
In Vivo Study of the Influence of CT Acquisition and Reconstruction Parameters on Chest CT Number
-
摘要: 目的:探讨不同扫描参数及重建算法对在体胸部各组织CT值的影响。方法:在不同CT扫描条件下测量人体胸部的气管、血管、肺、椎体与肌肉的CT值。分别设定6组不同扫描参数及重建算法:S1层厚5 mm、50%多模型自适应迭代重建技术(ASIR-V)、低剂量;S2层厚5 mm、滤波反投影(FBP)、常规剂量;S3层厚1.25 mm、50%ASIR-V、低剂量;S4层厚1.25 mm、50% ASIR-V、常规剂量;S5层厚1.25 mm、FBP、低剂量;S6层厚1.25 mm、FBP、常规剂量。扫描的辐射剂量采用两种噪声指数(NI)来进行控制,包括低剂量(NI=40)和常规剂量(NI=10)。采用t检验或秩和检验分析比较不同的两个组之间 CT值的差异。结果:扫描剂量仅对气管CT值的影响具有统计学意义,对其他组织CT值无影响;扫描层厚与重建算法对胸部各个组织CT值的影响均未见统计学差异。结论:人体胸部组织CT值受CT层厚、重建算法和CT剂量的影响小,具有良好的稳定性。Abstract: Objective: To explore the influence of different CT acquisition and reconstruction parameters on the CT number of the chest in vivo. Methods: The CT number of the trachea, blood vessels, lungs, vertebral bodies, and muscles of the human chest were measured under different CT scanning parameters. Six groups of different scanning parameters and reconstruction algorithms were set respectively: slice thickness 5 mm, 50% multi-model adaptive statistical iterative reconstruction Veo (ASIR-V) and low-dose for S1; slice thickness 5 mm, filtered back projection (FBP) and standard-dose for S2; slice thickness 1.25 mm, 50% ASIR-V and low-dose for S3; slice thickness 1.25 mm, 50% ASIR-V and standard-dose for S4; slice thickness 1.25 mm, FBP, low-dose for S5; slice thickness 1.25 mm, FBP, standard-dose for S6. The radiation dose of the scan was controlled using two noise indexes (NI), including low-dose (NI=40) and standard-dose (NI=10). Differences in CT number between two groups were compared using t-test or rank-sum test. Results: Significant differences of CT number of the trachea were detected between low-dose and standard-dose, but no significant differences of CT number of other tissues were detected between low-dose and standard-dose. No significant differences of CT number of chest tissues were detected between either 5 mm thickness and 1.25 mm thickness or 50% ASIR-V and FBP. Conclusion: The CT number of human chest tissues showed well stability which was scarcely influenced by slices thickness, reconstruction algorithm and scan dose.
-
Keywords:
- CT scan parameters /
- reconstruction algorithms /
- CT number /
- scan dose
-
-
![]()
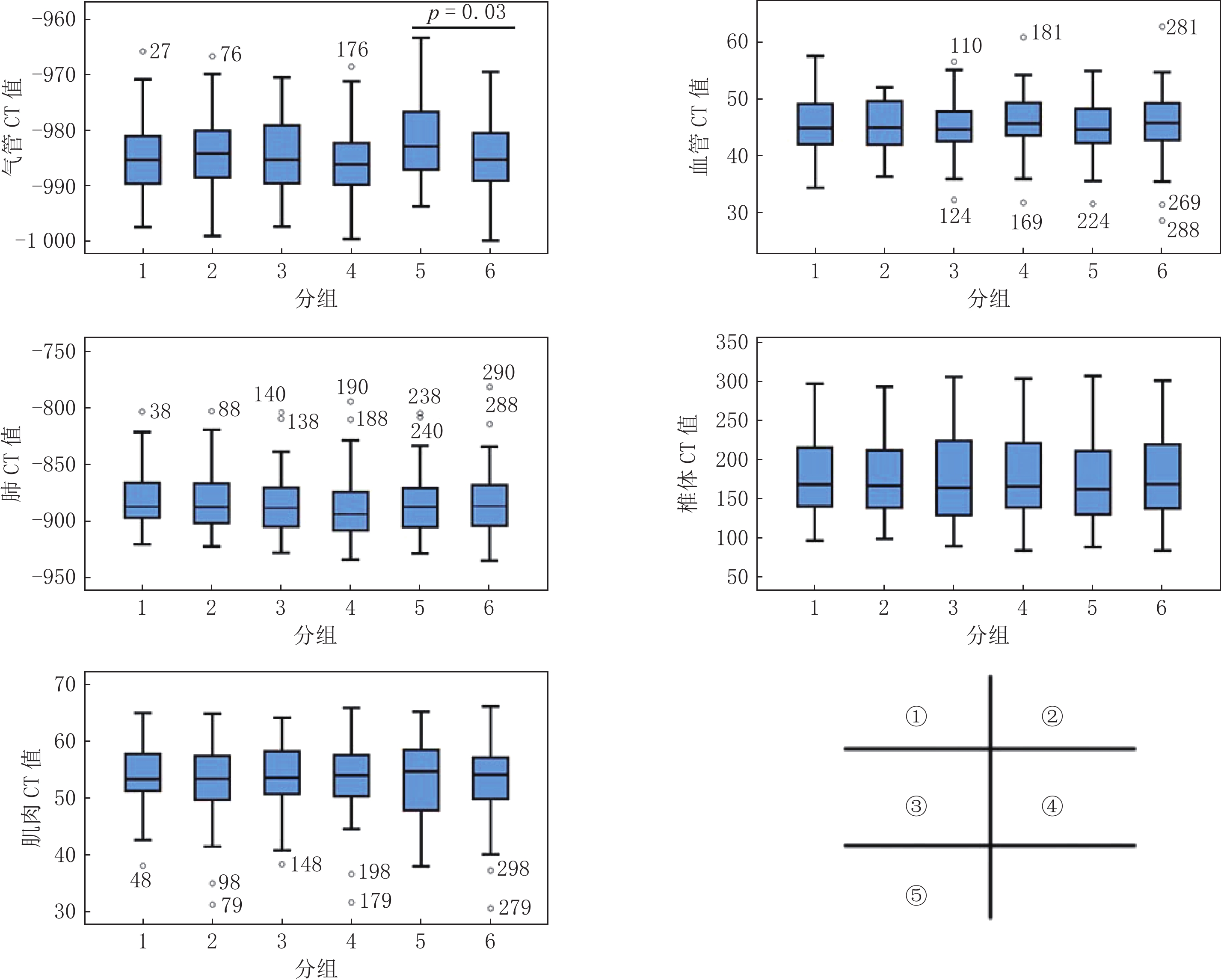
图 1 不同胸部组织在不同序列CT值分布
①气管 CT值在1-6序列中的分布,②血管 CT值在1-6序列中的分布,③肺 CT值在1-6序列中的分布,④椎体 CT值在1-6序列中的分布,⑤肌肉 CT值在1-6序列中的分布;通过对CT值两两比较,发现气管CT值在S5与S6两组的差异具有统计学意义,余各组织各序列相互比较均未见显著统计学差异。
Figure 1. Distribution of CT number measured in different sequences of each tissue
表 1 胸部CT扫描参数及重建方法
Table 1 Chest CT Scanning and reconstruction parameters
序列号 层厚/mm 重建算法 辐射剂量 S1 5.00 50% ASIR-V 低剂量 S2 5.00 FBP 常规剂量 S3 1.25 50% ASIR-V 低剂量 S4 1.25 50% ASIR-V 常规剂量 S5 1.25 FBP 低剂量 S6 1.25 FBP 常规剂量  下载: 导出CSV
下载: 导出CSV
表 2 两名研究者测量CT值一致性检验
Table 2 Interobserver variability test of CT number measured by two doctors
项目 ICC 95% CI F P S1-气管CT值 0.90 0.83~0.94 19.05 <0.001 S2-气管CT值 0.75 0.59~0.85 6.85 <0.001 S3-气管CT值 0.95 0.91~0.97 39.26 <0.001 S4-气管CT值 0.93 0.87~0.96 25.72 <0.001 S5-气管CT值 0.68 0.49~0.80 5.19 <0.001 S6-气管CT值 0.64 0.44~0.78 4.58 <0.001 S1-血管CT值 0.96 0.93~0.97 23.42 <0.001 S2-血管CT值 0.85 0.74~0.92 6.78 <0.001 S3-血管CT值 0.83 0.71~0.91 6.03 <0.001 S4-血管CT值 0.89 0.80~0.94 8.95 <0.001 S5-血管CT值 0.85 0.73~0.91 6.46 <0.001 S6-血管CT值 0.84 0.71~0.91 6.14 <0.001 S1-肺CT值 0.73 0.52~0.84 3.61 <0.001 S2-肺CT值 0.91 0.84~0.95 11.13 <0.001 S3-肺CT值 0.92 0.86~0.96 12.65 <0.001 S4-肺CT值 0.81 0.66~0.89 5.16 <0.001 S5-肺CT值 0.91 0.84~0.95 10.75 <0.001 S6-肺CT值 0.93 0.88~0.96 118.26 <0.001 S1-椎体CT值 0.99 0.96~0.99 118.26 <0.001 S2-椎体CT值 0.98 0.97~0.99 55.34 <0.001 S3-椎体CT值 0.90 0.83~0.95 10.75 <0.001 S4-椎体CT值 0.90 0.81~0.94 9.26 <0.001 S5-椎体CT值 0.93 0.88~0.96 15.17 <0.001 S6-椎体CT值 0.88 0.78~0.93 8.03 <0.001 S1-肌肉CT值 0.84 0.72~0.91 6.23 <0.001 S2-肌肉CT值 0.87 0.77~0.93 7.77 <0.001 S3-肌肉CT值 0.75 0.56~0.86 3.99 <0.001 S4-肌肉CT值 0.88 0.79~0.93 8.47 <0.001 S5-肌肉CT值 0.80 0.64~0.88 4.90 <0.001 S6-肌肉CT值 0.88 0.79~0.93 8.37 <0.001
下载: 导出CSV
表 3 各部位不同序列测量CT值的分布情况
Table 3 Distribution of CT number measured in different sequences of each tissue
序列 气管 血管 肺 椎体 肌肉 S1 -985.15±7.11 45.58±5.00 -887.22(-897.64~-865.48) 168.44(140.10~215.58) 53.57±5.85 S2 -983.95±7.11 41.94(44.98~49.66) -887.48(-902.30~-866.45) 166.67(138.18~214.14) 53.40(49.62~57.46) S3 -984.57±7.03 44.84±4.80 -884.84±27.11 177.88±50.97 53.83±6.09 S4 -985.93±6.49 45.58±5.41 -893.63(-908.19~-872.49) 178.76±51.34 138.60(165.74~221.41) S5 -981.90±6.81 45.11±4.78 -884.07±28.33 162.20(129.89~213.69) 53.58±6.57 S6 -984.89±6.54 45.52±6.01 -884.09±30.24 179.34±52.86 54.14(49.78~57.23)
下载: 导出CSV
表 4 胸部各组织不同序列CT值比较
Table 4 Comparison of different sequence CT values of chest tissues
组织 S1 vs S3 S2 vs S6 S3 vs S4 S5 vs S6 S3 vs S5 S4 vs S6 z/t P z/t P z/t P z/t P z/t P z/t P 气管 -0.41 0.68 0.69 0.49 1.00 0.32 2.23 0.03 -1.93 0.06 -0.80 0.43 血管 0.75 0.46 -0.72 0.47 -0.98 0.33 -0.38 0.70 -0.28 0.78 0.29 0.78 肺 -0.64 0.52 -0.43 0.66 -0.61 0.54 0.00 >0.99 -0.14 0.89 -0.44 0.66 椎体 0.05 0.96 -0.06 0.95 -0.09 0.93 -0.38 0.70 -0.26 0.79 -0.06 0.96 肌肉 -0.21 0.83 -0.29 0.77 -0.18 0.86 -0.38 0.71 0.19 0.85 -0.11 0.91
下载: 导出CSV
-
[1] National Lung Screening Trial Research Team, ABERLE D R, ADAMS A M, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening[J]. The New England Journal of Medicine, 2011, 365(5): 395−409. doi: 10.1056/NEJMoa1102873
[2] HANSELL D M, BANKIER A A, MacMAHON H, et al. Fleischner society: Glossary of terms for thoracic imaging[J]. Radiology, 2008, 246(3): 697−722. doi: 10.1148/radiol.2462070712
[3] GODOY M C, NAIDICH D P. Subsolid pulmonary nodules and the spectrum of peripheral adenocarcinomas of the lung: Recommended interim guidelines for assessment and management[J]. Radiology, 2009, 253(3): 606−622. doi: 10.1148/radiol.2533090179
[4] 李琼, 于红, 张丽, 等. 迭代重建技术对低管电压胸部CT增强扫描图像质量的影响[J]. 实用放射学杂志, 2012,28(10): 1615−1618. doi: 10.3969/j.issn.1002-1671.2012.10.033 LI Q, YU H, ZHANG L, et al. The effect of iterative reconstruction on image quality of contrast-enhanced chest CT with low tube voltage settings[J]. Journal of Practical, 2012, 28(10): 1615−1618. (in Chinese). doi: 10.3969/j.issn.1002-1671.2012.10.033
[5] 彭文献, 彭天舟, 夏顺仁, 等. X线管电压对生物组织CT值影响的实验研究[J]. 放射学实践, 2013,28(11): 1102−1104. PENG W X, PENG T Z, XIA S R, et a1. The effects of X-ray tube voltage on tissue CT value[J]. Radiologic Practice, 2013, 28(11): 1102−1104. (in Chinese).
[6] 彭文献, 彭天舟, 叶小琴, 等. CT扫描参数对人体组织CT值影响的研究[J]. 中华放射医学与防护杂志, 2010,30(1): 79−81. doi: 10.3760/cma.j.issn.0254-5098.2010.01.026 PENG W X, PENG T Z, YE X Q, et al. Effect of CT scanning parameters on CT number[J]. Chinese Journal of Radiological Medicine and Protection, 2010, 30(1): 79−81. (in Chinese). doi: 10.3760/cma.j.issn.0254-5098.2010.01.026
[7] 赵雷, 刘波. 重建算法及射束硬化伪影对CT值测量的影响[J]. 影像研究与医学应用, 2019,3(14): 88−90. [8] 韩萍, 于春水, 余永强, 等. 医学影像诊断学[M]. 4版. 北京: 人民卫生出版社, 2017: 4-5. [9] 朱明, 刘贵霞, 李敬玉. CT扫描参数对CT值影响因素的实验研究[J]. 中国中西医结合影像学杂志, 2017,15(4): 91−93. doi: 10.3969/j.issn.1672-0512.2017.04.029 [10] AOKAGE K, MIYOSHI T, ISHII G, et al. Clinical and pathological staging validation in the eighth edition of the TNM classification for lung cancer: Correlation between solid size on thin-section computed tomography and invasive size in pathological findings in the new T classification[J]. Journal of Thoracic Oncology, 2017, 12(9): 1403−1412. doi: 10.1016/j.jtho.2017.06.003
[11] HENSCHKE C I, YIP R, SMITH J P, et al. CT screening for lung cancer: Part-solid nodules in baseline and annual repeat rounds[J]. American Journal of Roentgenology, 2016, 207(6): 1176−1184. doi: 10.2214/AJR.16.16043
[12] YANKELEVITZ D F, YIP R, SMITH J P, et al. CT screening for lung cancer: Nonsolid nodules in baseline and annual repeat rounds[J]. Radiology, 2015, 277(2): 555−64. doi: 10.1148/radiol.2015142554
[13] 张丽, 吴宁, 李蒙, 等. Ⅰ期浸润性肺腺癌磨玻璃成分定量分析与附壁样生长的相关性研究[J]. 中华肿瘤杂志, 2017,39(4): 269−273. doi: 10.3760/cma.j.issn.0253-3766.2017.04.006 ZHANG L, WU N, LI M, et al. The correlation study of ground glass opacity and lepidic growth pattern component in stage I lung invasive adenocarcinoma[J]. Chinese Journal of Oncology, 2017, 39(4): 269−273. (in Chinese). doi: 10.3760/cma.j.issn.0253-3766.2017.04.006
[14] GAO C, LI J, WU L, et al. The natural growth of subsolid nodules predicted by quantitative initial CT features: A systematic review[J]. Frontiers in Oncology, 2020: 10318.
[15] 蒋宇, 贾晓民, 赵杰. 肺亚实性结节CT定量分析对肺腺癌病理侵袭性诊断价值[J]. 放射学实践, 2021,36(10): 1232−1237. doi: 10.13609/j.cnki.1000-0313.2021.10.007 JIANG Y, JIA X M, ZHAO J. Diagnostic value of quantitative CT analysis of pulmonary subsolid nodules to lung adenocarcinoma[J]. Radiologic Practice, 2021, 36(10): 1232−1237. (in Chinese). doi: 10.13609/j.cnki.1000-0313.2021.10.007
-
期刊类型引用(13)
1. 李腾飞,李俊霞. 良恶性肺结节鉴别诊断中CT引导下经皮肺穿刺活检的应用价值. 黑龙江医药科学. 2025(03): 173-175 .  百度学术
百度学术
2. 陈晓雪,李可峰,韩海森,李依明. CT能谱成像参数联合血清细胞角蛋白19片段抗原21-1水平对孤立性肺结节性质的鉴别诊断价值. 实用心脑肺血管病杂志. 2024(09): 95-98 . 百度学术
3. 陈光耀. CT引导下肺结节术前穿刺定位及穿刺活检并发症及风险因素探讨. 影像研究与医学应用. 2023(03): 194-196 . 百度学术
4. 张洁,王金萍,李保启,胡恩庆. 超声造影联合穿刺活检在胸部占位性病变诊断中的价值. 安徽医学. 2023(05): 541-543 . 百度学术
5. 张知远,李知慧,郑若娟. CT引导下同轴针穿刺活检与常规活检术在胸部肿瘤活检中的应用比较. 现代实用医学. 2023(12): 1575-1578 . 百度学术
6. 唐涌通,徐积兰,李小勇,章俊,陈庆乐,阳名华. 应用激光定位仪联合CT三维图像引导下同轴法对疑似肺癌病灶经皮肺穿刺活检术的研究. 赣南医学院学报. 2022(02): 174-176 . 百度学术
7. 杨国富. CT引导下肺结节术前穿刺定位及穿刺活检并发症及风险因素分析. 影像研究与医学应用. 2022(08): 194-196 . 百度学术
8. 苏海波. 低剂量螺旋CT扫描于肺结节诊断中的应用. 影像研究与医学应用. 2022(12): 153-155 . 百度学术
9. 孙维东,葛金梅,穆小飞,陈竹君,蔡晓敏. 双源CT低剂量引导下同轴活检针在经皮肺穿刺活检中的临床应用研究. 影像研究与医学应用. 2021(05): 194-195 . 百度学术
10. 周广新,刘晓真,许宇光,杨坤,汤庆. 经皮超声引导下肺周围型病变同轴穿刺活检联合超声造影的诊断准确性和并发症发生率. 中国医师杂志. 2021(06): 822-825 . 百度学术
11. 王广鑫. CT定位下经皮肺穿刺活检在肺结核鉴别诊断中的运用. 影像研究与医学应用. 2021(11): 84-85 . 百度学术
12. 王建. 小视野扫描方法在肺小结节CT引导下经皮穿刺活检中的应用效果. 临床医学研究与实践. 2021(21): 131-133 . 百度学术
13. 赵庆成,刘海军. CT引导下经皮肺穿刺活检在肺小结节临床诊治中的应用价值. 实用医技杂志. 2021(12): 1447-1449 . 百度学术
其他类型引用(0)
计量
- 文章访问数:
- HTML全文浏览量:
- PDF下载量:
- 被引次数: 13


