
The Application Value of CT Lymphangiography in Diagnosis and Grading in Patients with Primary Chyluria
-
摘要: 目的:探讨CT淋巴管成像(CTL)对于原发性乳糜尿患者诊断及分级的应用价值。方法:回顾性收集确诊为原发性乳糜尿的79例患者的临床及CTL影像学资料,CTL指标主要包括:①肾脏受累侧别及肾内淋巴管分布范围:单肾、双肾、肾窦、肾实质及肾门上区、肾门下区;②腹膜后异常淋巴管分布情况:包括腹膜后、腰干区域、肾血管周、肾周脂肪囊、肾上腺区域等;③腹盆部及胸部扩张淋巴管分布及淋巴反流情况;④其他异常表现:包括腹盆部、胸部及骨骼等部位的淋巴管相关异常改变;⑤影像学分级:按照腹膜后累及区域范围进行影像学分级,将腹膜后区域分为左侧和右侧肾门上区、肾门下区、腰干区、肾血管旁区、肾周区等10个区域,累及5个及以内区域为轻度,累及6个及以上区域为重度。根据乳糜尿临床分级标准进行临床分级,对于原发性乳糜尿患者临床特点及CTL征象采用分类变量资料中的构成比进行统计描述,利用一致性Kappa检验评估原发性乳糜尿患者影像分级及临床分级的一致性。结果:79例CTL示肾内异常碘油沉积74例(93.7%),单肾55例(69.6%),双肾19例(24.1%),肾窦74例(93.7%),肾实质37例(46.8%);肾门上区61例(77.2%),其中单侧52例(65.8%),双侧9例(11.4%);肾门下区61例(77.2%),其中单侧47例(59.5%),双侧14例(17.7%);腹膜后78例(98.7%);腰干区域76例(96.2%),其中单侧20例(25.3%),双侧56例(70.9%);肾血管周72例(91.1%),其中单侧45例(57.0%),双侧27例(34.2%);肾周脂肪囊14例(17.7%),其中单侧13例(16.5),双侧1例(1.3%);肾上腺区域12例(15.2%);膀胱内31例(39.2%),膀胱周12例(15.2%),髂血管周73例(92.4%),腹盆壁14例(17.7%),会阴12例(15.2%),直肠周14例(17.7%),肠系膜26例(32.9%),肠壁11例(13.9%),肠管内5例(6.3%),胰腺周15例(18.9%),脾周2例(2.5%),肝周7例(8.8%);肺门1例(1.3%),纵隔14例(17.7%),心包1例(1.3%),胸膜外25例(31.6%),胸壁2例(2.5%),骨骼2例(2.5%),胸导管末端70例(88.6%)。79例原发性乳糜尿患者中,临床分级为轻度27例,重度52例,影像学分级为轻度40例,重度39例,两种分级的一致性中等。结论:CTL能够准确评价原发性乳糜尿患者的肾内及腹膜后扩张淋巴管分布及范围,评估胸腹盆部淋巴管及胸导管异常情况,为原发性乳糜尿的诊断、分级及治疗提供影像依据。Abstract: Objective: To investigate the application value of CT lymphangiography in diagnosis and grading in patients with primary chyluria. Methods: Clinical and CTL imaging data of 79 patients diagnosed with primary chyluria were collected retrospectively. For CTL, the indexs were (1) Involved kidney and distribution of abnormal lymphatic vessels in the kidney: unilateral or bilateral kidney,renal sinus, renal parenchymal, suprahilar area and subhilar area; (2) Distribution of perirenal and retroperitoneal abnormal lymphatic vessels: retroperitoneal area,lumbar trunk area, renal perivascular area, fatty capsule area, adrenal area, etc; (3) Distribution of dilated lymphatic vessels and lymphatic reflux in chest, abdomen and pelvis; (4) Other abnormal manifestations: lymphatic-related abnormal changes in the chest, abdomen, pelvic cavity and bone; (5) Imaging grading: the imaging grading was carried out according to the range of retroperitoneal involvement, and the retroperitoneal area was divided into 10 areas, including left and right suprahilar area, subhilar area, perirenal area, renal perivascular area and lumbar trunk area, involvement of five or fewer areas were graded as mild, while involvement of six or more were graded as severe. In addition, clinical grading was carried out according to clinical manifestations. The clinical characteristics and CTL signs of patients with primary chyluria were statistically described by the composition ratio of classification variables, and the consistency of imaging grade and clinical grade of patients with primary chyluria was evaluated by Kappa test. Results: CTL showed abnormal lipiodol deposition in kidney in 74 cases (93.7%), unilateral kidney in 55 cases (69.6%), bilateral kidneys in 19 cases (24.1%), renal sinus in 74 cases (93.7%), renal parenchyma in 37 cases (46.8%); suprahilar area in 61 cases (77.2%), 52 cases (65.8%) were unilateral and 9 cases (11.4%) were bilateral; subhilar area in 61 cases (77.2%), 47 cases (59.5%) were unilateral and 14 cases (17.7%) were bilateral; retroperitoneal area in 78 cases (98.7%); lumbar trunk area in 76 cases (96.2%), 20 cases (25.3%) were unilateral and 56 cases (70.9%) were bilateral; perivascular area in 72 cases (91.1%), 45 cases (57.0%) were unilateral and 27 cases (34.2%) were bilateral; fatty capsule in 14 cases (17.7%), 13 cases (16.5%) were unilateral and 1 case (1.3%) was bilateral; adrenal area in 12 cases (15.2%); bladder in 31 cases (39.2%), perivesical area in 12 cases (15.2%), iliac perivascular area in 73 cases (92.4%), abdominal and pelvic wall in 14 cases (17.7%), perineal area in 12 cases (15.2%), perirectal area in 14 cases (17.7%), mesentery in 26 cases (32.9%), intestinal wall in 11 cases (13.9%), intestinal canal in 5 cases (6.3%), peripancreatic area in 15 cases (18.9%), perisplenic area in 2 cases (2.5%), perihepatic area in 7 cases (8.8%), hilus of the lung in 1 case (1.3%), mediastinum in 14 cases (17.7%), pericardium in 1 case (1.3%), extrapleural area in 25 cases (31.6%), chest wall in 2 cases (2.5%), skeleton in 2 cases (2.5%), end of thoracic duct in 70 cases (88.6%). Among the 79 patients with primary chyluria, according to clinical classification, 27 cases were mild and 52 cases were severe; according to imaging classification, 40 cases were mild and 39 cases were severe. The consistency of the two grades was moderate. Conclusion: CTL can evaluate the distribution and range of intrarenal, perirenal and retroperitoneal dilated lymphatic vessels accurately, and evaluate the abnormal lymphatic vessels in the chest, abdomen and pelvis and thoracic duct in patients with primary chyluria.It can provide image basis for the diagnosis, grading and treatment of primary chyluria.
-
Keywords:
- tomography /
- X-ray computed /
- primary chyluria /
- direct lymphangiography /
- lymph
-
乳糜尿是指各种原因致乳糜液从淋巴管道进入泌尿集合系统,使尿液中混有乳糜颗粒而呈乳浊色及乳白色的一种罕见症状[1]。乳糜尿根据病因不同分为原发性和继发性,原发性乳糜尿多由先天性淋巴管异常所致[2],继发性乳糜尿多见于寄生虫感染[3]、肿瘤、结核、手术等[4-5]。目前,随着我国丝虫病消除工作的开展,继发性乳糜尿新发病例逐年减少[6],而原发性乳糜尿并不十分少见[2]。近年来,直接淋巴管造影(direct lymphangiography,DLG)、CT淋巴管成像(computed tomography lymphangiography,CTL)、MR淋巴成像(MR lymphography,MRL)、放射性核素淋巴显像(radionuclide lymphoscintigraphy)等多种影像学检查技术应用于乳糜尿的术前诊断[7-8],但是对于评估原发性乳糜尿的肾内、肾周及腹膜后淋巴管扩张的分布情况及严重程度的相关研究鲜有报道[3]。
本研究回顾性收集79例确诊为原发性乳糜尿患者的临床及CTL影像资料,初步探讨CTL对于原发性乳糜尿患者诊断及分级的应用价值。
1. 资料与方法
1.1 一般资料
回顾性分析北京大学第九临床医学院(首都医科大学附属北京世纪坛医院)2011年1月至2021年12月确诊的79例原发性乳糜尿患者,男性31例,女性48例,发病年龄11岁~71岁,平均发病年龄(45.6±19.3)岁,病程范围1月~50年,平均病程10.9年。临床表现包括间断或持续排乳浊色或乳白色尿液79例,伴乳糜凝块37例,血尿和/或血块21例,腰部不适9例,排尿困难15例,尿痛、尿急10例,腹胀或腹泻4例,胸闷或胸痛8例,咳嗽、咳痰1例(表1)。
表 1 79例原发性乳糜尿患者的临床特点Table 1. Clinical characteristics in 79 patients with primary chyluria临床特点 轻度 重度 合计 男性/例(%) 7(8.8) 24(30.4) 31(39.2) 女性/例(%) 20(25.3) 28(35.4) 48(60.8) 发病平均年龄/岁 41.8±18.6 47.6±19.5 45.6±19.3 平均病程/年 5.1 14.0 10.9 乳浊色或乳白色尿液/例(%) 27(34.2) 52(65.8) 79(100.0) 乳糜凝块/例(%) 0(0.0) 37(46.8) 37(46.8) 血尿和/或血块/例(%) 0(0.0) 21(26.6) 21(26.6) 腰部不适/例(%) 0(0.0) 9(11.4) 9(11.4) 排尿困难/例(%) 0(0.0) 15(19.0) 15(19.0) 尿痛、尿急/例(%) 0(0.0) 10(12.7) 10(12.7) 注:构成比为阳性数与患者总数的比值。 入组标准:①临床表现为间断或持续性排乳浊色或乳白色尿,实验室检查尿乳糜试验阳性;②接受 CT淋巴管成像检查。排除标准:①存在寄生虫感染、肿瘤、炎症、结核、手术或创伤等可能导致继发性乳糜尿的因素;②实验室检查提示肾功能异常者;③临床及 CTL影像资料不全者。
根据原发性乳糜尿患者的临床症状进行临床分级。轻度表现为间歇性排乳浊色或乳白色尿,不伴其他任何临床症状;重度表现为间歇或持续性排乳浊色或乳白色尿,伴乳糜凝块和/或血尿,伴或不伴尿潴留及体重减轻。79例原发性乳糜尿患者中,临床分级轻度27例,重度52例。
1.2 检查方法
79例患者均接受CTL检查,检查前告知患者和家属检查内容及检查禁忌症,患者及家属签署知情同意书。
DLG检查。根据患者临床情况,于患者单侧健侧足于第1和第2趾根间皮下注射1~2 mL对比剂(亚甲蓝与2% 利多卡因1∶1混合溶液),寻找分离一支蓝染的浅部淋巴管,以8 mL/h的流率注入8~20 mL碘油,采用GE Innova 2000-IQ DSA机观察碘油回流过程,直至碘油沿着下肢、髂、腰干及胸导管进入左侧静脉角或碘油停止流动时结束检查。
CTL检查。于DLG检查20 min~2 h后采用Siemens Sensation 16 CT、Philips Brilliance iCT或GE Revolution CT进行扫描,扫描范围起自颈部甲状软骨下缘止于耻骨联合下缘。扫描参数设置:管电压80~120 kV,管电流250~300 mA,层厚5 mm,层间隔5 mm,螺距为1。之后进行横断面、冠状面及矢状面重建,层厚2 mm,层间隔1.8 mm,并进行最大密度投影、多平面重组及容积演示等后处理重建。
1.3 图像分析
由两名放射科医师以盲法分别进行CTL影像独立阅片,阅片结果不一致时再由另一位有10年以上影像诊断工作经验的医师指导下得出最终结果。淋巴管迂曲扩张是指异常碘油呈条片状、蚯蚓状或团片状;淋巴反流是指在碘油注入侧的对侧出现异常碘油沉积,例如异常碘油出现在对侧髂淋巴管、腰干、支气管纵隔干、颈干、锁骨下干等位置。
CTL主要征象指标: ①肾脏受累侧别及肾内淋巴管分布范围:单肾、双肾、肾窦、肾实质及肾门上区、肾门下区;肾门上区是指异常碘油沉积于肾门及肾门以上肾窦和/或肾实质内;肾门下区是指异常碘油沉积于肾门及肾门以下肾窦和/或肾实质内。②腹膜后异常淋巴管分布情况:包括腹膜后、腰干区域、肾血管周、肾周脂肪囊、肾上腺区域等。③腹盆部及胸部扩张淋巴管分布及淋巴反流等异常情况:通过异常碘油沉积的形态及分布判断双髂、腰干、盆腔、腹腔、胸部及胸导管等淋巴管异常情况。④其他异常表现:包括腹盆部、胸部及骨骼等淋巴管相关异常改变。⑤影像学分级:按照腹膜后累及区域范围进行影像学分级,将腹膜后区域分为左侧和右侧肾门上区、肾门下区、腰干区域、肾血管旁区、肾周区等10个区域,累及5个及以内区域为轻度,累及6个及以上区域为重度。
1.4 统计学分析
采用SPSS 26.0统计软件,对于原发性乳糜尿患者临床特点及CTL征象采用分类变量资料中的构成比进行统计描述;利用一致性Kappa检验评估临床分级及影像学分级的一致性,Kappa值<0.20为一致性极低,0.20<Kappa值≤0.40为一致性一般,0.40<Kappa值≤0.60为一致性中等,0.60<Kappa值≤0.80为高度一致性,0.80<Kappa值≤1.00为完全一致。设显著性水平P=0.05。
2. 结果
2.1 原发性乳糜尿患者CTL影像表现
(1)原发性乳糜尿患者肾脏及腹膜后CTL影像表现(表2)。CTL示肾内异常碘油沉积74例(93.7%),其中单肾55例(69.6%)(图1),双肾19例(24.1%)(图2),肾窦74例(93.7%)(图1和图3),肾实质37例(46.8%)(图1);肾门上区61例(77.2%),其中单侧52例(65.8%),双侧9例(11.4%);肾门下区61例(77.2%),其中单侧47例(59.5%)(图3),双侧14例(17.7%);腹膜后78例(98.7%)(图2),腰干区域76例(96.2%),其中单侧20例(25.3%),双侧56例(70.9%);肾血管周72例(91.1%),其中单侧45例(57.0%),双侧27例(34.2%)(图2);肾周脂肪囊14例(17.7%),其中单侧13例(16.5%),双侧1例(1.3%);肾上腺区域12例(15.2%)(图1)。
表 2 79例原发性乳糜尿患者的CTL肾脏及腹膜后碘油异常沉积Table 2. CTL abnormal lipiodol deposition in renal and retroperitoneal area of 79 patients with primary chyluria碘油异常沉积 例(%) 肾脏 74(93.7) 单肾 55(69.6) 双肾 19(24.1) 肾窦 74(93.7) 肾实质 37(46.8) 肾门上区 61(77.2) 单侧 52(65.8) 双侧 9(11.4) 肾门下区 61(77.2) 单侧 47(59.5) 双侧 14(17.7) 腹膜后 78(98.7) 腰干区域 76(96.2) 单侧 20(25.3) 双侧 56(70.9) 肾血管周 72(91.1) 单侧 45(57.0) 双侧 27(34.2) 肾周脂肪囊 14(17.7) 单侧 13(16.5) 双侧 1(1.3) 肾上腺区 12(15.2) ![]() 图 1 患者,女,15岁,间断排乳糜尿1年余。CTL冠状面图示左侧肾窦内(白箭)、肾实质内(虚线白箭)及肾上腺区域(黑箭)异常碘油沉积;脾脏内类圆形低密度灶(白三角)Figure 1. A 15-year-old female patient with intermittent chyluria for more than 1 year. The coronal image of CTL shows abnormal lipiodol deposition in the left renal sinus (white arrow),the left renal parenchyma (white dotted arrow) and the left adrenal area (black arrow); a round hypodensity lesion in the spleen(white triangle)
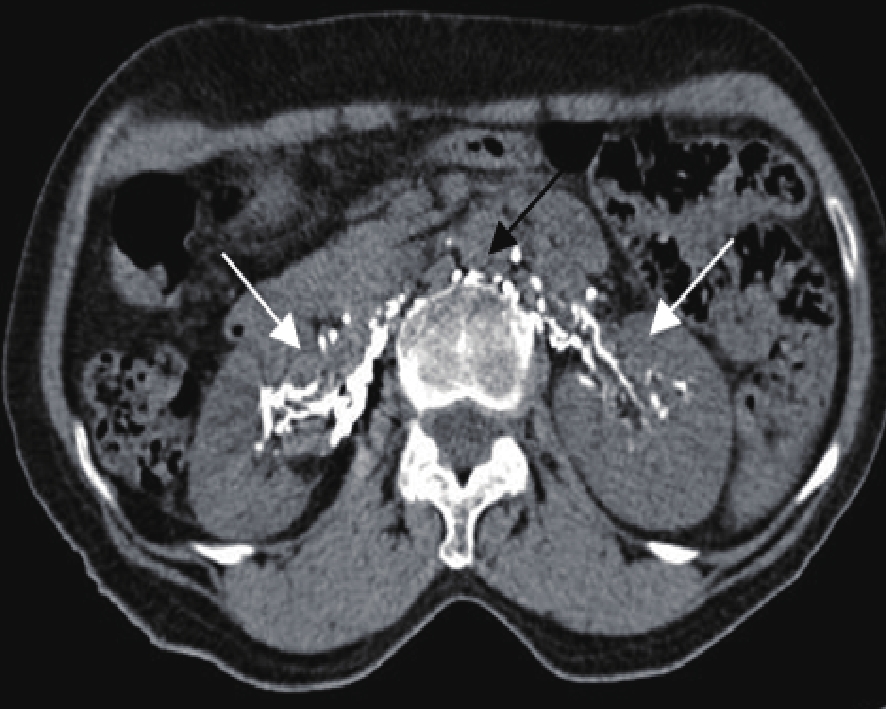
图 1 患者,女,15岁,间断排乳糜尿1年余。CTL冠状面图示左侧肾窦内(白箭)、肾实质内(虚线白箭)及肾上腺区域(黑箭)异常碘油沉积;脾脏内类圆形低密度灶(白三角)Figure 1. A 15-year-old female patient with intermittent chyluria for more than 1 year. The coronal image of CTL shows abnormal lipiodol deposition in the left renal sinus (white arrow),the left renal parenchyma (white dotted arrow) and the left adrenal area (black arrow); a round hypodensity lesion in the spleen(white triangle)![]() 图 2 患者,女,64岁,间断排乳糜尿伴乏力1年8个月。CTL轴面图示腹膜后(黑箭)、双侧肾血管周(白箭)异常碘油沉积Figure 2. A 64-year-old female patient with intermittent chyluria and fatigue for 20 months. The axial image of CTL shows abnormal lipiodol deposition in the retroperitoneal (blacck arrow) and the bilateral renal perivascular area (white arrow)
图 2 患者,女,64岁,间断排乳糜尿伴乏力1年8个月。CTL轴面图示腹膜后(黑箭)、双侧肾血管周(白箭)异常碘油沉积Figure 2. A 64-year-old female patient with intermittent chyluria and fatigue for 20 months. The axial image of CTL shows abnormal lipiodol deposition in the retroperitoneal (blacck arrow) and the bilateral renal perivascular area (white arrow)![]() 图 3 患者,男,75岁,间断排乳糜尿半年。CTL冠状面图示左侧肾门下区肾窦内(白箭)异常碘油沉积Figure 3. A 75-year-old male patient with intermittent chyluria for half a year. The coronal image of CTL shows abnormal lipiodol deposition in the left renal sinus below hilum level (white arrow)
图 3 患者,男,75岁,间断排乳糜尿半年。CTL冠状面图示左侧肾门下区肾窦内(白箭)异常碘油沉积Figure 3. A 75-year-old male patient with intermittent chyluria for half a year. The coronal image of CTL shows abnormal lipiodol deposition in the left renal sinus below hilum level (white arrow)(2)原发性乳糜尿患者腹盆部、胸部、骨骼CTL影像表现(表3):CTL示异常碘油沉积于膀胱内31例(39.2%)(图4),膀胱周12例(15.2%),髂血管周73例(92.4%)(图5),腹盆壁14例(17.7%),会阴12例(15.2%),直肠周14例(17.7%),肠系膜26例(32.9%),肠壁11例(13.9%),肠管内5例(6.3%),胰腺周15例(18.9%),脾周2例(2.5%),肝周7例(8.8%),肺门1例(1.3%),纵隔14例(17.7%)(图6),心包1例(1.3%),胸膜外25例(31.6%),胸壁2例(2.5%),骨骼2例(2.5%),胸导管末端70例(88.6%)。
表 3 79例原发性乳糜尿患者的CTL腹部及胸部碘油异常沉积Table 3. CTL abnormal lipiodol deposition in the thoracic, abdominal and pelvic area of 79 patients with primary chyluria碘油异常沉积 例(%) 腹盆部 膀胱内 31(39.2) 膀胱周 12(15.2) 髂血管周 73(92.4) 腹盆壁 14(17.7) 会阴 12(15.2) 直肠周 14(17.7) 肠系膜 26(32.9) 肠壁 11(13.9) 肠管内 5(6.3) 胰腺周 15(18.9) 脾周 2(2.5) 肝周 7(8.8) 胸部 肺门 1(1.3) 纵隔 14(17.7) 心包 1(1.3) 胸膜外 25(31.6) 胸壁 2(2.5) 骨骼 2(2.5) 胸导管末端 70(88.6) ![]() 图 4 患者,女,28岁,间断排乳糜尿1月余。CTL轴面图示膀胱内(白箭)异常碘油沉积Figure 4. A 28-year-old female patient with intermittent chyluria for more than 1 month. The axial image of CTL shows abnormal lipiodol deposition in the bladder (white arrow)
图 4 患者,女,28岁,间断排乳糜尿1月余。CTL轴面图示膀胱内(白箭)异常碘油沉积Figure 4. A 28-year-old female patient with intermittent chyluria for more than 1 month. The axial image of CTL shows abnormal lipiodol deposition in the bladder (white arrow)![]() 图 5 患者,女,24岁,间断排乳糜尿20年,阴道乳糜瘘10年,伴腹胀1月。CTL冠状面图示腹膜后(白箭)、双髂血管周(黑箭)、子宫及阴道周围(虚线白箭)多发碘油异常沉积;腹腔内液性密度影(白三角)Figure 5. A 24-year-old female patient with intermittent chyluria for 20 years, vaginal chylous fistula for 10 years and abdominal distension for 1 month. The coronal image of CTL shows abnormal lipiodol deposition in the retroperitoneal (white arrow), bilateral iliac perivascular (black arrow), uterine and vaginal area (white dotted arrow); liquid hypodensity in the abdominal cavity (white triangle)
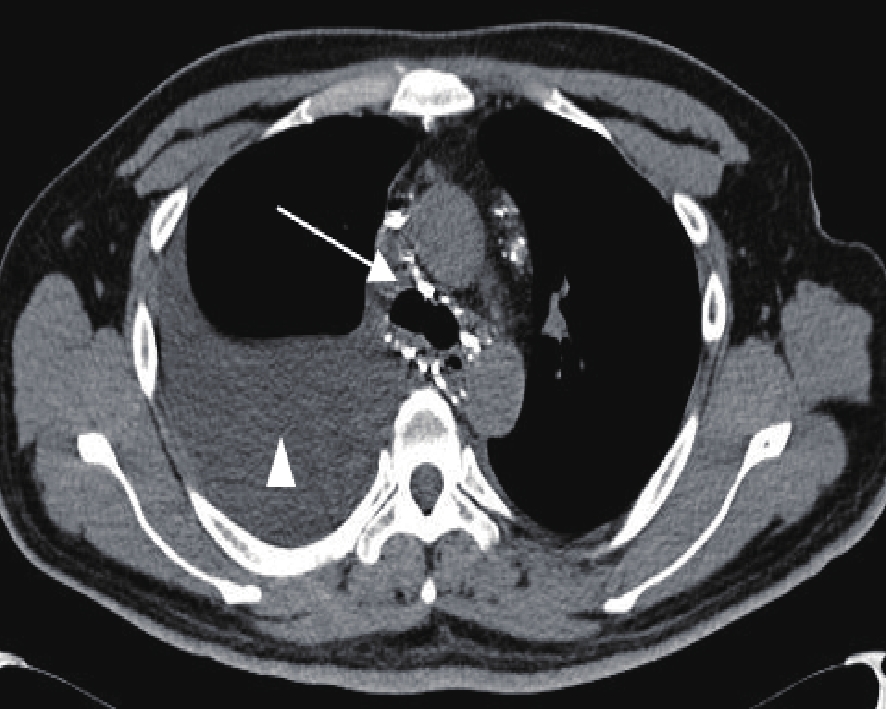
图 5 患者,女,24岁,间断排乳糜尿20年,阴道乳糜瘘10年,伴腹胀1月。CTL冠状面图示腹膜后(白箭)、双髂血管周(黑箭)、子宫及阴道周围(虚线白箭)多发碘油异常沉积;腹腔内液性密度影(白三角)Figure 5. A 24-year-old female patient with intermittent chyluria for 20 years, vaginal chylous fistula for 10 years and abdominal distension for 1 month. The coronal image of CTL shows abnormal lipiodol deposition in the retroperitoneal (white arrow), bilateral iliac perivascular (black arrow), uterine and vaginal area (white dotted arrow); liquid hypodensity in the abdominal cavity (white triangle)![]() 图 6 患者,男,35岁,间断排乳糜尿7年。CTL轴面图示纵隔区域内异常碘油沉积(白箭);胸腔内液性低密度影(白三角)Figure 6. A 35-year-old male patient with intermittent chyluria for 7 years. The axial image of CTL shows abnormal lipiodol deposition in the mediastinal area (white arrow); fluid hypodensity in pleural cavity (white triangle)
图 6 患者,男,35岁,间断排乳糜尿7年。CTL轴面图示纵隔区域内异常碘油沉积(白箭);胸腔内液性低密度影(白三角)Figure 6. A 35-year-old male patient with intermittent chyluria for 7 years. The axial image of CTL shows abnormal lipiodol deposition in the mediastinal area (white arrow); fluid hypodensity in pleural cavity (white triangle)2.2 其他异常表现
本组79例患者CTL还发现15例不同部位囊性淋巴管畸形,其中腹膜后5例,脾脏5例(图1),纵隔2例,骨骼3例,表现为大小不等类圆形、不规则形的囊状低密度影,部分病灶内可见碘油进入;1例腹盆壁淋巴管扩张,表现为迂曲管状稍低密度或软组织密度影,可见大量异常碘油沉积;21例肺部淋巴回流障碍改变,表现为磨玻璃密度病灶和/或蛙卵结节;乳糜性腹腔积液3例(图5),胸腔积液9例(图6),心包积液1例,阴道乳糜瘘2例(图5)。
2.3 原发性乳糜尿CTL影像分级和临床分级的一致性
79例原发性乳糜尿患者中,临床分级为轻度27例,重度52例;影像学分级为轻度40例,重度39例,其中5例CTL影像分级为重度者临床分级为轻度,18例CTL影像分级为轻度者临床分级为重度,两种分级的一致性中等(表4)。
表 4 79例原发性乳糜尿患者的CTL影像分级与临床分级Table 4. CTL image grade and clinical grade of 79 patients with primary chyluria影像分级 临床分级/例(%) 合计/例(%) 统计检验 轻度 重度 Kappa P 轻度 22(27.8) 18(22.8) 40(50.6) 0.420 <0.05 重度 5(6.3) 34(43.0) 39(49.4) 合计 27(34.2) 52(65.8) 79(100.0) 3. 讨论
3.1 原发性乳糜尿临床特点、发病机制及治疗
原发性乳糜尿是指由于淋巴管或胸导管发育异常导致乳糜液进入泌尿集合系统使得尿液混有乳糜微粒的一种淋巴管相关病变[1-3],典型临床表现为尿液呈乳浊色或乳白色,其他临床症状还包括乳糜凝块、血尿、血块、腰痛、尿潴留、营养不良、体重下降、低蛋白血症等[9-10]。本组原发性乳糜尿病例男女比例约为3∶5,与既往文献[11]报道具有差异。
目前,原发性乳糜尿的发病机制尚不十分明确,有研究者[2]认为胸导管末端异常可能是其主要原因,胸导管末端梗阻时,淋巴回流不畅,乳糜液反流至腹膜后及腰干淋巴管,致使淋巴管迂曲扩张,乳糜液进一步反流至肾内淋巴管,经淋巴管-泌尿集合系统异常交通处进入尿液。根据原发性乳糜尿患者的临床严重程度可采用保守治疗、介入治疗及手术治疗[12-15]。
3.2 原发性乳糜尿CTL影像表现
既往文献[3,7]报道,肾内及腹膜后淋巴管异常是原发性乳糜尿的典型CTL影像表现。本组研究CTL示74例(93.7%)肾内异常碘油沉积,其中肾窦内均可见异常碘油沉积,这可能与原发性乳糜尿发病机制有关,有研究者[16]认为原发性乳糜尿患者淋巴管-肾脏集合系统异常交通处可能多位于肾脏肾盏穹窿处;37例(46.8%)异常碘油从肾窦延至肾实质,可能是碘油沿着肾脏内淋巴通路反流至肾实质;78例(98.7%)异常碘油沉积于腹膜后,有文献[17]报道乳糜尿可能是腹膜后淋巴管异常扩张或阻塞所致;72例(91.1%)异常碘油沉积于肾血管周、12例(15.2%)沉积于肾上腺区域,这与张银高等[18]研究结果一致,14例(17.7%)沉积于脂肪囊,这与既往研究[18]结果具有差异。因此,我们认为CTL可以检出肾内、肾周及腹膜后的异常扩张淋巴管分布与范围,对于异常淋巴管结扎或栓塞等手术治疗具有重要指导意义。
本组研究结果表明,原发性乳糜尿患者除肾内、肾周及腹膜后异常碘油沉积外,还可见腹盆部及胸部等多处的淋巴异常反流。此外,21例患者可见肺内淋巴回流障碍改变,15例患者合并乳糜瘘,15例患者合并囊性淋巴管畸形。因此,我们推测原发性乳糜尿可能是一种全身的系统性的淋巴回流障碍性病变,并且部分患者可以合并先天性淋巴管发育不良及瘤样增生。
本组79例原发性乳糜尿患者中有5例CTL未示肾脏内异常碘油沉积,其中2例患者盆腔内多发扩张淋巴管,并且1例合并阴道乳糜瘘,可能是由于盆腔内淋巴管发育异常,大量碘油首先反流至盆腔内扩张淋巴管,而未能进一步向上回流;2例患者胸导管末端梗阻,并可见左侧颈干、锁骨下干多发异常反流,可能是因为胸导管末端多处异常反流降低了胸导管压力,从而碘油未能进一步向下反流沉积至肾脏;另外1例患者左髂淋巴管扩张及胸导管回流受阻,肾脏及其他部位未见明显碘油异常反流,可能是由于胸导管不完全梗阻,少量乳糜液间歇性反流,肾内淋巴管扩张程度低,CTL未示肾内异常碘油沉积。
既往文献[9]根据逆行肾盂造影的肾盏受累数量进行乳糜尿分级。关晓姣等[3]参考此分级方法,提出按照碘油累及肾盏数量进行CTL影像分级,双侧肾脏见1个或2个肾盏存在异常碘油为轻度,2个以上肾盏存在异常碘油为重度,其影像分级结果与临床分级结果的一致性一般,他们认为可能是由于淋巴管-泌尿集合系统异常交通的范围大小之间存在差异。而我们推测也可能是由于多发碘油沉积于肾内扩张淋巴管内,肾盏内碘油沉积难以观察而影响影像分级结果。本研究按照CTL所示腹膜后扩张淋巴管分布区域提出新的影像学分级,本组结果与既往研究结果[3]具有差异,其与临床分级的一致性中等,可能是由于肾内及腹膜后淋巴管扩张程度及分布范围与淋巴管-泌尿集合系统异常交通的程度及范围不相匹配有关。
3.3 本研究局限性
本研究局限性。①对于腹膜后、腰干、肾内、肾周、腹盆部及胸部淋巴管影像缺乏正常淋巴管影像对照;②未能对不同严重程度的原发性乳糜尿的 CTL影像表现进行对比研究;③只关注原发性乳糜尿患者淋巴管异常碘油沉积结果,未能动态评估淋巴回流状态。我们将继续对于以上问题进行研究和探讨。
综上所述,CTL可以通过不同部位的异常碘油沉积推测淋巴管异常形态和回流情况,清晰显示肾内、肾周及腹膜后扩张淋巴管的分布和范围,并且明确异常淋巴管与周围组织结构关系。因此,CTL能够为原发性乳糜尿的诊断、分级提供影像学依据,对于治疗具有重要指导意义。
-
![]()
图 1 患者,女,15岁,间断排乳糜尿1年余。CTL冠状面图示左侧肾窦内(白箭)、肾实质内(虚线白箭)及肾上腺区域(黑箭)异常碘油沉积;脾脏内类圆形低密度灶(白三角)
Figure 1. A 15-year-old female patient with intermittent chyluria for more than 1 year. The coronal image of CTL shows abnormal lipiodol deposition in the left renal sinus (white arrow),the left renal parenchyma (white dotted arrow) and the left adrenal area (black arrow); a round hypodensity lesion in the spleen(white triangle)
![]()
图 2 患者,女,64岁,间断排乳糜尿伴乏力1年8个月。CTL轴面图示腹膜后(黑箭)、双侧肾血管周(白箭)异常碘油沉积
Figure 2. A 64-year-old female patient with intermittent chyluria and fatigue for 20 months. The axial image of CTL shows abnormal lipiodol deposition in the retroperitoneal (blacck arrow) and the bilateral renal perivascular area (white arrow)
![]()
图 3 患者,男,75岁,间断排乳糜尿半年。CTL冠状面图示左侧肾门下区肾窦内(白箭)异常碘油沉积
Figure 3. A 75-year-old male patient with intermittent chyluria for half a year. The coronal image of CTL shows abnormal lipiodol deposition in the left renal sinus below hilum level (white arrow)
![]()
图 4 患者,女,28岁,间断排乳糜尿1月余。CTL轴面图示膀胱内(白箭)异常碘油沉积
Figure 4. A 28-year-old female patient with intermittent chyluria for more than 1 month. The axial image of CTL shows abnormal lipiodol deposition in the bladder (white arrow)
![]()
图 5 患者,女,24岁,间断排乳糜尿20年,阴道乳糜瘘10年,伴腹胀1月。CTL冠状面图示腹膜后(白箭)、双髂血管周(黑箭)、子宫及阴道周围(虚线白箭)多发碘油异常沉积;腹腔内液性密度影(白三角)
Figure 5. A 24-year-old female patient with intermittent chyluria for 20 years, vaginal chylous fistula for 10 years and abdominal distension for 1 month. The coronal image of CTL shows abnormal lipiodol deposition in the retroperitoneal (white arrow), bilateral iliac perivascular (black arrow), uterine and vaginal area (white dotted arrow); liquid hypodensity in the abdominal cavity (white triangle)
![]()
图 6 患者,男,35岁,间断排乳糜尿7年。CTL轴面图示纵隔区域内异常碘油沉积(白箭);胸腔内液性低密度影(白三角)
Figure 6. A 35-year-old male patient with intermittent chyluria for 7 years. The axial image of CTL shows abnormal lipiodol deposition in the mediastinal area (white arrow); fluid hypodensity in pleural cavity (white triangle)
表 1 79例原发性乳糜尿患者的临床特点
Table 1 Clinical characteristics in 79 patients with primary chyluria
临床特点 轻度 重度 合计 男性/例(%) 7(8.8) 24(30.4) 31(39.2) 女性/例(%) 20(25.3) 28(35.4) 48(60.8) 发病平均年龄/岁 41.8±18.6 47.6±19.5 45.6±19.3 平均病程/年 5.1 14.0 10.9 乳浊色或乳白色尿液/例(%) 27(34.2) 52(65.8) 79(100.0) 乳糜凝块/例(%) 0(0.0) 37(46.8) 37(46.8) 血尿和/或血块/例(%) 0(0.0) 21(26.6) 21(26.6) 腰部不适/例(%) 0(0.0) 9(11.4) 9(11.4) 排尿困难/例(%) 0(0.0) 15(19.0) 15(19.0) 尿痛、尿急/例(%) 0(0.0) 10(12.7) 10(12.7) 注:构成比为阳性数与患者总数的比值。  下载: 导出CSV
下载: 导出CSV
表 2 79例原发性乳糜尿患者的CTL肾脏及腹膜后碘油异常沉积
Table 2 CTL abnormal lipiodol deposition in renal and retroperitoneal area of 79 patients with primary chyluria
碘油异常沉积 例(%) 肾脏 74(93.7) 单肾 55(69.6) 双肾 19(24.1) 肾窦 74(93.7) 肾实质 37(46.8) 肾门上区 61(77.2) 单侧 52(65.8) 双侧 9(11.4) 肾门下区 61(77.2) 单侧 47(59.5) 双侧 14(17.7) 腹膜后 78(98.7) 腰干区域 76(96.2) 单侧 20(25.3) 双侧 56(70.9) 肾血管周 72(91.1) 单侧 45(57.0) 双侧 27(34.2) 肾周脂肪囊 14(17.7) 单侧 13(16.5) 双侧 1(1.3) 肾上腺区 12(15.2)
下载: 导出CSV
表 3 79例原发性乳糜尿患者的CTL腹部及胸部碘油异常沉积
Table 3 CTL abnormal lipiodol deposition in the thoracic, abdominal and pelvic area of 79 patients with primary chyluria
碘油异常沉积 例(%) 腹盆部 膀胱内 31(39.2) 膀胱周 12(15.2) 髂血管周 73(92.4) 腹盆壁 14(17.7) 会阴 12(15.2) 直肠周 14(17.7) 肠系膜 26(32.9) 肠壁 11(13.9) 肠管内 5(6.3) 胰腺周 15(18.9) 脾周 2(2.5) 肝周 7(8.8) 胸部 肺门 1(1.3) 纵隔 14(17.7) 心包 1(1.3) 胸膜外 25(31.6) 胸壁 2(2.5) 骨骼 2(2.5) 胸导管末端 70(88.6)
下载: 导出CSV
表 4 79例原发性乳糜尿患者的CTL影像分级与临床分级
Table 4 CTL image grade and clinical grade of 79 patients with primary chyluria
影像分级 临床分级/例(%) 合计/例(%) 统计检验 轻度 重度 Kappa P 轻度 22(27.8) 18(22.8) 40(50.6) 0.420 <0.05 重度 5(6.3) 34(43.0) 39(49.4) 合计 27(34.2) 52(65.8) 79(100.0)
下载: 导出CSV
-
[1] WANG Y C, WU C C. Chyluria[J]. Nephrology (Carlton), 2014, 19(3): 172. doi: 10.1111/nep.12180
[2] 信建峰, 孙宇光, 夏松, 等. 直接淋巴管造影术在原发性乳糜尿诊断中的应用[J]. 中华医学杂志, 2013,93(28): 2212−2214. doi: 10.3760/cma.j.issn.0376-2491.2013.28.010 XIN J F, SUN Y G, XIA S, et al. Application of direct lymphangiography in the diagnosis of primary chyluria[J]. National Medical Journal of China, 2013, 93(28): 2212−2214. (in Chinese). doi: 10.3760/cma.j.issn.0376-2491.2013.28.010
[3] 关晓姣, 沈文彬, 信建峰, 等. 特发性乳糜尿患者直接淋巴管造影后CT表现[J]. 中国医学影像技术, 2022,38(3): 388−391. doi: 10.13929/j.issn.1003-3289.2022.03.016 GUAN X J, SHEN W B, XIN J F, et al. Post-direct lymphangiography CT findings in patients with idiopathic chyluria[J]. Chinese Journal of Medical Imaging Technology, 2022, 38(3): 388−391. (in Chinese). doi: 10.13929/j.issn.1003-3289.2022.03.016
[4] DEV N, KUMAR R. Chyluria: A rare initial manifestation of disseminated tuberculosis[J]. International Journal of Mycobacteriology, 2018, 7(3): 282−284. doi: 10.4103/ijmy.ijmy_101_18
[5] ASSAKER R, El HASBANI G, VARGAS J, et al. Trans-urethral resection of bladder tumor (TURBT) and radiofrequency ablation of renal tumor: Rare etiologies of chyluria[J]. Radiology Case Reports, 2020, 15(9): 1579−1583. doi: 10.1016/j.radcr.2020.06.007
[6] 张开仁, 王锐, 瞿宾雁. 湘西自治州慢性丝虫病关怀照料364例患者临床特征分析[J]. 实用预防医学, 2020,27(4): 460−462. [7] 董健, 信建峰, 霍萌, 等. 直接淋巴管造影和CT淋巴管成像在乳糜尿中的诊断价值[J]. 临床放射学杂志, 2018,37(5): 798−802. doi: 10.13437/j.cnki.jcr.2018.05.020 DONG J, XIN J F, HUO M, et al. Direct Lymphangiography with Sequential CT lymphangiography in chyluria: A retrospective study[J]. Journal of Clinical Radiology, 2018, 37(5): 798−802. (in Chinese). doi: 10.13437/j.cnki.jcr.2018.05.020
[8] 孔令, 岳云龙, 左利利, 等. 非增强MR淋巴成像与直接淋巴管造影术后CT定位乳糜尿患者淋巴管-泌尿系瘘道与胸导管异常[J]. 中国医学影像技术, 2020,36(5): 707−711. KONG L, YUE Y L, ZUO L L, et al. Unenhanced MR lymphograghy and CT after direct lymphangiography for locating lympho-urinary fistula and duct abnormalities in patients with chyluria[J]. Chinese Journal of Medical Imaging Technology, 2020, 36(5): 707−711. (in Chinese).
[9] PURKAIT B, GARG G, SINGH M, et al. Chyluria in pregnancy: Etiology, diagnosis, and management perspective[J]. Saudi Journal of Kidney Diseases and Transplantation, 2019, 30(2): 309−314. doi: 10.4103/1319-2442.256837
[10] GUTTILLA A, BELTRAMI P, BETTIN L, et al. Non-parasitic chyluria: Our experience with sclerotherapy with solution of povidone-iodine and destrose and a review of the literature[J]. Urology Case Reports, 2016, 8: 28−30. doi: 10.1016/j.eucr.2016.05.010
[11] 于江, 金讯波. 乳糜尿: 现状及诊治进展[J]. 泌尿外科杂志(电子版), 2018,10(2): 55−59. [12] ZHANG T, WANG J, YU D, et al. It is unnecessary to completely mobilize the kidney in retroperitoneoscopic renal pedicle lymphatic disconnection for intractable chyluria[J]. International Urology and Nephrology, 2016, 48(10): 1565−1569. doi: 10.1007/s11255-016-1351-7
[13] SIVASHANKAR M, NANDASENA A C N. A patient with milky urine: Nonparasitic chyluria and silver nitrate sclerotherapy[J]. Case Reports in Urology, 2020: 8853473.
[14] YADAV P K, SWAIN S, SINGH A, et al. Single-dose instillation of povidone iodine for chyluria: A safe and effective therapy[J]. Urology Annals, 2021, 13(1): 36−40. doi: 10.4103/UA.UA_159_19
[15] ZHANG Y D, CAO R F, JIANG Z J. The approach of retroperitoneal laparoscopic partial dissection of adipose renal capsule plus ligation of renal pedicle lymphatic vessels to the treatment of chyluria[J]. European Review for Medical and Pharmacological Sciences, 2016, 20(24): 5033−5036.
[16] TRIFFONI-MELO A T, DIEZ-GARCIA R W, BARROS SILVA G E, et al. Good response of low-fat/high-protein diet in a patient with chyluria[J]. Renal Failure, 2014, 36(3): 453−456. doi: 10.3109/0886022X.2013.865485
[17] ABEYGUNASEKERA A M, SUTHARSHAN K, BALAGOBI B. New developments in chyluria after global programs to eliminate lymphatic filariasis[J]. International Journal of Urology, 2017, 24(8): 582−588. doi: 10.1111/iju.13378
[18] 张银高, 王行环, 曾俊, 等. 乳糜尿肾周淋巴管分布规律及临床意义[J]. 中华实验外科杂志, 2014,31(7): 1597−1600. doi: 10.3760/cma.j.issn.1001-9030.2014.07.073 ZHANG Y G, WANG X H, ZENG J, et al. The distribution and clinic relevance of lymphatic vessels in the perinephric space of patients with chyluria[J]. Chinese Journal of Experimental Surgery, 2014, 31(7): 1597−1600. (in Chinese). doi: 10.3760/cma.j.issn.1001-9030.2014.07.073




计量
- 文章访问数: 262
- HTML全文浏览量: 140
- PDF下载量: 17


