于其侵入性低和可接受的并发症率,临床上经常使用,但受操作者的熟练程度、病灶位置和大小的影响,仍有一些肺癌患者无法获得足够的合格样本进行准确诊断[13],从而导致漏诊和有效治疗的延迟。在诊断性介入肺脏病学操作中,ROSE是一项实时伴随于取材过程的快速细胞学判读技术,获取满意靶标本后,操作适可而止,不仅可节省操作时间和资源,还可减少患者痛苦及并发症。
在设立对照组的3项研究中,ROSE组中329例患者中有322例取得满意标本,316例完成了准确诊断,非ROSE组中284例患者中有243例取得满意标本,237例完成了准确诊断,应用ROSE在肺部病灶取材充分性、诊断准确率分别提高12% 和13%。
随着精准治疗时代的到来,获得足够多的样本来评估患者的病理类型、分子分型、基因状态和免疫状态,是医学上迫切需要解决的问题。Trisolini等[14]对肺癌样本多基因分析中发现,ROSE组中有更多患者获得完整的基因分型(ROSE组为90.8%,非ROSE组为80.3%),表明ROSE可以增加肿瘤细胞比例较高的样本数量,从而提高免疫组化和基因分型的成功率,避免二次手术创伤和检查的费用。
在满足纳入条件的6项研究中,应用ROSE诊断肺部病灶特异度的异质性不显著,灵敏度存在轻度异质性,通过亚组分析,发现异质性来源与研究类型有关。因回顾性研究存在选择偏移和时间偏倚,对灵敏度产生一定影响,故应用随机效应模型进行分析,合并灵敏度、特异度、AUC分别为94%、95%、0.97,表明CT引导下穿刺活检结合快速现场评价,对肺部病灶良恶性有较高的诊断准确性。CT引导下穿刺活检常见的并发症包括气胸、出血和胸膜反应等。少量气胸、出血不需特殊处理,可以自行吸收。纳入分析的6项研究中ROSE组的不良反应发生率为30.3%,非ROSE组不良反应发生率为23.9%,差异无统计学意义,表明CT引导下穿刺活检联合快速现场评价对肺部病灶的诊断具有较高的安全性。
本研究遵循诊断性试验Meta分析推荐的报告规范。虽然在进行本篇Meta分析时我们进行了细致地文献检索和数据提取,然而,仍存在一定的局限性。首先,目前国内外关于ROSE在CT引导下经皮穿刺肺活检应用的研究很少,研究结论也不尽相同;其次本研究没有将CT引导下经皮穿刺肺活检与其他影像引导方式结果进行直接比较。希望在未来的研究中收集更多的样本后继续研究这个问题。
6. 结论
总之,CT引导下穿刺活检联合快速现场评价是一种安全、实用的辅助检查手段,在肺部病变中具有较高的高诊断准确性、敏感性和特异性,可作为诊断肺部病灶的重要方法之一。
-
![]()
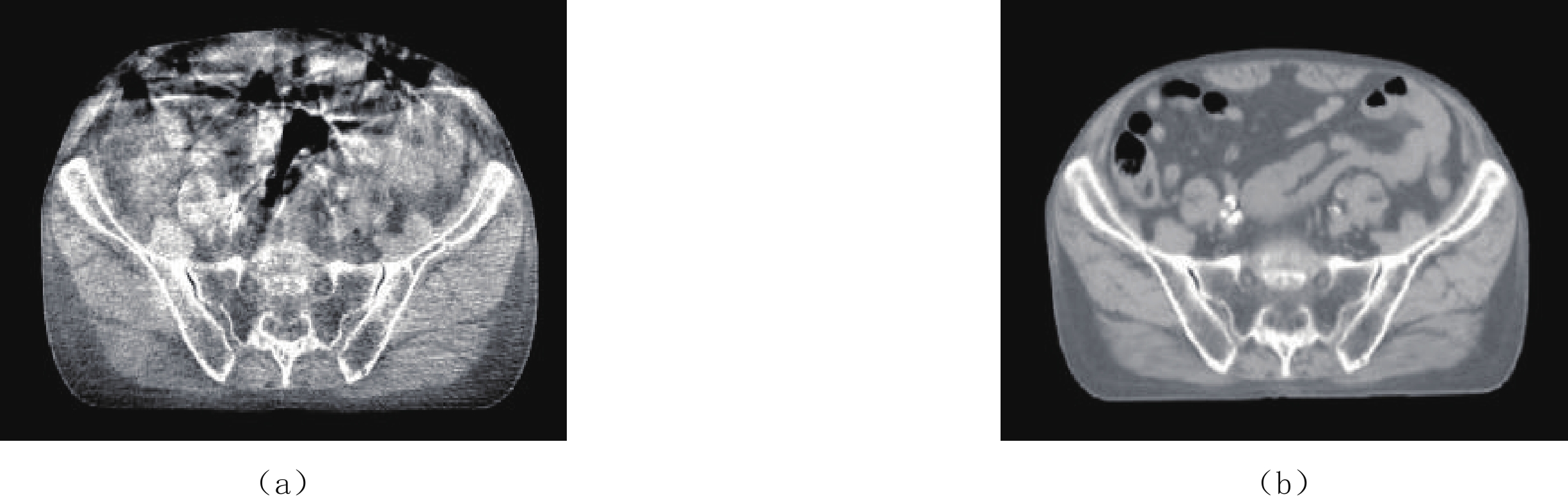
图 1 同一位患者的腹腔锥束CT(a)和诊断CT(b)扫描横断面图像(显示窗:[-500, 500] HU)
Figure 1. Comparison between the transverse images from abdominal cone-beam CT and diagnostic CT scans of one patient (Display window: [-500, 500] HU)
![]()
图 2 胰腺癌放疗图像引导锥束CT图像域运动伪影修正策略
Figure 2. Proposed image-domain motion artifact correction strategy for CBCT in IGRT of pancreatic cancer
![]()
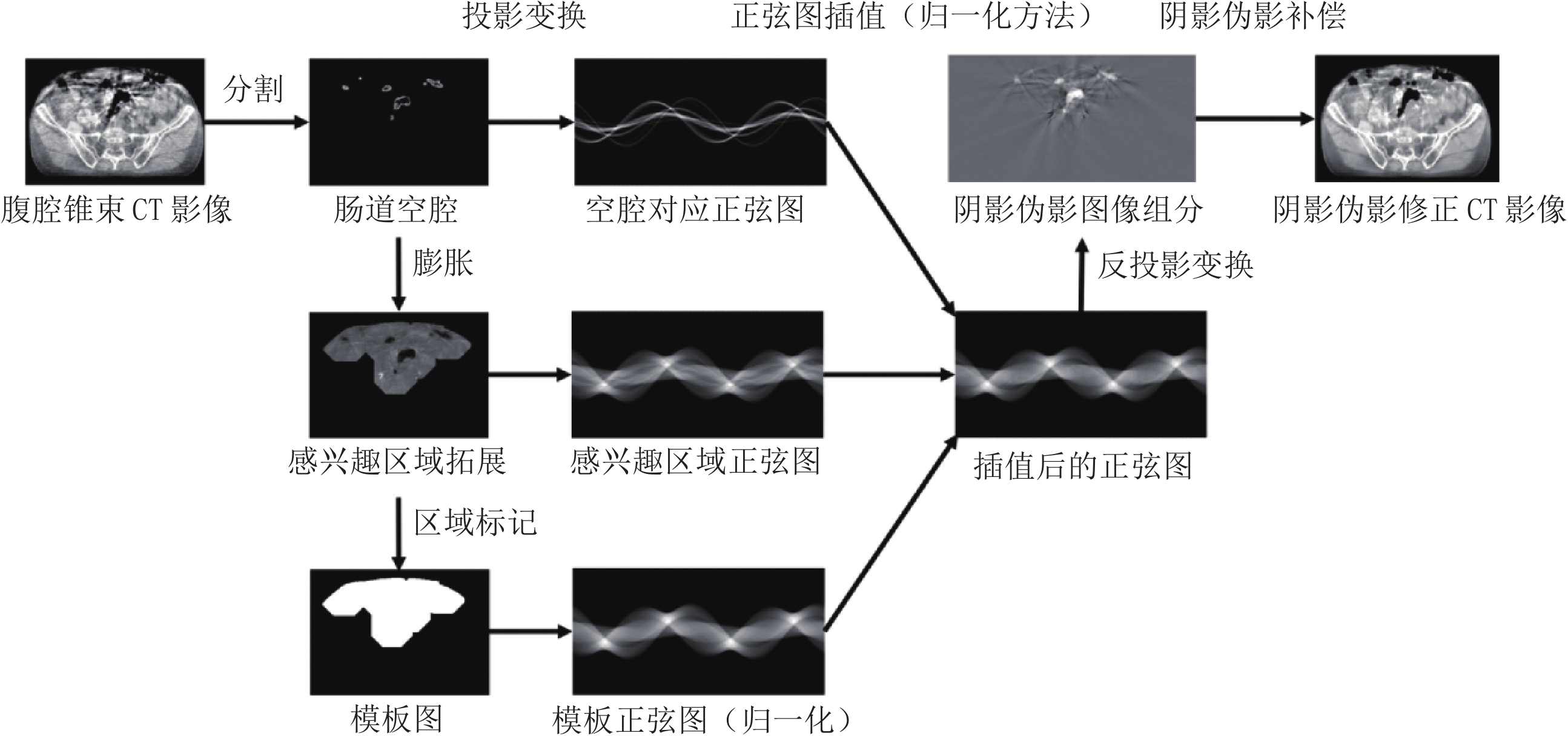
图 3 胰腺癌放疗图像引导锥束CT图像域阴影伪影修正流程
Figure 3. Proposed shading artifact correction flowchart for CBCT in IGRT of pancreatic cancer
![]()
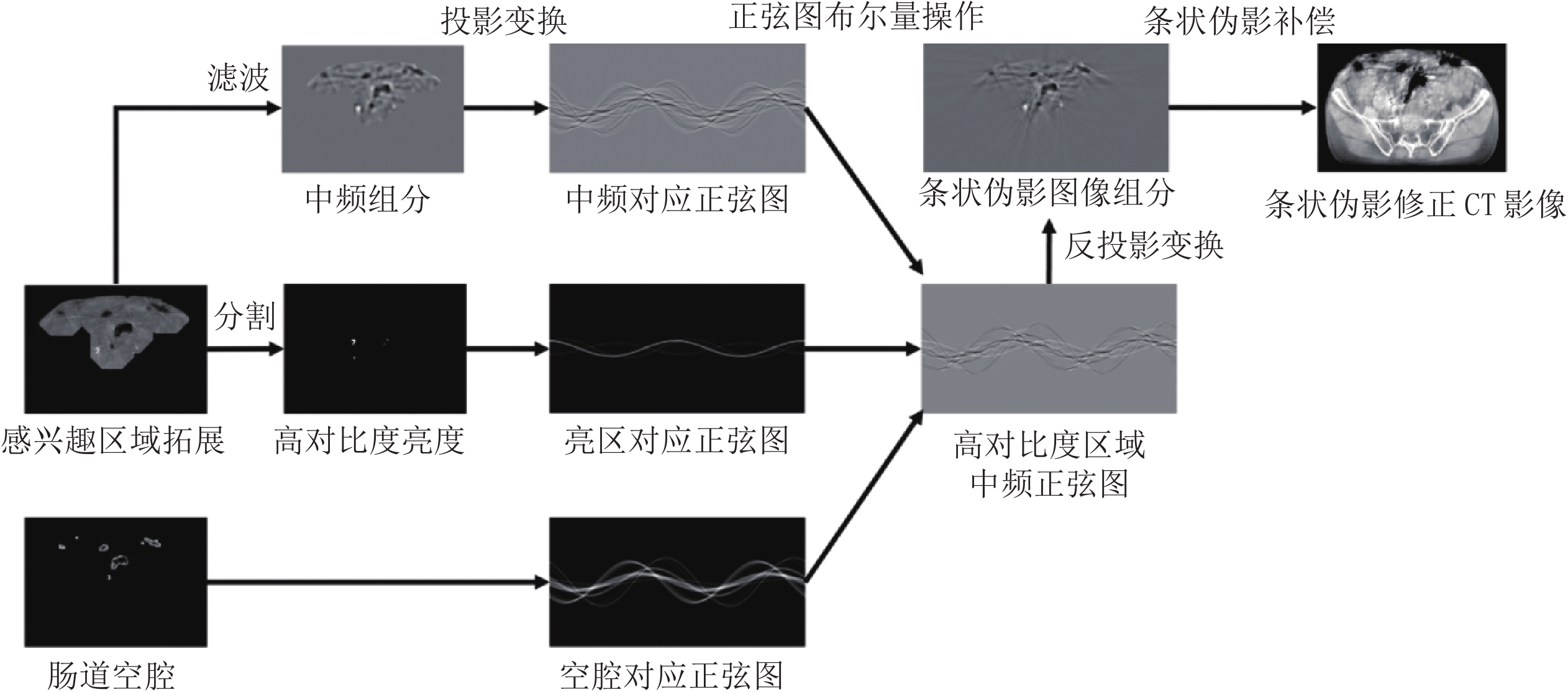
图 4 胰腺癌放疗图像引导锥束CT图像域条状伪影修正流程
Figure 4. Proposed streaking artifact correction flowchart for CBCT in IGRT of pancreatic cancer
![]()
图 5 腹腔锥束CT运动伪影修正效果(横断面视图)
Figure 5. Motion artifact correction results for one abdominal CBCT scan (transverse view)
![]()
图 6 腹腔锥束CT运动伪影修正效果(矢状位视图)
Figure 6. Motion artifact correction results for one abdominal CBCT scan (sagittal view)
![]()
图 7 腹腔锥束CT运动伪影修正效果(横断面和和矢状位视图)
Figure 7. Motion artifact correction results for another abdominal CBCT scan (transverse and sagittal views)
表 1 Trilogy放疗机OBI锥束CT系统的扫描参数
Table 1 Scan parameters of the OBI CBCT system on Trilogy radiotherapy device
扫描参数名 参数值 源到探测器距离(SID)/mm 1501 源到转轴距离(SAD)/mm 1000 探测器水平偏移量/mm 148 扫描电压/kVp 125 扫描电流/mA 80 扫描模式 腹腔、半扇 投影角数量 663  下载: 导出CSV
下载: 导出CSV
表 2 腹腔锥束CT运动伪影修正后图像质量指标变化
Table 2 Changes in image quality indicators before and after abdominal CBCT motion artifact correction
图像质量指标 修正前 修正后 整体图像PSNR/dB 41.562 61.110 感兴趣区域PSNR/dB 47.593 62.263 整体图像SSIM 0.844 0.939 感兴趣区域CT数MAE/HU 92.348 33.762 感兴趣区域CT数RMSE/HU 98.986 42.873
下载: 导出CSV
-
[1] SIEWERDSEN J H, JAFFRAY D A. Cone-beam computed tomography with a flat-panel imager: Magnitude and effects of X-ray scatter[J]. Medical Physics, 2001, 28(2): 220−231. doi: 10.1118/1.1339879
[2] JAFFRAY D A, SIEWERDSEN J H, WONG J W, et al. Flat-panel cone-beam computed tomography for image-guided radiation therapy[J]. International Journal of Radiation Oncology, Biology, Physics, 2002, 53(5): 1337−1349. doi: 10.1016/S0360-3016(02)02884-5
[3] SABEL M. First results with the varian on-board imager (TM)[J]. Strahlentherapie und Onkologie, 2005: 181.
[4] ABBAS H, CHANG B, CHEN Z J. Motion management in gastrointestinal cancers[J]. Journal of Gastrointestinal Oncology, 2014, 5(3): 223−235.
[5] MURPHY M J, MARTIN D, WHYTE R, et al. The effectiveness of breath-holding to stabilize lung and pancreas tumors during radiosurgery[J]. International Journal of Radiation Oncology, Biology, Physics, 2002, 53(2): 475−482. doi: 10.1016/S0360-3016(01)02822-X
[6] SONKE J J, ZIJP L, REMEIJER P, et al. Respiratory correlated cone beam CT[J]. Medical Physics, 2005, 32(4): 1176−1186. doi: 10.1118/1.1869074
[7] LI T F, XING L, MUNRO P, et al. Four-dimensional cone-beam computed tomography using an on-board imager[J]. Medical Physics, 2006, 33(10): 3825−3833. doi: 10.1118/1.2349692
[8] DIETRICH L, JETTER S, TUCKING T, et al. Linac-integrated 4D cone beam CT: First experimental results[J]. Physics in Medicine and Biology, 2006, 51(11): 2939−2952. doi: 10.1088/0031-9155/51/11/017
[9] SONKE J J, ROSSI M, WOLTHAUS J, et al. Frameless stereotactic body radiotherapy for lung cancer using four-dimensional cone beam CT guidance[J]. International Journal of Radiation Oncology, Biology, Physics, 2008, 74(2): 567−574.
[10] BISSONNETTE J P, FRANKS K N, PURDIE T G, et al. Quantifying interfraction and intrafraction tumor motion in lung stereotactic body radiotherapy using respiration-correlated cone beam computed tomography[J]. International Journal of Radiation Oncology, Biology, Physics, 2009, 75(3): 688−695. doi: 10.1016/j.ijrobp.2008.11.066
[11] SHIEH C C, KIPRITIDIS J, O'BRIEN R T, et al. Image quality in thoracic 4D cone-beam CT: A sensitivity analysis of respiratory signal, binning method, reconstruction algorithm, and projection angular spacing[J]. Medical Physics, 2014, 41(4): 041912.
[12] STEINER E, SHIEH C C, CAILLET V, et al. 4-Dimensional cone beam computed tomography-measured target motion underrepresents actual motion[J]. International Journal of Radiation Oncology, Biology, Physics, 2018, 102(4): 932−940. doi: 10.1016/j.ijrobp.2018.04.056
[13] SHIMOHIGASHI Y, TOYA R, SAITO T, et al. Tumor motion changes in stereotactic body radiotherapy for liver tumors: An evaluation based on four-dimensional cone-beam computed tomography and fiducial markers[J]. Radiation Oncology, 2017, 12(1): 61.
[14] TOYA R, SAITO T, SHIMOHIGASHI Y, et al. Four-dimensional cone-beam computed tomography-guided radiotherapy for gastric lymphoma[J]. Japanese Journal of Radiology, 2018, 36(2): 159−163. doi: 10.1007/s11604-017-0698-8
[15] JIN P, HULSHOF M C C M, van WIERINGEN N, et al. Interfractional variability of respiration-induced esophageal tumor motion quantified using fiducial markers and four-dimensional cone-beam computed tomography[J]. Radiotherapy and Oncology, 2017, 124(1): 147−154. doi: 10.1016/j.radonc.2017.05.015
[16] OHIRA S, ISONO M, UEDA Y, et al. Assessment with cone-beam computed tomography of intrafractional motion and interfractional position changes of resectable and borderline resectable pancreatic tumours with implanted fiducial marker[J]. British Journal of Radiology, 2017, 90(1072): 20160815.
[17] MARCHANT T E, PRICE G J, MATUSZEWSKI B J, et al. Reduction of motion artefacts in on-board cone beam CT by warping of projection images[J]. British Journal of Radiology, 2011, 84(999): 251−264. doi: 10.1259/bjr/90983944
[18] MARCHANT T E, SKALSKI A, MATUSZEWSKI B J. Automatic tracking of implanted fiducial markers in cone beam CT projection images[J]. Medical Physics, 2012, 39(3): 1322−1334. doi: 10.1118/1.3684959
[19] WANG M J, SHARP G C, RIT S, et al. 2D/4D marker-free tumor tracking using 4D CBCT as the reference image[J]. Physics in Medicine and Biology, 2014, 59(9): 2219−2233. doi: 10.1088/0031-9155/59/9/2219
[20] ZACHIU C, de SENNEVILLE B D, TIJSSEN R H N, et al. Non-rigid CT/CBCT to CBCT registration for online external beam radiotherapy guidance[J]. Physics in Medicine and Biology, 2018, 63(1): 015027.
[21] LIU J L, ZHANG X, ZHANG X Q, et al. 5D respiratory motion model based image reconstruction algorithm for 4D cone-beam computed tomography[J]. Inverse Problem, 2015, 31(11): 115007. doi: 10.1088/0266-5611/31/11/115007
[22] ZHANG H, MA J H, BIAN Z Y, et al. High quality 4D cone-beam CT reconstruction using motion-compensated total variation regularization[J]. Physics in Medicine and Biology, 2017, 62(8): 3313−3329. doi: 10.1088/1361-6560/aa6128
[23] PETERLIK I, STRZELECKI A, LEHMANN M, et al. Reducing residual-motion artifacts in iterative 3D CBCT reconstruction in image-guided radiation therapy[J]. Medical Physics, 2021, 48(10): 6497−6507. doi: 10.1002/mp.15236
[24] VOOGT J, de BOIS J, van HERK M, et al. Cone beam CT motion artifact reduction by projection image selection[C]//University of Toronto. Proceedings of the XVth International Conference on the Use of Computers in Radiation Therapy (ICCR 2007), Toronto, Canada, 2007: 13-17.
[25] NIJKAMP J, VOOGT J, DE BOIS J, et al. Improved automatic prostate localization after cone beam CT motion artefact reduction[J]. Radiotherapy and Oncology, 2008, 88: S108−S. doi: 10.1016/j.radonc.2007.10.030
[26] MÄKINEN Y, AZZARI L, FOI A. Collaborative filtering of correlated noise: Exact transform-domain variance for improved shrinkage and patch matching[J]. IEEE Transactions on Image Processing, 2020, 29: 8339−8354. doi: 10.1109/TIP.2020.3014721
-
期刊类型引用(2)
1. 倪剑刚. 多层螺旋CT多期扫描对胰腺癌的诊断价值评价. 影像研究与医学应用. 2024(06): 128-130 .  百度学术
百度学术
2. 李牧,李倩,柯熙政,陶启婷. 基于两阶段运动伪影消除的心率检测算法. 计算机应用. 2023(S1): 333-339 . 百度学术
其他类型引用(1)



















计量
- 文章访问数: 2921
- HTML全文浏览量: 2432
- PDF下载量: 274
- 被引次数: 3


