
Application Value of Segond Fracture Imaging Features in Lateral Knee Instability
-
摘要:
目的:评价Segond骨折的影像学特征并探讨其在膝关节外侧不稳中的临床应用价值。方法:回顾性分析45例临床影像诊断为胫骨平台外缘撕脱骨折(Segond骨折)的病例,分析骨折的特点,包括骨折与膝关节周围韧带、半月板损伤的关系、骨折块的大小、位置,探讨Segond骨折对临床治疗的意义。结果:45例Segond骨折中有41例(91.11%)合并前交叉韧带(ACL)损伤,31例(68.89%)合并前外侧韧带(ALL)损伤,12例(26.67%)合并髂胫束(ITB)损伤。ALL全部附着于骨折块上,ITB附着25例(55.55%)。骨折块体积越大、与Gerdy结节中心的距离越小,ITB附着折块的可能性就越大。结论:Segond骨折常合并ACL损伤、累及ALL、ITB,骨折块越大、距Gerdy结节中心越近累及ITB的可能性就越大,Segond骨折患者应警惕膝关节外侧不稳。
Abstract:Objective: To evaluate the imaging features of the Segond fracture and explore its clinical value in lateral instability of the knee joint. Methods: We retrospectively analyzed 45 cases of the Segond fracture. This involved the analysis of the characteristics of the fracture, including the relationship between the fracture and the ligaments around the knee joint, meniscus injury, and the size and location of the fracture block. Moreover, the significance of the Segond fracture in clinical treatment was discussed. Results: Among 45 cases of the Segond fracture, 41 (91.11%) had anterior cruciate ligament (ACL) injury, 31 (68.89%) had anterolateral ligament (ALL) injury, and 12 (26.67%) had iliotibial bundle (ITB) injury. The ALL were all attached to the fracture block, and 25 cases (55.55%) were attached to the ITB. The larger the size of the fracture block and the smaller the distance from the center of Gerdy's nodule, the more likely that the fracture block was attached to the ITB. Conclusion: The Segond fracture is often associated with ACL injury, involving the ALL and ITB. The larger the fracture block and the closer to the center of Gerdy's nodule, the greater the possibility of ITB involvement. Therefore, patients with Segond fractures should be alert to lateral instability of the knee joint.
-
Keywords:
- magnetic resonance imaging /
- knee joint /
- anterolateral ligament /
- injury
-
在我国当前城市地区快速建设的大背景下,机场、地铁等大型基础设施的建设越来越多。建设中由于场地地形、地基土体土质条件不能满足工程地基要求,常常需要对工程场地进行挖填方及地基压实加固处理[1]。这些地基土体处理恰当与否,不仅影响施工的进度,而且将直接影响建筑物的使用性能和工程质量[2]。因此需对地基土体加固质量进行评价,以满足地基强度、变形、动力稳定性要求,从而达到减小地基在上覆荷载作用下引起的沉降或不均匀沉降的目的[3]。
传统的地基土体加固质量的评价指标主要有地基承载力、地基土体变形模量、地基土体压实系数等[4]。地基承载力、地基土体变形模量等参数的测定的主要方法是原位载荷试验,所需试验设备笨重、试验耗时,最突出的特点是对地基的检测是“点”测,很难满足大面积地基处理质量快速检测的需要,也不可能对地基土体展开连续检测;地基土体压实系数方法主要有原位灌砂法和土样测试等方法[5],这些方法需要对地基土体开挖或取样,会对已经加固的地基土体造成破坏。因此急需突破上述方法的局限,实现对地基土体压实质量的快速检测和空间分布均匀性的连续测定。
理论分析和实际测试都表明,岩土体的弹性波速与物理力学性质密切相关[6-7]。考虑某大型工程大面积水塘填筑地基质量控制的需求,本文以瑞雷波相速度VR与岩土体物理力学性质的相关性为基础[8],实现地基压实程度和地基处理效果均匀性两方面的检测。
首先,采用考虑道间时差相位的多道瞬态瑞雷波探测方法(multichannel method of transient Rayleigh wave detecting in consideration of arrival time difference phase between channels,简称TDP法)[9]对填方地基土体进行快速的连续覆盖探测,获得填方地基土体一定深度范围内的瑞雷波相速度三维成像;同时,按照一定的控制密度在填方地基范围内布置土体抽样点,通过土体抽样测试得到的填方地基土体压实系数;进而利用同一抽样点上土体压实系数和瑞雷波相速度,建立研究区地基土体弹性波速与压实系数之间的统计关系;最后,利用所建立的统计关系将填方地基土体瑞雷波相速度三维成像转换为土体压实系数三维成像,从而获取地基土体压实系数的空间连续分布,实现地基处理效果的快速连续检测,为地基填筑质量的评价提供可靠依据。
1. 检测原理和方法
1.1 地基土体弹性波速空间分布的快速连续检测
采用多道瞬态瑞雷波探测方法[9-11],对地基土体弹性波速空间分布展开连续检测,从而获得可以反映地基土体三维加固效果的弹性波速空间成像,即:地基土体瑞雷波相速度-深度成像剖面、地基土体瑞雷波相速度成像水平切片[12]。
1.1.1 瑞雷波检测原理
瑞雷波是沿介质表面或层面传播的一种弹性波动,波动能量集中在界面附近一定范围内,离开界面一定距离后其能量迅速衰减。瑞雷波的质点振动轨迹位于波传播方向与界面法线方向决定的入射面内,在界面附近,其质点振动方式为长轴平行于界面法线方向的逆进椭圆。在不均匀介质中传播的瑞雷波有一个重要的特性:频散,即,瑞雷波中不同频率成分(即,不同波长)的波动以不同的速度向前传播[13-14]。波动现象中波长
$ \lambda $ 、波速$ V $ 和频率$ f $ 之间有一个简单的关系:$ \lambda = {V /f} $ ;另外,理论分析表明,瑞雷波的有效探测深度$ Z $ 与其波长成正比,即$Z=\beta \cdot\lambda$ ,其中,$ \beta $ 为与地基土体泊松比有关的系数,对一般土体地基可取$ \beta $ =0.7。层状介质瑞雷波频散曲线的正演分析表明,频散曲线的高频部分与浅层介质相对应,频散曲线的低频部分与深层介质相对应,频散曲线的拐点与不同介质的分层界面相对应,这为利用瑞雷波探测地基土体弹性波速的空间分布提供了可能[15]。
1.1.2 瑞雷波检测方法
对填方地基土体弹性波速空间分布的测量采用考虑道间时差相位的多道瞬态瑞雷波探测方法(TDP法)[9]。该方法只用两道检波器的瞬态瑞雷波记录即可提取多种频率成分波动的相速度,完成现有方法通过一个多道检波器排列才能解决的工作。
如图1(a)所示,按一定的间距(道间距Δx)布置在同一条测线多个测点上的检波器可以观测同一激发点上、同一次激发的瑞雷波,这些按一定的道间距布置在测线上的检波器构成一个检波器排列(图1(b))。譬如,采用由12个检波器组成的检波器排列,相对于同一次激发,由自制工程地震仪获取12道瞬态瑞雷波记录时域波形(图1(c))。根据本工程对探测空间分辨率的要求,检波器的道间距设为Δx,一个排列的12道检波器可覆盖11条Δx的测线长度(排列长度)范围[13,16]。
![]() 图 1 瞬态瑞雷波激发和观测系统及探测仪器设备Figure 1. Schematic diagram of the transient Rayleigh wave generating and observing device system
图 1 瞬态瑞雷波激发和观测系统及探测仪器设备Figure 1. Schematic diagram of the transient Rayleigh wave generating and observing device system1.1.3 地基土体瑞雷波相速度成像空间架构
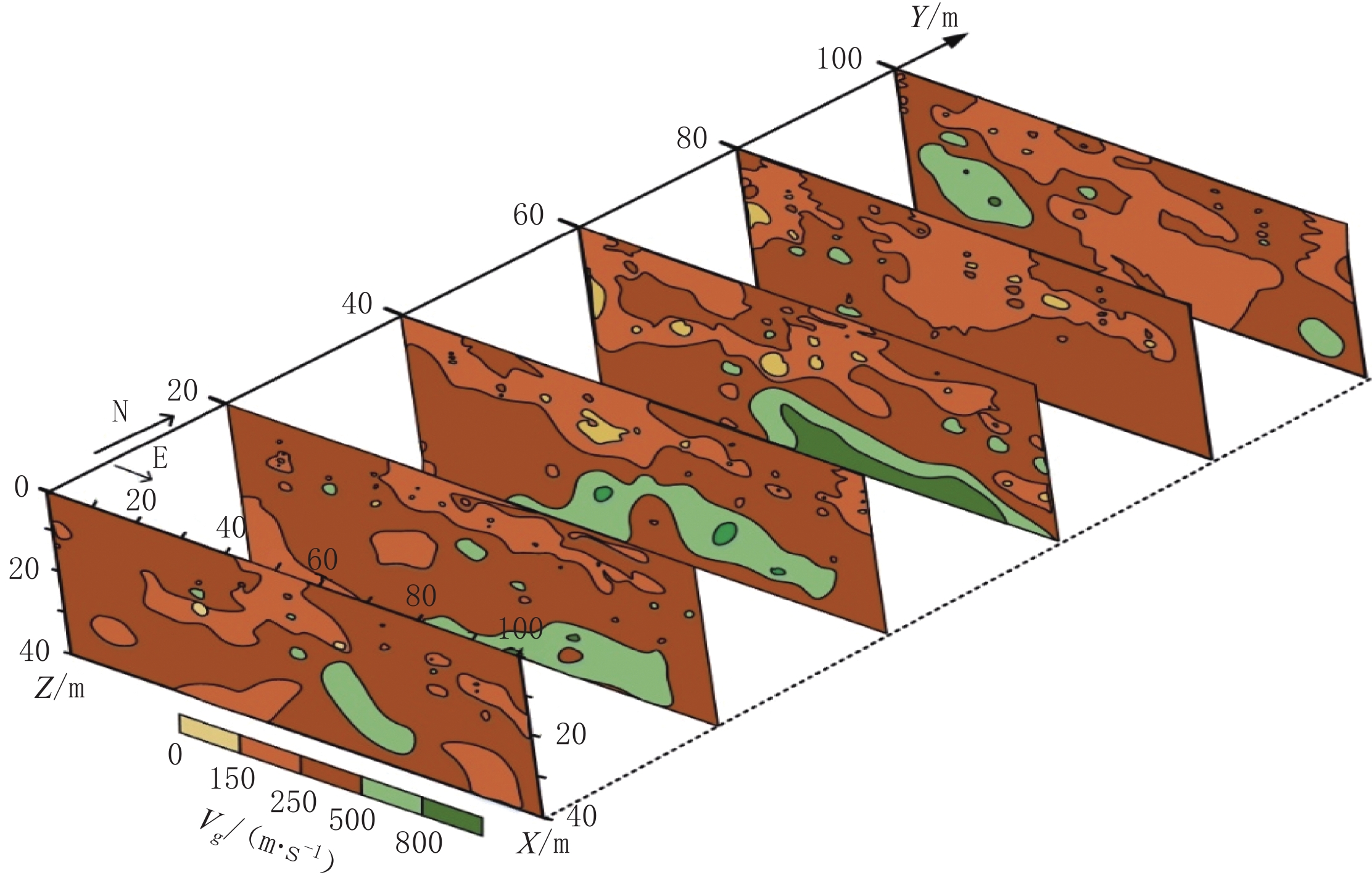
地基土体瑞雷波相速度三维成像的空间架构如图2所示。提取各测线所有相邻道(测点)之间的瑞雷波相速度,对于n道检波器的测线上相邻道两两组合可以得到
$n-1$ 条瑞雷波相速度-深度(${V_{\text{R}}} - Z$ )曲线。联合同一测线上所有相邻道间的${V_{\text{R}}} - Z$ 曲线构建沿测线的成像剖面(二维成像${V_{\text{R}}} - X - {Y_{\text{i}}} - Z$ ,i=1,2,···,l;其中,Yi为第i条测线对应的Y轴坐标,l为测线的条数)。整合所有测线的瑞雷波相速度-深度成像剖面,即可形成探测区介质体的三维瑞雷波相速度成像${V_{\text{R}}} - X - Y - Z$ ,并可进一步重构不同深度上介质层的瑞雷波相速度成像水平切片(${V_{\text{R}}} - X - Y - {Z_{{j}}}$ ,j=1,2,···,m;其中,$Z_j $ 为第j个水平切片的深度坐标,m为切片的个数)。![]() 图 2 地基土体瑞雷波相速度三维成像的空间架构Figure 2. Spatial architecture of the Rayleigh wave phase velocity 3D imaging
图 2 地基土体瑞雷波相速度三维成像的空间架构Figure 2. Spatial architecture of the Rayleigh wave phase velocity 3D imaging1.2 地基土体压实系数空间分布的抽样检测
现场土体取样地点均选在瑞雷波探测检波器排列中两个检波器测点之间,以便土样测试得到的土体压实系数与相应位置的瑞雷波相速度对应比较。在每个点的几个不同深度上采取若干组土样,求取该点不同深度处土体参数的平均值。
压实系数
$ \gamma $ 指现场经加固压实的地基土体实际干密度(原状土体干密度)$ {\rho _{\text{d}}} $ (g/cm3)与地基土体的最大干密度$ {\rho _{\text{d}}}_{\max } $ (g/cm3)的比值,即:$$ \gamma {\text{ = }}\frac{{{\rho _{\rm{d}}}}}{{{\rho _{{\rm{d}}\max }}}}。 $$ (1) 压实系数测试分为土体最大干密度测试和土体实际干密度测试两部分,测试土样采自现场地基土体。根据《土工试验方法标准》GB/T50123-2019[5],最大干密度
$ {\rho _{\text{d}}}_{\max } $ 采用重型击实试验方法测定。土体实际干密度采取环刀法测试,采取现场土体原状土样,现场取样随即完成土样质量$ {m_0} $ 称重和土样体积$ {v_0} $ 计算,土样质量m0与土样体积V0的比值即为土体原状密度$ {\rho _0} $ 。将土样用密封袋密封带回实验室烘干,测得原状土体含水率$ {w_0} $ 。按式(2)求出原状干密度:$$ {\rho _{\text{d}}}{\text{ = }}\frac{{{\rho _0}}}{{1 + {{0.01}{w_0}}}} 。 $$ (2) 1.3 地基土体瑞雷波相速度成像到地基压实系数成像的转换
按地基土体加固相关标准规范要求,地基土体加固效果的直接评价指标主要是地基土体压实系数[1,4]。因此,还需要将填方地基土体瑞雷波相速度(空间成像)转换为对地基承载力有贡献的深度范围内地基土体深度平均压实系数(水平分布成像)。为此,要展开两方面分析工作。
1.3.1 地基土体弹性波速与土体压实系数关系分析
考虑地基承载能力主要是地基附加应力影响深度
$ {Z_\sigma } $ 范围内地基土体的贡献,取抽样点上地基土体附加应力影响深度范围内$Z \leq {Z_\sigma }$ 地基土体的瑞雷波相速度$ {V}_{{\rm{R}}}({Z}_{\sigma }) $ 与地基土体深度平均压实系数$ \overline{\gamma }({Z}_{\sigma }) $ 进行统计分析,建立附加应力影响深度范围内的瑞雷波相速度与地基土体深度平均压实系数之间的统计关系$$ \overline \gamma {\text{ = }}f\left( {{V_{\rm{R}}}} \right),\quad Z \leq {Z_\sigma } 。 $$ (3) 1.3.2 附加应力影响深度范围内地基土体深度平均压实系数水平分布成像
利用式(3)将Z=Zσ对应的地基土体瑞雷波相速度成像水平切片(
$ {V_{\text{R}}} - X - Y - {Z_\sigma } $ )转换为$ Z \leq {Z_\sigma } $ 深度范围内地基土体深度平均压实系数水平分布成像($ \bar \gamma - X - Y - {Z_\sigma } $ )。1.4 地基加固效果空间分布的评价
地基土体加固效果关注两个方面,一个是土体加固程度,可以由土体的弹性波速(瑞雷波相速度)和压实系数大小反映;另一个是土体加固的均匀性,由土体弹性波速和压实系数的空间分布变化反映。
根据探测得到的填筑地基土体瑞雷波相速度成像(各条测线的瑞雷波相速度-深度剖面以及不同深度的瑞雷波相速度水平切片)以及按式(3)由瑞雷波相速度成像转换得到的附加应力影响深度范围内地基土体的深度平均压实系数水平分布成像对地基土体加固效果进行分析评价。
1.4.1 按瑞雷波相速度的地基土体加固效果评价
地基土体的弹性波速与地基土体的密实程度直接相关,弹性波速越大,土体越密实。理论上对于同一介质,瑞雷波波速
$ {V_{\text{R}}} $ 约为0.95倍的剪切波速$ {V_{\text{R}}} $ ,结合建筑抗震设计规范(GB5011-2010)[17]中土的类型划分和剪切波速范围,列出瑞雷波相速度与地基土体特性之间的关系(表1),即可对工程场地地基土体加固效果做出分析评价。表 1 填方地基压实土体瑞雷波相速度$ {V_{\text{R}}} $ 分级与土体性状对照表Table 1. Comparison table between the Rayleigh wave phase velocity$({V_{\text{R}}} )$ classification and the soil properties of compacted soil mass土体性状 软弱土体 中软土体 中硬土体 坚硬土体 岩体 VR/(m/s) ≤150 150~250 250~500 500~800 ≥800 1.4.2 按深度平均压实系数的地基加固效果评价
按统计关系式(3)将
$ Z = {Z_\sigma } $ 对应的地基土体瑞雷波相速度成像水平切片($ {V_{\text{R}}}- X - Y- {Z_\sigma } $ )数据转换为$ Z \leq {Z_\sigma } $ 深度范围内地基土体深度平均压实系数水平分布成像($ \bar \gamma - X - Y - {Z_\sigma } $ )数据。参照建筑地基处理技术规范(JGJ 79-2012)[1]对地基加固处理压实系数的控制标准,制定场地$ Z \leq {Z_\sigma } $ 深度范围内地基土体深度平均压实系数$\bar \gamma $ 分级与地基土体性状之间的定性对照,如表2所示。表 2 填方地基压实土体深度压实系数$\bar \gamma $ 分级与土体性状对照表Table 2. Comparison table between the classification of depth compaction coefficient ($\bar \gamma $ ) and the soil properties of compacted soil mass土体性状 软弱土体
压实程度较低中软土体
压实程度中等中硬土体
压实程度较高坚硬土体
压实程度高$\bar \gamma $ 0~0.78 0.78~0.83 0.83~0.95 0.95~1 按表2划定的地基土体深度平均压实系数分级,将工程场地
$ Z \leq {Z_\sigma } $ 深度范围内地基土体深度平均压实系数水平分布数据绘制成地基土体深度平均压实系数水平分布成像($ \bar \gamma -X - Y - {Z_\sigma } $ )。根据地基土体深度平均压实系数水平分布成像反映的地基土体压实系数量值和水平分布,即可对工程场地地基土体加固效果做出分析评价。2. 现场检测和数据分析
如图3所示,地基土体压实效果检测的场地为一个规则的矩形区块。现场检测分为场地地基土体弹性波速空间分布的多道瞬态瑞雷波探测和场地抽样点一定深度范围内地基土体压实系数的取样测试两部分。
![]() 图 3 填方地基土体压实效果检测场地瑞雷波测线及土体抽样点布置图Figure 3. Layout of the Rayleigh wave survey lines and soil sampling points at the testing site for the compaction effect of filling foundation soil mass
图 3 填方地基土体压实效果检测场地瑞雷波测线及土体抽样点布置图Figure 3. Layout of the Rayleigh wave survey lines and soil sampling points at the testing site for the compaction effect of filling foundation soil mass2.1 地基土体多道瞬态瑞雷波探测
在现场布置多条测线,沿测线进行多道瞬态瑞雷波探测,采用考虑道间时差相位的瞬态瑞雷波相速度分析方法[7],获得场地地基土体瑞雷波相速度的空间分布数据,形成场地地基土体瑞雷波空间成像(瑞雷波相速度-深度剖面,不同深度瑞雷波相速度成像水平切片)。
2.1.1 测线布置
如图3所示,填方地基土体压实效果检测场地为一个规则的矩形区块。以检测场地北侧DLW值班室西南角为基准点建立场地观测坐标系
$X - Y - Z$ :$X - Y$ 平面与场地地面重合;X轴在基准点以南,沿东西向指向东(E),距基准点135.5 m;Y轴在基准点以西,沿南北向指向北(N),距基准点61.2 m;Z轴自X、Y轴交点起垂直向下。在场地内平行于X轴布置 11条多道瞬态瑞雷波测线,测线间隔10 m,由南向北测线编号依次为CX1~CX11,每条测线布置12个测点,测点间距10 m。为产生沿测线传播的瞬态瑞雷波,每条测线设置一个激发点,位于测线向西的延长线上,与测点1相距15 m。
2.1.2 多道瞬态瑞雷波探测
多道瞬态瑞雷波探测的现场实施要考虑瞬态瑞雷波的激发、观测记录各个环节的技术实现,最重要的是通过现场探测,获得能够满足探测深度和探测分辨率要求的瞬态瑞雷波记录数据。
利用灌满混凝土的圆柱形水桶做成约为120 kg的混凝土大锤,在激发点上冲击地面,从而产生在地基土体中传播的瞬态瑞雷波。对激发得到的记录波形进行解译表明,以这种方式激发所能达到的有效探测深度超过40 m。按图3所示的测线布置铅垂向检波器,记录瞬态瑞雷波在地基土体表面产生的质点振动的铅垂分量。
为便于地基土体瑞雷波相速度成像,取相邻两个测点的中点坐标作为这两个测点间提取的瑞雷波相速度与场地对应的平面位置,相速度对应的地基土体深度
$ Z $ 由相速度对应的波长$ {Z_R} $ 确定($ Z=\beta \cdot{\lambda }_{R} $ ,其中,$ \beta $ 为波长深度转换系数,通常与地基土体的泊松比有关)。2.1.3 地基土体瑞雷波相速度成像
按照上述多道瞬态瑞雷波记录和相速度提取方法,可以获得一个检波器排列中各个相邻道之间的瑞雷波相速度-深度数据。
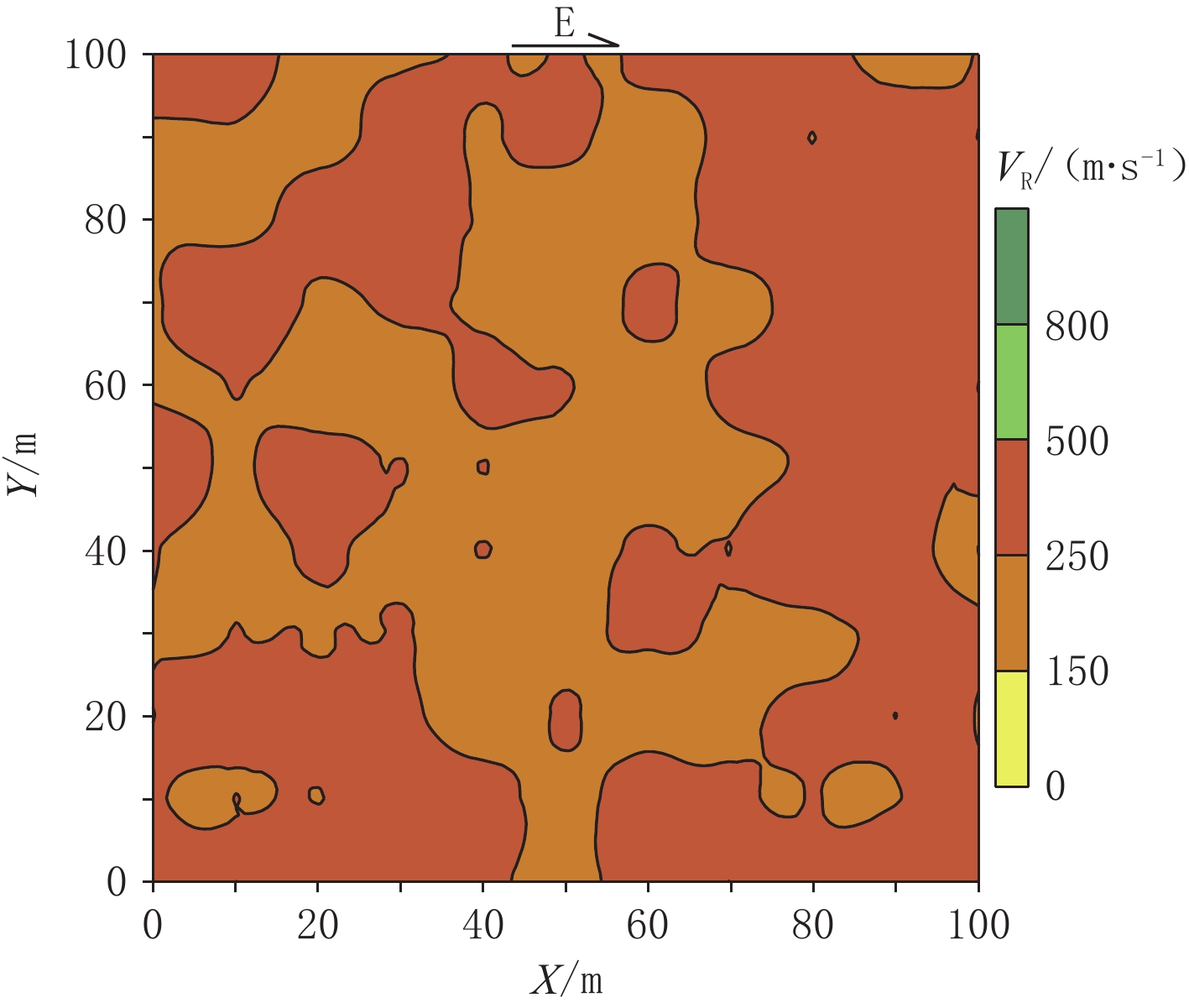
图4所示为由现场多道瞬态瑞雷波探测获得的填方地基土体Z=40深度范围奇数编号测线的成像剖面。在各条测线成像剖面的基础上构建填方地基土体瑞雷波相速度三维成像,由三维成像截取Z=5深度上的瑞雷波相速度成像水平切片如图5所示。
![]() 图 4 填方地基土体瑞雷波相速度成像剖面Figure 4. Rayleigh wave phase velocity-depth imaging profile of the foundation soil mass
图 4 填方地基土体瑞雷波相速度成像剖面Figure 4. Rayleigh wave phase velocity-depth imaging profile of the foundation soil mass![]() 图 5 Z=5填方地基土体瑞雷波相速度VR成像水平切片Figure 5. VR imaging horizontal section of the Rayleigh wave phase velocity in the foundation soil mass at Z=5
图 5 Z=5填方地基土体瑞雷波相速度VR成像水平切片Figure 5. VR imaging horizontal section of the Rayleigh wave phase velocity in the foundation soil mass at Z=52.2 地基土体压实系数检测
通过场地地基土体抽样点一定深度范围内土体取样测试,获得抽样点上不同深度上的土样压实系数,并进一步获得一定深度范围内土体深度平均压实系数数据。对场地地基土体瑞雷波相速度数据和场地抽样点土体取样的压实系数数据进行统计获得附加应力影响深度以上的地基土体瑞雷波相速度与深度平均压实系数之间的统计关系。进而,利用所述统计关系,将附加应力影响深度上的地基土体瑞雷波相速度水平切片转换为地基土体深度平均压实系数水平分布成像。
2.2.1 场地地基土体抽样点布置及土体取样测试
按以往地基土体载荷试验的经验,设地基土体附加应力的影响深度
$ {Z_\sigma }=5 $ 。如图3所示,在检测场地范围内布置了9个地基土体抽样点(编号1~9)。在每个抽样点上钻孔,在设定的附加应力影响深度(
$ {Z_\sigma } =5$ )内$ {Z_{{j}}} = $ 1、2、3、4、5几个深度上采用环刀法采取原状土样,测定各个深度上原状土体的原状密度$ {\rho _0} $ 和原状含水率$ {w_0} $ ,场地土体实测最大干密度$ {\rho _{{\text{d}}\max }} = $ 1.987。进一步,按前述方法求出不同深度上地基土体的压实系数${\gamma _{{{zjk}}}}$ $({Z_{{j}}} =$ 1,2,5;$ k = $ 1,2,···,9)。根据这些数据,可求出各抽样点上$ Z \leq {Z_\sigma } $ 深度范围内地基土体的深度平均压实系数$\overline{\gamma }({Z}_{\sigma })_{\text{k}}$ ($ k = $ 1,2,···,9)。2.2.2 地基土体瑞雷波相速度与压实系数的关系
在场地地基土体多道瞬态瑞雷波探测成像结果中提取
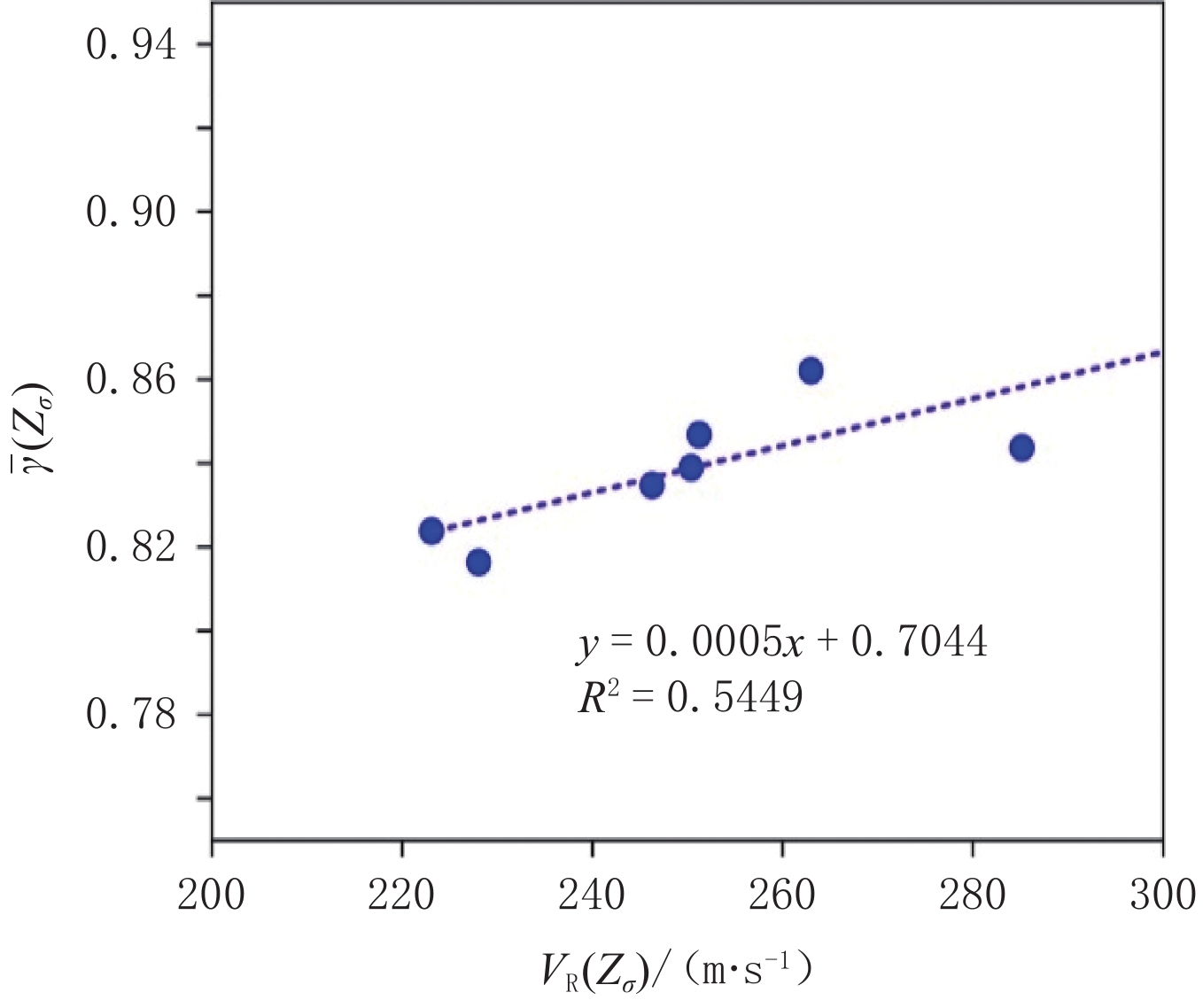
$ Z = {Z_{\text{σ }}} =5$ 深度上对应各个土体抽样点的瑞雷波相速度水平分布数据${V}_{\text{R}}({Z}_{\sigma })_{{k}}$ $( k =1,2,\cdots,9) $ 。对上述测试数据$\{(\overline{\gamma }({Z}_{\sigma })_{{k}},{V}_{\text{R}}({Z}_{\sigma })_{{k}})|$ $ k = 1,2,\cdots,9\}$ (表3,剔除瑞雷波相速度最大值313 m/s和最小值203 m/s对应的异常数据)进行统计分析,得到如式(4)和图6所示的统计关系(统计方差$ {R^2} $ =0.5449)。表 3 填方地基土体抽样点土体参数测试结果一览表Table 3. Test results of soil parameters at filling foundation soil sampling points抽样点
编号$\bar \gamma(Z_\sigma )$ $V_{\rm{R}}(Z_\sigma )$/m·s−1 抽样点
编号$\bar \gamma(Z_\sigma )$ $V_{\rm{R}}(Z_\sigma )$/m·s−1 抽样点
编号$\bar \gamma(Z_\sigma )$ $V_{\rm{R}}(Z_\sigma )$/m·s−1 1 0.835 246 4 0.839 250 7 0.862 263 2 0.844 285 5 0.807 313 8 0.824 223 3 0.833 203 6 0.816 228 9 0.847 251 ![]() 图 6 地基土体瑞雷波相速度与压实系数的统计关系Figure 6. Statistical relationship between the Rayleigh wave phase velocity and the compaction coefficient of the foundation soil
图 6 地基土体瑞雷波相速度与压实系数的统计关系Figure 6. Statistical relationship between the Rayleigh wave phase velocity and the compaction coefficient of the foundation soil$$ \overline{\gamma }({Z}_{\sigma })_{{k}}=0.000\,5\cdot{V}_{{\rm{R}}}({Z}_{\sigma })_{{k}}+0.704\,4 。 $$ (4) 2.2.3 场地地基土体压实系数水平分布成像
利用式(4)所示的统计关系,将附加应力影响深度(
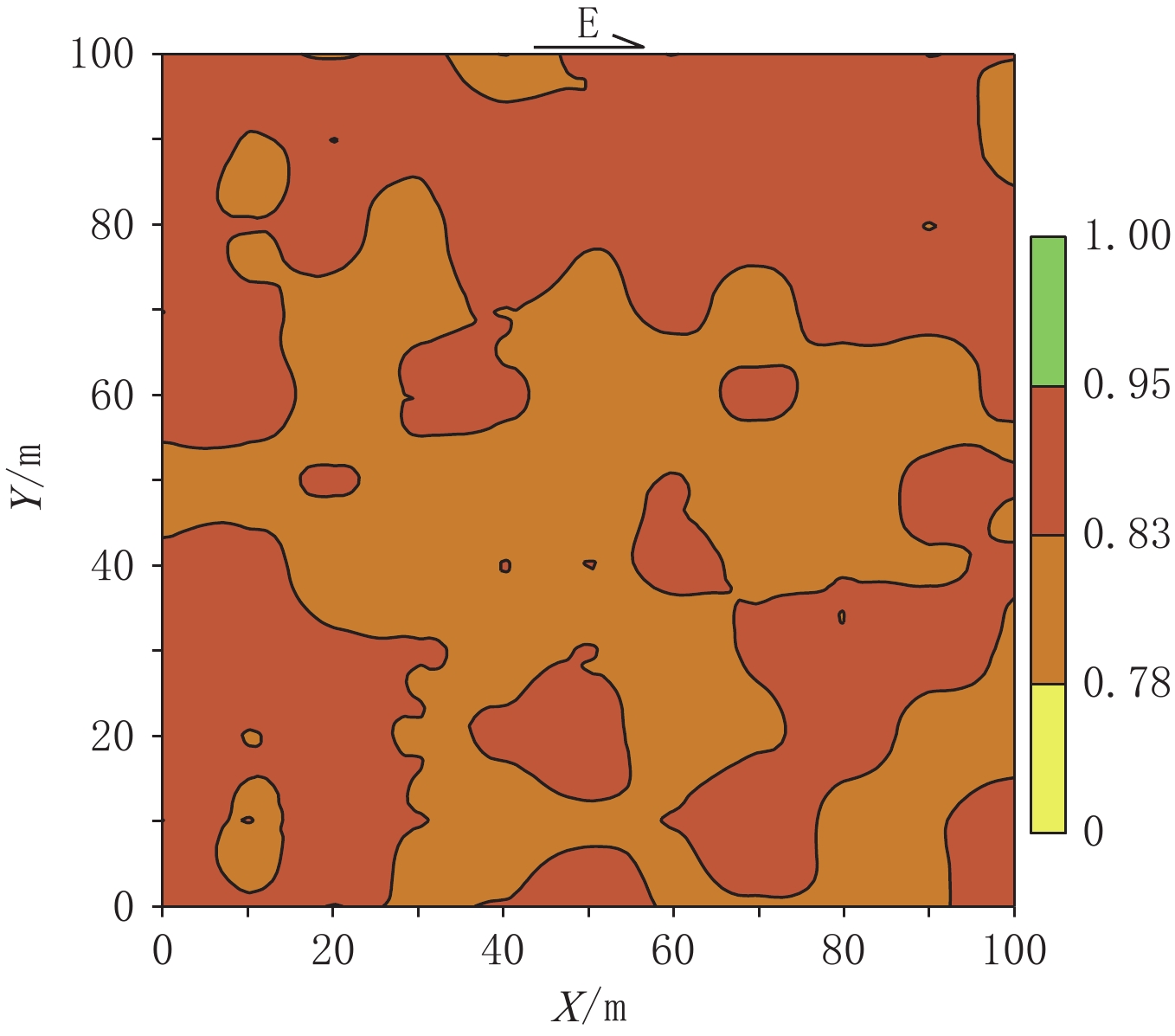
$ Z = {Z_\sigma } =5 $ )上的地基土体瑞雷波相速度水平切片($ {V_{\text{R}}} - X - Y - {Z_\sigma } $ )转换为地基土体深度平均压实系数水平分布成像($ \bar \gamma - X - Y - {Z_\sigma } $ ),转换结果如图7所示。![]() 图 7 填方地基持力层土体(Z≤5)深度平均压实系数水平分布成像(
图 7 填方地基持力层土体(Z≤5)深度平均压实系数水平分布成像($\bar \gamma - X - Y - {Z_\sigma }$ )Figure 7. Horizontal distribution imaging of the depth-average compaction coefficient of the bearing layer soil mass (Z≤5) in the filling foundation($ \bar \gamma - X - Y - {Z_\sigma } $ )3. 填方地基土体压实加固效果评价
填方地基土体瑞雷波相速度成像和附加应力影响深度范围内地基土体深度平均压实系数的水平分布成像为场地地基土体加固效果评价提供了依据。
3.1 依据瑞雷波相速度的填方地基土体加固效果评价
根据瑞雷波相速度成像剖面和水平切片所反映的地基土体弹性波速的大小和空间分布,可以了解经压实处理后填方地基土体的软硬程度和均匀程度。
3.1.1 瑞雷波相速度—深度剖面反映的填方地基土体性状
由图4所示填方地基土体几个瑞雷波相速度-深度剖面示例可以看出,检测场地地基中存在上部和下部(浅部和深部)两套显著不同的岩土单元:浅部为
$ {V_{\text{R}}} \leq $ 500的松散沉积土层(或填筑土体);深部则是由基岩(${V_{\text{R}}} > $ 800)和坚硬的残积土体(500$ < {V_{\text{R}}} \leq $ 800)构成的沉积基底。在
$Z > 20$ 以下的深部土体中存在大片的$ {V_{\text{R}}} > $ 500的坚硬土体分布,甚至有$ {V_{\text{R}}} > $ 800的硬核岩体。在各个成像剖面深部出露的$ {V_{\text{R}}} > $ 500的坚硬岩土体的深浅位置、形态尺度变化较大,反映出了早期沉积基底岩土体所遭受的地质作用和风化侵蚀,从而形成起伏不平、形态多变的基底岩土体。后期
$ {V_{\text{R}}} \leq $ 500的松散沉积物以不整合的接触关系陆续沉积覆盖在沉积基底之上,形成了填方施工前的场地天然地基土体。进一步观察浅部土体中的波速分布可以看到,浅部土体中存在这较大面积$ {V_{\text{R}}} \leq $ 250的低速区,其中不少区块还存在$ {V_{\text{R}}} \leq $ 150的更为软弱土体。这些软弱区块反映了填方施工前场地的低洼部位,甚至可以反映出低洼积水向深部渗透导致的软弱低速区向剖面更深部位的延伸。3.1.2 瑞雷波相速度成像水平切片反映的填方地基土体性状
瑞雷波相速度成像水平切片可以看出不同深度上地基土体软硬程度及其在水平横向上的变化。由图5所示
$ Z =5$ 深度上的瑞雷波相速度成像水平切片可以看出,这个深度上的瑞雷波相速度均在150~500之间,说明在深度5 m以上的地基土体属于中软-中硬土体,土体大致均匀。$ 150< {V_{\text{R}}} \leq 250 $ 的相对低速分布区大致可以反映出具有一定厚度的填方土体分布的大致范围。3.2 依据深度平均压实系数的填方地基土体加固效果评价
根据
$\bar \gamma(Z_\sigma )$ 水平分布成像可以了解场地地基持力层土体压实压实系数的大小和横向分布的均匀程度。如图7所示,场地地基土体经压实加固处理后,地基持力层(附加应力影响深度范围)土体的平均压实系数介于0.78~0.95之间,最小值0.816,最大值0.862,压实系数差异Δγ=0.046。由此可见,经压实加固处理后的地基土体密实均匀程度比较好。但是,按照现行地基处理规范标准(γ>0.95),本次检测场地填方地基土体在附加应力影响深度范围内的加固效果尚未达到规范要求(绝对标准评价),在地基投入使用前需采取进一步的压实处理措施。
4. 结论
通过对所依托的大型工程填方地基场地的多道瞬态瑞雷波探测和抽样点地基土体压实系数测试,获得有关地基土体压实加固效果的信息,经分析得到如下结论:
(1)根据瑞雷波相速度—深度成像剖面和不同深度的水平切片反映的地基土体波速变化,场地浅部(
$ Z \leq $ 5)土层的瑞雷波相速度量值范围为150$ < {V_{\text{R}}} \leq $ 500,属于中软土体~中硬土体,地基处理空间均匀性较好。(2)检测得到的填方地基持力层(
$Z < {Z_{\text{σ}}} =$ 5)土体的深度平均压实系数$ \overline{\gamma }({Z}_\sigma ) $ 最大、最小值分别为($ {\gamma _{\max }} = $ 0.862、$ {\gamma _{\min }} = $ 0.816),压实系数差异$ \Delta \gamma = $ 0.046,经压实处理后的地基土体相对比较均匀。(3)地基压实处理后的地基土体压实系数需满足 γc ≥0.95的要求,本次检测场地填方地基土体在附加应力影响深度范围内的加固效果尚未达到规范要求(绝对标准评价),在地基投入使用前需采取进一步的压实处理措施。
-
![]()
图 1 男,35岁,右胫骨平台外侧缘撕脱骨折
膝关节CT平扫横断面(a)及冠状面MPR(b),示右胫骨平台外侧缘可见撕脱小骨块体积0.04 cm3(0.59 cm×0.11 cm×0.56 cm),距Gerdy结节距离约2.02 cm。(c)~(d)冠状面脂肪抑制TSE PDWI。(c)显示ALL附着于骨折块上并水肿(箭)。(d)显示ITB未见明显异常(箭)。
Figure 1. Imaging of a 35-year-old male with an avulsion fracture of the lateral edge of the right tibial plateau
![]()
图 2 Segond骨折块大小、体积、距Gerdy结节及关节面距离与ITB附着的ROC曲线
Figure 2. ROC curve of the Segond fracture block size, volume, distance from Gerdy’s nodule, and articular surface to ITB attachment
![]()
图 3 男,51岁,左胫骨外侧平台撕脱骨折
膝关节CT平扫横断面(a)及冠状面MPR(b),显示右胫骨平台外侧缘可见撕脱小骨块体积0.07 cm3(0.92 cm×0.11 cm×0.70 cm),距Gerdy结节距离约0.72 cm。(c)~(d)冠状面脂肪抑制TSE PDWI。(c)显示ALL(长箭)及ITB(短箭)附着骨折块上,韧带未见明显损伤。(d)显示ITB附着点水肿(细箭),内侧副韧带损伤(粗箭)。
Figure 3. Imaging of a 51-year-old male with an avulsion fracture of the left lateral tibial plateau
表 1 Segond骨折合并韧带、半月板损伤(例%)
Table 1 Segond fractures with ligament and meniscus injury (%)
影像表现 ACL ALL ITB PCL LCL MCL MM* ML* 撕裂 19(42.22) 2(4.44) 0 0 2(4.44) 10(22.22) 8(17.77) 9(20.00) 水肿 22(48.89) 29(64.44) 12(26.67) 5(11.11) 24(53.33) 25(55.56) 11(24.44) 7(15.56) 正常 4(8.89) 14(31.11) 33(73.33) 40(88.89) 19(42.22) 20(44.44) 26(57.78) 19(42.22) 注:ALL:前外侧韧带;ITB:髂胫束;ACL:前交叉韧带;PCL:后交叉韧带;LCL:外侧副韧带;MCL:内侧副韧带;MM:内侧半月板;ML:外侧半月板。*半月板损伤 Ⅲ 度以上归为撕裂、Ⅰ度、Ⅱ度为水肿。  下载: 导出CSV
下载: 导出CSV
表 2 Segond骨折块的大小、位置与附着韧带的关系
Table 2 The relationship between the size and position of the Segond fracture block and the attached ligament
Segond骨折块 ALL(n=45) ITB(n=25) 统计检验 Z P D前后/cm 1.05±0.37 1.38±3.3 -2.73 0.006 D左右/cm 0.62±0.19 0.73±0.15 -1.69 0.090 D上下/cm 0.28±0.08 0.36±0.08 -0.31 0.002 D/cm3 0.19±0.12 0.36±0.13 -4.16 <0.001 D距Gerdy结节/cm 0.90±0.23 0.64±0.16 -3.39 0.001 D距关节面/cm 0.21±0.11 0.20±0.12 -0.89 0.370
下载: 导出CSV
-
[1] SEGOND P. Recherches cliniques et experimentales sur les epanchements sanguins du genou par entorse[M]. Paris: Aux Bureaux du Progrès Médical, 1879: 1-85.
[2] WHARTON R, HENCKEL J, BHATTEE G, et al. Segond fracture in an adult is not pathognomonic for ACL injury[J]. Knee Surgery, Sport Traumatology, Arthroscopy, 2015, 23(7): 1925−1928. doi: 10.1007/s00167-014-2965-x
[3] PATEL R M, BROPHY R H. Anterolateral ligament of the knee: Anatomy, function, imaging, and treatment[J]. The American Journal of Sports Medicine, 2018, 46(1): 217−223. doi: 10.1177/0363546517695802
[4] FERRETTI A, MONACO E, WOLF M R, et al. Surgical treatment of Segond fractures in acute anterior cruciate ligament reconstruction[J]. Orthopaedic Journal of Sports Medicine, 2017, 5(10): 1−6.
[5] de MAESENEER M, BOULET C, WILLEKENS I, et al. Segond fracture: Involvement of the iliotibial band, anterolateral ligament, and anterior arm of the biceps emoris in knee trauma[J]. Skeletal Radiology, 2015, 44(3): 413−421. doi: 10.1007/s00256-014-2044-x
[6] HELITO P V P, BARTHOLOMEEUSEN S, CLAES S, et al. Magnetic resonance imaging evaluation of the anterolateral ligament and the iliotibial band in acute anterior cruciate ligament injuries associated with Segond fractures[J]. Arthroscopy, 2020, 36(6): 1679−1686. doi: 10.1016/j.arthro.2020.02.005
[7] GETGOOD A, BROWN C, LORDING T, et al. The anterolateral complex of the knee: Results from the International ALC Consensus Group Meeting[J]. Knee Surgery, Sport Traumatology, Arthroscopy, 2019, 27(1): 166−176. doi: 10.1007/s00167-018-5072-6
[8] 范亚杰, 张民泽. 前外侧韧带对膝关节旋转稳定作用的研究进展[J]. 骨科临床与研究杂志, 2017,2(4): 253−256. [9] DAVIS B A, HILLER L P, IMBESI S G, et al. Isolated lateral collateral ligament complex injury in rock climbing and Brazilian Jiu -jitsu[J]. Skeletal Radiology, 2015, 44(8): 1175−1179. doi: 10.1007/s00256-015-2108-6
[10] CLAES S, VEREECKE E, MAES M, et al. Anatomy of the anterolateral ligament of the knee[J]. Journal of Anatomy, 2013, 223(4): 321−328. doi: 10.1111/joa.12087
[11] DODDS A L, HALEWOOD C, GUPTE C M, et al. The anterolateral ligament: Anatomy, length changes and association with the Segond fracture[J]. Bone & Joint Journal, 2014, 96-B(3): 325−331.
[12] FLORES D V, SMITAMAN E, HUANG B K, et al. Segond fracture: An MR evaluation of 146 patients with emphasis on the avulsed bone fragment and what attaches to it[J]. Skeletal Radiology, 2016, 45(12): 1635−1647. doi: 10.1007/s00256-016-2479-3
[13] 徐亦鹏, 李冕, 闫石, 等. 前交叉韧带损伤与胫骨平台后侧骨损伤的相关性分析[J]. 骨科, 2020,11(3): 54−58. doi: 10.3969/j.issn.1674-8573.2020.03.009 XU Y P, LI M, YAN S, et al. Correlation analysis between anterior cruciate ligament injury and posterior tibial plateau bone injury[J]. Orthopaedics Journal, 2020, 11(3): 54−58. (in Chinese). doi: 10.3969/j.issn.1674-8573.2020.03.009
[14] 狄亚龙, 韩长旭, 任逸众. 膝关节前外侧韧带的研究进展[J]. 中华解剖与临床杂志, 2017,22(3): 252−255. doi: 10.3760/cma.j.issn.2095-7041.2017.03.018 DI Y L, HAN C X, REN Y Z. The research progress of anterolateral ligament[J]. Chinese Journal of Anatomy and Clinics, 2017, 22(3): 252−255. (in Chinese). doi: 10.3760/cma.j.issn.2095-7041.2017.03.018
[15] VIEIRA E L, VIEIRA E A, SILVA R T, et al. An anatomic study of the iliotibial tract[J]. Arthroscopy, 2007, 23(3): 269−274. doi: 10.1016/j.arthro.2006.11.019







































































































计量
- 文章访问数: 256
- HTML全文浏览量: 153
- PDF下载量: 20


