
A Study of the Correlations between CT and MRI Findings and Elevated Serum IgG4 Levels in Newly-diagnosed Patients with IgG4-related Sclerosing Cholangitis
-
摘要: 目的:观察IgG4相关硬化性胆管炎(IgG4-SC)的CT和MRI表现,探究初诊患者影像特征与血清IgG4、IgG水平的关系。方法:总结50例IgG4-SC初诊患者的临床、实验室及影像资料,通过MRCP观察病变分型、管腔狭窄形态与扩张程度;增强MRI和CT观察管壁增厚、强化模式及合并其他IgG4-RD的数量,分析基线血清IgG4及IgG水平与胆管病变和合并其他IgG4-RD数量的相关性。结果:初诊41例MRCP见Ⅰ型IgG4-SC 28例,Ⅱa型11例,Ⅲ型、Ⅳ型各1例;肝外胆管狭窄端呈漏斗状37例、截断状4例,狭窄段均为长狭窄(≥1.0 cm),其中1例胰腺段狭窄伴憩室样外凸;狭窄上游胆管扩张37例,不扩张4例。初诊42例增强MRI/CT均显示肝外胆管壁连续性增厚,15例见肝内胆管壁弥漫性增厚,管壁增厚呈向心性。50例IgG4-SC均合并AIP,其他受累器官还包括肾19例、涎腺7例、腹膜后纤维化5例、肝4例、肺4例、前列腺2例、硬化性纵隔炎2例、胆囊壁增厚20例及上腹部淋巴结肿大15例。基线血清IgG4、IgG水平升高与合并其他IgG4-RD的数量呈正相关,而与胆管壁厚度、狭窄段长度不相关。结论:胆管局限性狭窄伴上游胆管扩张或不扩张以及管壁弥漫性增厚是IgG4-SC初诊患者的特征性MRI和CT表现。基线血清IgG4及IgG水平升高与胆管病变的严重程度无关,而与合并其他IgG4-RD的数量有关。
-
关键词:
- X线计算机体层摄影 /
- 磁共振成像 /
- IgG4相关硬化性胆管炎 /
- 诊断
Abstract: Objective: To observe the CT and MRI findings in newly diagnosed patients with IgG4-related sclerosing cholangitis (IgG4-SC) and explore their correlations with serum IgG4 and IgG levels. Methods: The clinical, laboratory, and imaging data of 50 newly diagnosed IgG4-SC patients were retrospectively summarized. The type of lesions, shape of lumen stenosis, degree of dilatation of the diseased bile ducts on MRCP, characteristics and enhancement patterns of the thickened bile duct walls, and the number of other coexisting IgG4-RDs on enhanced MRI and CT were observed. Subsequently, the correlations of the patients' baseline serum IgG4 and IgG levels with the severity of bile duct lesions and the number of other coexisting IgG4-RDs were analyzed. Results: Forty-one patients underwent MRCP examinations, and the following types of IgG4-SC were identified: type Ⅰ in 28 cases, type Ⅱa in 11, type Ⅲ in 1, and type Ⅳ in 1. Extrahepatic bile duct stenosis was funnel-shaped in 37 cases and truncated in 4 cases. Moreover, all the stenotic segments were long (≥1.0 cm) and one diverticulum-like outpouching was seen in the pancreatic segment stenosis. Upstream bile ducts of the stenosis showed dilatation in 37 cases, while the other 4 cases did not show this. Contrast-enhanced MRI and CT examinations showed continuous thickening of the extrahepatic bile duct walls in 42 cases, and diffuse thickening of the intrahepatic bile duct walls was simultaneously observed in 15 cases among them. The thickness of the bile duct walls was uniformly concentric. Meanwhile, other accompanying IgG4-RDs included AIP in 50 cases, kidney involvement in 19, salivary gland involvement in 7, retroperitoneal fibrosis in 5, liver involvement in 4, lung involvement in 4, prostate involvement in 2, sclerosing mediastinitis in 2, thickened gallbladder wall (without stones) in 20, and enlarged upper abdominal lymph nodes in 15 cases. Moreover, higher baseline serum IgG4 and IgG levels were positively correlated with the number of other coexisting IgG4-RDs, but not with the bile duct wall thickness and stenotic segment length. Conclusions: Localized stenosis of the bile ducts with dilatation or non-dilation of the upstream bile ducts, as well as diffuse thickening of the bile duct walls, are the MRI and CT features of newly diagnosed patients with IgG4-SC. Furthermore, higher baseline serum IgG4 and IgG levels are not related to the severity of the diseased bile ducts but are related to the number of other coexisting IgG4-RDs. -
计算机断层成像(computed tomography,CT)是应用最为广泛的医学成像模态,由于其过高的X射线辐射剂量可能存在诱发癌症的风险。因此,低剂量CT成为当前研究的热点。目前,低剂量CT有两种实现方法,一种是降低每个投影角度下的辐射剂量,另一种是在稀疏角度下减少投影个数。在稀疏投影角度下重建的图像就是稀疏重建,其中以滤波反投影(filtered back projection,FBP)[1]算法为代表的解析法,是一类经典的CT图像重建算法。然而FBP算法稀疏重建的图像产生严重的条状伪影,可能导致出现错误的疾病判读,基于此,研究者们开始设计新的高精度稀疏重建算法,以压制条状伪影。
CT稀疏重建方法大致分为两类。一类方法是基于压缩感知(compressed sensing,CS)[2]的迭代法,2006年以来,Sidky等[3-4]提出了扇束和锥束CT的总变差(total variation,TV)最小算法,实现了高精度CT稀疏重建。随后,研究者们在TV算法的基础上,提出了自适应加权TV(adaptive-weighted total variation,awTV)[5]、保边TV(edge-preserving TV,EPTV)[6]、各向异性TV(anisotropic TV,aTV)[7]、高阶TV(high order TV,HOTV)[8]、非局部TV(non-local TV,NLTV)[9]及TpV(total p-variation,TpV)[10-11]等算法,进一步提高了重建精度,有力地推动了CT稀疏重建的发展。此外,其他基于压缩感知的重建算法也得到了深入研究,如基于字典学习的方法[12]和基于秩最小的方法[13]。
另一类方法是深度学习法。Chen等[14]提出的RED-CNN网络,结合了反卷积[15]和残差学习[16],在CT稀疏重建方面取得了不错的效果。Wolterink等[17]使用生成式对抗网络(generative adversarial networks,GAN)[18]在CT稀疏重建问题上也获得了很大的提升。Han等[19]证明学习条状伪影比学习原始信号更加简单,并提出了基于Unet网络[20-21]的深度残差学习方法来估计条状伪影,然后通过输入的含条状伪影的CT图像减去估计的条状伪影来获得高质量的CT图像。Jin等[22]提出的FBPConvNet网络将残差UNet网络和FBP算法结合起来解决稀疏重建中出现的条形伪影问题,并将该方法与传统的TV方法进行对比,取得了不错的效果。
Zhang等[23]提出的DD-Net网络结合密集连接[24]和反卷积,通过特征复用克服了梯度消失和梯度爆炸以及模型参数大小增加等问题,让网络结构进一步的压缩从而更容易训练,提高了网络训练的性能。Han等[25]揭示了Unet网络可能会产生模糊边缘的缺陷,提出了基于UNet的多分辨率深度学习网络结构:多级结构UNets和轻量级结构UNets,增强了图像的高频特征,并论证了该网络压制伪影的性能优于传统的TV算法。Steven等[26]提出的FD-UNet网络在UNet网络的收缩和扩展路径中均引入密集连接来抑制条状伪影,进一步实现高精度稀疏重建。
在这些利用深度学习的图像处理中,ResNet网络中残差连接可以在训练更深网络的同时,又能保证良好的性能。一定程度上解决了深度神经网络存在的退化问题和梯度消失、梯度爆炸的问题[16]。密集连接增加了浅层网络的特征映射在深层网络中的复用,提升了网络的表达能力[24];注意力机制通过对空间或通道信息进行加权,强调有用信息,提升了网络性能[27];对抗机制通过两个不同网络的博弈达到纳什均衡,在计算机视觉方面取得了良好的效果[18]。
本文拟在经典UNet网络的基础上,引入残差连接、密集连接、注意力机制和对抗机制,提出一种对抗式残差密集深度神经网络,用于压制由解析法FBP稀疏重建产生的条状伪影,以期进一步提高CT稀疏重建的精度。
1. GAN模型
GAN[18]网络被广泛应用于图像处理的各个领域。GAN由生成网络G(generator,G)和判别网络D(discriminator,D)两个网络构成,生成网络G用来生成图像,判别网络D用来判别图像的真假。标准GAN模型的目标函数为:
$$ \underset{G}{{\rm{min}}}\;\underset{D}{{\rm{max}}}V(D,G)={E}_x\sim{P}_{{\rm{data}}}\left(x\right)\Big(\mathit{{\rm{log}}}D\left(x\right)\Big)+{E}_z\sim{P}_{z}\left(z\right)\bigg(\mathit{{\rm{log}}}\Big(1-D\big(G\left(z\right)\big)\Big)\bigg), $$ (1) 其中
$G$ 为生成器;$ D $ 为判别器;$ z $ 为噪声,服从高斯分布;${P}_{{\rm{data}}}\left(x\right)$ 为真实数据$ x $ 服从的概率分布;$ {P}_{z}\left(z\right) $ 为$ z $ 服从的概率分布;$ {E}_{x} $ 和$ {E}_{z} $ 为期望值。对抗式残差密集网络的框架图如图1所示。在训练过程中,对抗式残差密集网络分别迭代训练残差密集生成网络和判别网络,从而达到纳什均衡,以压制条状伪影。2. 网络结构设计
2.1 残差密集生成网络结构
残差密集生成网络原理是将FBP算法稀疏重建的含条状伪影的CT图像作为输入,经过残差密集生成网络训练后,得到高精度CT图像。残差密集生成网络基于经典UNet进行了改进,残差密集生成网络结构如图2所示,网络结构以大小为256×256的CT图像作为输入,在U型结构的左侧,第1个卷积单元(这里将每次下采样后到下一次下采样之前的卷积操作称作1个卷积单元)包含一个通道数为32的3×3卷积层、BN(batch normalization)层、ReLU (Rectified linear unit)激活层和RAD块(residual attention-based dense block)等操作,其余4个卷积单元只包含RAD块操作。
在U型结构的右侧,每一次上采样之后的输出与U型结构左侧相同大小的特征映射图进行拼接,之后进行1×1卷积层、BN层、ReLU激活层和RD块(residual dense block)等操作。1×1卷积将输入的特征图的通道数减少为原来的1/4倍,RD块操作将输入的特征图通道数转换为原来的2倍。其中,上采样过程中转置卷积操作卷积核大小为4×4,步长为2,padding为1。
最后一个卷积单元的最后一层是通道数为1的1×1卷积层,用来输出图像。在U型结构的输入和输出之间加入了残差连接。这样,整个深度网络实际上是在学习含条状伪影图像到条状伪影图像的映射。
一种输入为32通道输出为64通道的RAD块如图3所示,它是整个网络第1单元中的RAD块,其余单元中的RAD块有类似结构。在图3中,RAD块包含6个单元。前4个单元构成密集连接块,具体的特征映射图变化流程如图3所示。
第5个单元是一个通道注意力模块,如图4所示。它通过学习到一个64×1的通道注意力权重,并将之与输入的通道数为64的特征映射图相乘,获得特定通道被加强的特征映射图。第6个单元是1×1卷积层,并在第4个单元与第6个单元之间加入了残差学习。RD块与RAD块的区别是没有第5个单元即注意力模块。
2.2 判别器结构
判别网络结构图如图5所示。判别网络采用4个卷积层,将大小为256×256的高精度CT图像和残差密集生成网络重建的CT图像分别作为网络的输入,然后进行4个卷积操作,4个卷积操作使用3×3大小的卷积核,步长为2。最后一个卷积操作将通道数转换为1,进行输出,通过这样训练的时候可以获取到更多的图像细节。图中n32s2代表卷积层的卷积核的数量为32,步长为2。
2.3 损失函数
本文对抗式残差密集网络采用原始GAN中的交叉熵二分类作为对抗损失,本文的对抗式残差密集网络的损失函数采用内容损失和对抗损失的加权和,内容损失使用
$ {\mathcal{l}}_{2} $ 损失可以获取到更好的效果。内容损失表示为:$$ {L}_{{\rm{Con}}}=\frac{1}{N}\sum _{i=0}^{N}{({y}_{i}-{x}_{i})}^{2}, $$ (2) 其中,
$ i $ 表示图像中像素的索引,$ N $ 为图像的大小, x为残差密集生成网络生成的CT图像,$ y $ 为相对应的高精度CT图像。本文损失函数表示为:$$ L={L}_{{\rm{Con}}}+{L}_{{\rm{adv}}} 。$$ (3) 3. 实验结果与分析
本节主要介绍数据集,网络训练参数设定,以及实验对比分析。实验选取经典的RED-CNN网络、FBPConvNet和FD-UNet网络3种算法作为稀疏重建的算法,来与本文算法进行对比。
3.1 数据集的创建
本文选取了2015幅不同的CT图像进行训练,来自TCIA数据集(https://www.cancerimagingarchive.net/),其中50幅为测试集,50幅为验证集。图像大小为256×256像素。含条状伪影的CT图像通过对高精度CT图像进行Radon变换得到相对应的稀疏投影图像,其中每幅CT图像选择60个投影进行稀疏重建。
3.2 网络训练超参数设定
在实验中,RED-CNN网络、FBPConvNet网络和FD-UNet网络使用
$ {\mathcal{l}}_{2} $ 损失函数。本文提出的对抗式残差密集网络使用$ {\mathcal{l}}_{2} $ 损失与对抗损失加权,其他参数保持一致。其中,所有的网络都使用Adam优化器,epoch为80,学习率为0.0002,batch_size为8。所有的卷积和反卷积滤波器都以均值为0、标准差为0.01的随机高斯分布初始化。3.3 实验平台
实验配置CPU是Inter(R) Xeon(R) CPU E5-2620 v4 @ 2.10 GHz,GPU是NVIDIA Geforce GTX 1080 Ti,使用Keras库,在Python上进行训练,训练时间约为4 h。
3.4 实验结果及分析
3.4.1 稀疏重建算法对比分析
该实验中,输入是在[0,π]范围内等间隔采集60个角度下的投影数据进行稀疏重建的CT图像。在测试集中分别选取两幅CT图像不同算法测试结果如图6和图7所示,将本文提出的方法与经典的RED-CNN、FBPConvNet和FD-UNet三种算法进行实验对比,实验结果表明,FBP稀疏重建的CT图像具有明显的条状伪影,其他3种经典稀疏重建算法都有效地压制了条状伪影,并取得了较好的效果,但图像中仍然存在一些明显的条状伪影,而本文提出的对抗式残差密集网络重建图像较为清晰,在去掉条状伪影的同时保留了更多的图像细节。
对于定量分析,本文采用峰值信噪比(PSNR)、均方根误差(RMSE)和结构相似性(SSIM)作为CT图像稀疏重建效果的评价指标,结果如表1所示。本文方法与经典的RED-CNN、FBPConvNet和FD-UNet三种方法相比,第1幅CT图像PSNR 高出 FBPConvNet网络大概1 dB,RMSE降低了将近0.002,与FD-UNet网络相比,SSIM略微领先。第2幅CT图像中本文方法指标也优于其他的稀疏重建方法。实验结果表明,本文提出的方法与经典的RED-CNN、FBPConvNet和FD-UNet三种算法相比,该方法保留的细节信息更多,重建出的CT图像精度更高。
表 1 稀疏重建结果的RMSE、SSIM和PSNR分析Table 1. RMSE, SSIM and PSNR analysis of sparse-view reconstruction results重建方法 FBP RED-CNN FBPConvNet FD-UNet 本文方法 PSNR 22.230 28.800 34.440 35.180 35.240 RMSE 0.077 0.036 0.019 0.017 0.017 SSIM 0.645 0.923 0.967 0.969 0.970 PSNR 19.740 27.210 35.660 35.930 36.150 RMSE 0.103 0.044 0.016 0.016 0.016 SSIM 0.593 0.941 0.981 0.979 0.981 3.4.2 本文算法在不同稀疏情形下的性能分析
为了探索本文提出的对抗式残差密集网络在不同稀疏情形下的重建图像算法的性能,在[0,π]范围内等间隔分别采集15、30和90个角度下的投影数据进行稀疏重建的CT图像作为本文算法的输入进行训练,并进行定性和定量分析。
实验结果如图8所示,在稀疏度为15时,该对抗式残差密集网络稀疏重建的CT图像效果最差,稀疏度为30时重建的图像仍然存在明显的条状伪影,稀疏度为60时,保留的细节信息明显增加,从图8(i)可以看出,90个投影角度下保留的细节信息更多,纹理结构更加明显。对于定量分析,比较结果如表2所示,在90个稀疏角度下重建出的CT图像PSNR比60个稀疏度下重建的CT图像高出将近0.2 dB。实验结果表明,在深度学习去条状伪影过程中,稀疏角度越多的CT图像,在该网络中越容易训练出高精度CT图像。
![]() 图 8 不同稀疏情形下的重建图像对比图Figure 8. Comparison of reconstructed images under different sparsity表 2 不同稀疏度下重建图像的PSNR值、SSIM值、RMSE值Table 2. RMSE, SSIM and PSNR analysis of reconstruction results under different sparsity
图 8 不同稀疏情形下的重建图像对比图Figure 8. Comparison of reconstructed images under different sparsity表 2 不同稀疏度下重建图像的PSNR值、SSIM值、RMSE值Table 2. RMSE, SSIM and PSNR analysis of reconstruction results under different sparsity投影个数 15 30 60 90 PSNR 29.770 31.450 34.690 34.810 RMSE 0.032 0.027 0.018 0.018 SSIM 0.908 0.930 0.964 0.964 4. 结语
在本文提出的对抗式残差密集深度神经网络中,将残差密集生成网络基于经典UNet进行了改进,判别网络提高了网络的表达能力。与经典的RED-CNN、FBPConvNet和FD-UNet三种稀疏重建算法相比,该算法能够有效地恢复图像细节,且重建出的CT图像精度更高。与此同时,稀疏角度越多,该网络越容易训练出高精度CT图像,说明该网络在提高CT图像高精度稀疏重建方面具有很大的潜力。
未来的研究方向将基于此网络架构的压制条状伪影网络进行改进,进一步提高CT图像稀疏重建的精度。现在,我们正将此网络应用于电子顺磁共振稀疏重建中,评估其在此成像模态下的性能。
-
![]()
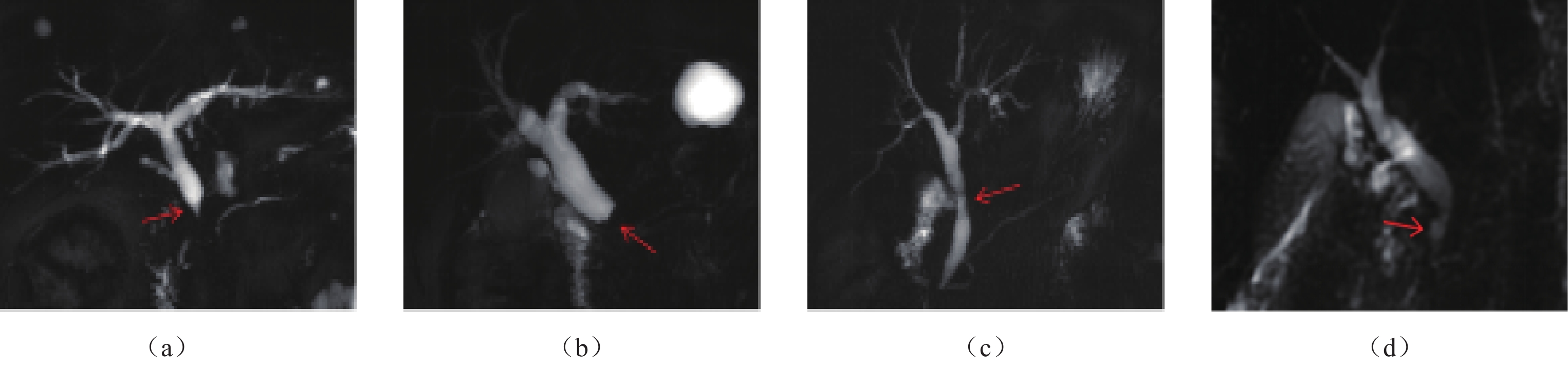
图 1 初诊IgG4-SC患者MRCP分型表现
(a)~(d)分别显示Ⅰ~Ⅳ型IgG4-SC。(a)图为Ⅰ型,胆总管下段狭窄(箭),其上游肝内外胆管扩张。(b)图为Ⅱa型,胆总管下段及肝内胆管多发狭窄(箭),狭窄上游肝内外胆管扩张。(c)图为Ⅲ型,胆总管下段和肝门部胆管狭窄(箭),其上游胆管扩张。(d)图为Ⅳ型,肝门部胆管狭窄(箭),肝内胆管梗阻性扩张。
Figure 1. MRCP classifications of IgG4-SC in newly diagnosed patients
![]()
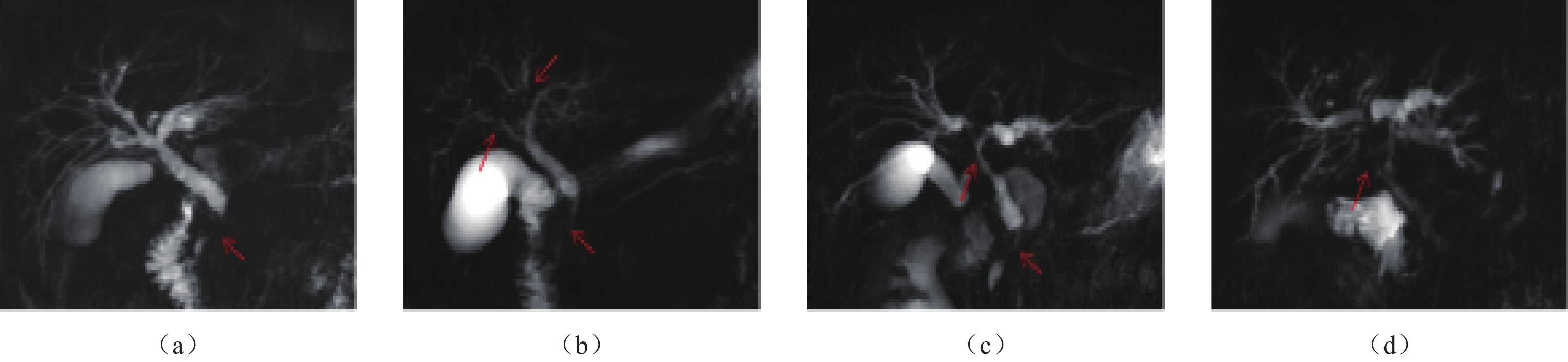
图 2 初诊IgG4-SC患者MRCP狭窄端及狭窄段形态
(a)图显示肝外胆管狭窄端呈漏斗状(箭),狭窄段较长且管腔断续可见。(b)图显示狭窄端呈截断状,狭窄段管腔不可见(箭)。(c)图显示肝外胆管胰上段狭窄,管腔粗细不均(箭)。(d)图显示肝外胆管胰腺段狭窄伴邻近十二指肠侧憩室样外凸(箭)。
Figure 2. Morphologic patterns of the stenotic end and segment of IgG4-SC in newly diagnosed patients on MRCP
![]()
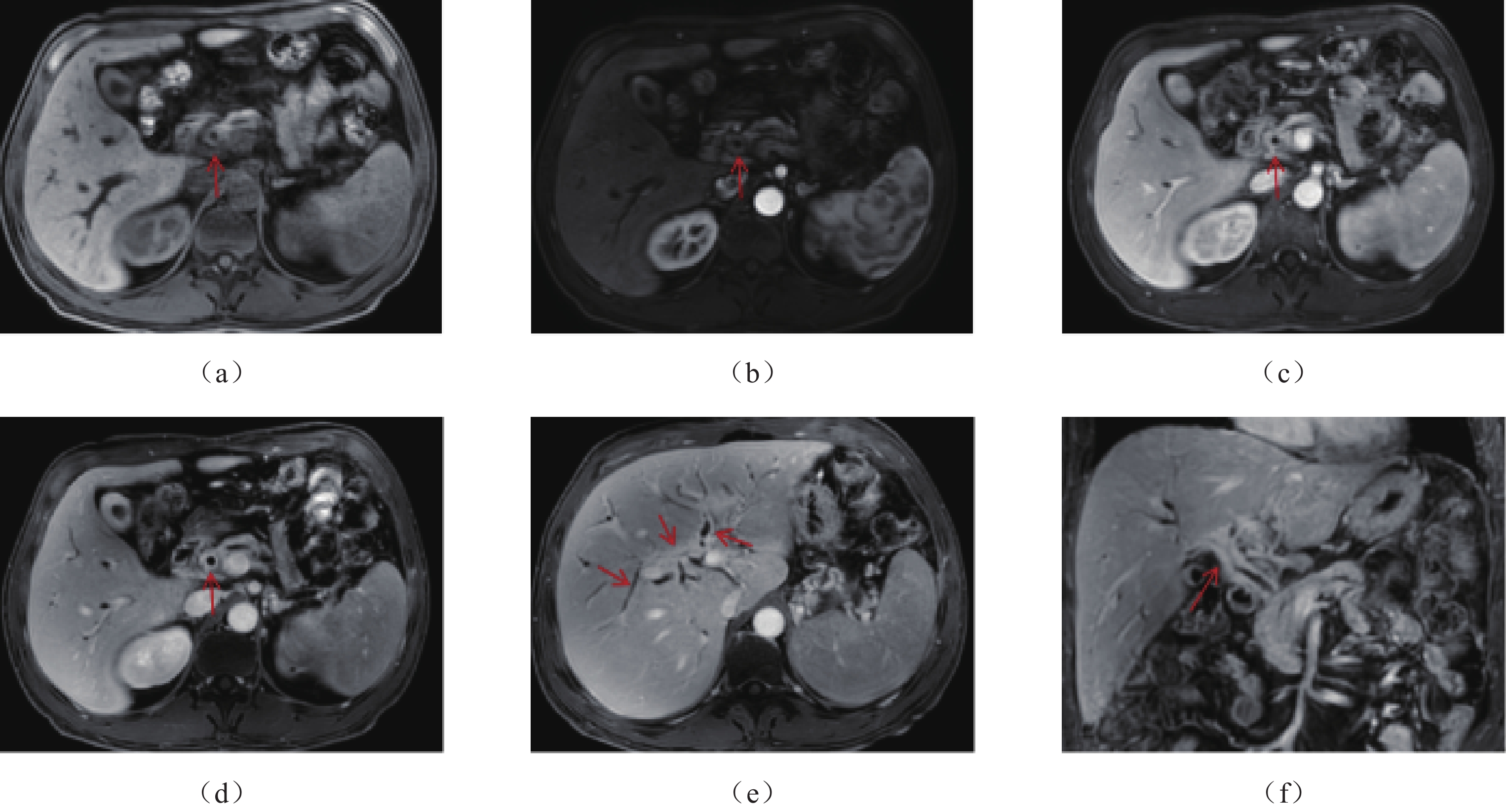
图 3 51岁,男性,初诊IgG4-SC患者增强MRI表现
(a)~(d)分别为轴面T1WI的蒙片、动脉期、门静脉期、延迟期图像,可见肝外胆管壁均匀向心性增厚及渐进性强化(箭),同时见胆囊壁增厚及异常强化。(e)为肝内胆管层面的轴面T1WI延迟期,(f)为冠状面T1WI延迟期,可见肝内、外胆管壁弥漫性增厚及明显强化(箭),肝内胆管扩张。
Figure 3. Contrast-enhanced MRI findings of IgG4-SC in a newly diagnosed 51-year-old male patient
表 1 IgG4-SC患者血清IgG4、IgG升高与影像表现的相关性分析
Table 1 Correlation analysis between elevated serum IgG4 and IgG levels and imaging findings in patients with IgG4-SC
影像表现 血清IgG4升高 血清IgG升高 r P r P 肝外胆管狭窄段长度 -0.348 0.070 -0.086 0.717 管壁厚度MRI测量 0.208 0.271 0.209 0.363 管壁厚度CT测量 0.247 0.416 0.655 0.078 合并其他IgG4-RD的数量 0.613* 0.000 0.524* 0.003 注:*为P<0.01,相关性显著。  下载: 导出CSV
下载: 导出CSV
-
[1] LOHR J M, VUJASINOVIC M, ROSENDAHL J, et al. IgG4-related diseases of the digestive tract[J]. Nature Reviews Gastroenterology and Hepatology, 2021. DOI: 10.1038/s41575-021-00529-y.
[2] NAKAZAWA T, KAMISAWA T, OKAZAKI K, et al. Clinical diagnostic criteria for IgG4-related sclerosing cholangitis 2020[J]. Journal of Hepato-Biliary-Pancreatic Sciences, 2021, 28(3): 235−242. DOI: 10.1002/jhbp.913.
[3] OHARA H, OKAZAKI K, TSUBOUCHI H, et al. Clinical diagnostic criteria of IgG4-related sclerosing cholangitis 2012[J]. Journal of Hepato-Biliary-Pancreatic Sciences, 2012, 19(5): 536−542. DOI: 10.1007/s00534-012-0521-y.
[4] SWENSSON J, TIRKES T, TANN M, et al. Differentiating IgG4-related sclerosing cholangiopathy from cholangiocarcinoma using CT and MRI: Experience from a tertiary referring center[J]. Abdominal Radiology, 2019, 44(6): 2111−2115. DOI: 10.1007/s00261-019-01944-1.
[5] YATA M, SUZUKI K, FURUHASHI N, et al. Comparison of the multidetector-row computed tomography findings of IgG4-related sclerosing cholangitis and extrahepatic cholangiocarcinoma[J]. Clinical Radiology, 2016, 71(3): 203−210. DOI: 10.1016/j.crad.2015.10.024.
[6] TOKALA A, KHALILI K, MENEZES R, et al. Comparative MRI analysis of morphologic patterns of bile duct disease in IgG4-related systemic disease versus primary sclerosing cholangitis[J]. American Journal of Roentgenology, 2014, 202(3): 536−543. DOI: 10.2214/AJR.12.10360.
[7] 李安琪, 王屹. IgG4相关性胆管炎CT及MRI影像学诊断与鉴别诊断[J]. 中华消化外科杂志, 2015,14(4): 344−348. doi: 10.3760/cma.j.issn.1673-9752.2015.04.017 LI A Q, WANG Y. CT and MRI for identification and diagnosis of immunoglobulin G4 associated cholangitis[J]. Chinese Journal of Digestive Surgery, 2015, 14(4): 344−348. (in Chinese). doi: 10.3760/cma.j.issn.1673-9752.2015.04.017
[8] 张斌斌, 张洁, 靳二虎, 等. IgG4相关硬化性胆管炎的CT和磁共振胰胆管成像表现[J]. 中国介入影像与治疗学, 2015,12(6): 336−340. DOI: 10.13929/j.1672-8475.2015.06.004. ZHANG B B, ZHANG J, JIN E H, et al. CT and magnetic resonance cholangiopancreatography features of lgG4-related sclerosing cholangitis[J]. Chinese Journal of Interventional Imaging and Therapy, 2015, 12(6): 336−340. DOI: 10.13929/j.1672-8475.2015.06.004. (in Chinese).
[9] 姜畔, 连敏, 李博, 等. 免疫球蛋白G4相关硬化性胆管炎及合并自身免疫性胰腺炎患者的临床观察[J]. 中华肝脏病杂志, 2018,26(6): 415−419. doi: 10.3760/cma.j.issn.1007-3418.2018.06.005 JIANG P, LIAN M, LI B, et al. Clinical observation of isolated immunoglobulin G4-related sclerosing cholangitis and immunoglobulin G4 sclerosing cholangitis combined autoimmune pancreatitis[J]. Chinese Journal of Hepatology, 2018, 26(6): 415−419. (in Chinese). doi: 10.3760/cma.j.issn.1007-3418.2018.06.005
[10] TANAKA A, TAZUMA S, OKAZAKI K, et al. Clinical features, response to treatment, and outcomes of IgG4-related sclerosing cholangitis[J]. Clinical Gastroenterology and Hepatology, 2017, 15(6): 920−926. DOI: 10.1016/j.cgh.2016.12.038.
[11] KEMP W, MAJEED A, MITCHELL J, et al. Management, outcomes and survival of an Australian IgG4-SC cohort: The MOSAIC study[J]. Liver International, 2021, 41(12): 2934−2943. DOI: 10.1111/liv.15036.
[12] NAKAZAWA T, OHARA H, SANO H, et al. Schematic classification of sclerosing cholangitis with autoimmune pancreatitis by cholangiography[J]. Pancreas, 2006, 32(2): 229. DOI: 10.1097/01.mpa.0000202941.85955.07.
[13] 张文, 董凌莉, 朱剑, 等. IgG4相关性疾病诊治中国专家共识[J]. 中华内科杂志, 2021,60(3): 192−206. ZHANG W, DONG L L, ZHU J, et al. Chinese expert consensus on the diagnosis and treatment of IgG4- related diseases[J]. Chinese Journal of Internal Medicine, 2021, 60(3): 192−206. (in Chinese).
[14] KARIM F, LOEFFEN J, BRAMER W, et al. IgG4-related disease: A systematic review of this unrecognized disease in pediatrics[J]. Pediatric Rheumatology, 2016, 14(1). DOI: 10.1186/s12969-016-0079-3.
[15] TANAKA A, MORI M, KUBOTA K, et al. Epidemiological features of immunoglobulin G4-related sclerosing cholangitis in Japan[J]. Journal of Hepato-Biliary-Pancreatic Sciences, 2020, 27(9): 598−603. DOI: 10.1002/jhbp.793.
[16] ALI A H, BI Y, MACHICADO J D, et al. The long-term outcomes of patients with immunoglobulin G4-related sclerosing cholangitis: The Mayo Clinic experience[J]. Journal of Gastroenterology, 2020, 55(11): 1087−1097. DOI: 10.1007/s00535-020-01714-7.
[17] HUGGETT M T, CULVER E L, KUMAR M, et al. Type 1 autoimmune pancreatitis and IgG4-related sclerosing cholangitis is associated with extrapancreatic organ failure, malignancy, and mortality in a prospective UK cohort[J]. The American Journal of Gastroenterology, 2014, 109(10): 1675−1683. DOI: 10.1038/ajg.2014.223.
[18] NAITOH I, KAMISAWA T, TANAKA A, et al. Clinical characteristics of immunoglobulin IgG4-related sclerosing cholangitis: Comparison of cases with and without autoimmune pancreatitis in a large cohort[J]. Digestive and Liver Disease, 2021, 53(10): 1308−1314. DOI: 10.1016/j.dld.2021.02.009.
[19] NOTOHARA K. Histological features of autoimmune pancreatitis and IgG4-related sclerosing cholangitis with a correlation with imaging findings[J]. Journal of Medical Ultrasonics (2001), 2021, 48(4): 581−594. DOI: 10.1007/s10396-021-01148-5.
[20] KIM J H, BYUN J H, LEE S J, et al. Differential diagnosis of sclerosing cholangitis with autoimmune pancreatitis and periductal infiltrating cancer in the common bile duct at dynamic CT, endoscopic retrograde cholangiography and MR cholangiography[J]. European Radiology, 2012, 22(11): 2502−2513. DOI: 10.1007/s00330-012-2507-1.
[21] MADHUSUDHAN K S, DAS P, GUNJAN D, et al. IgG4-relatEd sclerosing cholangitis: A clinical and imaging review[J]. American Journal of Roentgenology, 2019, 213(6): 1221−1231. DOI: 10.2214/AJR.19.21519.
[22] NAITOH I, NAKAZAWA T, HAYASHI K, et al. Comparison of intraductal ultrasonography findings between primary sclerosing cholangitis and IgG4-related sclerosing cholangitis[J]. Journal of Gastroenterology and Hepatology, 2015, 30(6): 1104−1109. DOI: 10.1111/jgh.12894.
[23] NAITOH I, NAKAZAWA T, OHARA H, et al. Endoscopic transpapillary intraductal ultrasonography and biopsy in the diagnosis of IgG4-related sclerosing cholangitis[J]. Journal of Gastroenterology, 2009, 44(11): 1147−1155. DOI: 10.1007/s00535-009-0108-9.
[24] MAEDA E, AKAHANE M, YOSHIOKA N, et al. Comparison of CT findings of biliary tract changes with autoimmune pancreatitis and extrahepatic bile duct cholangiocarcinoma[J]. Japanese Journal of Radiology, 2012, 30(3): 227−234. DOI: 10.1007/s11604-011-0035-6.
[25] LEE Y C, CHON H K, CHOI K H. IgG4-related sclerosing cholangitis involving the gallbladder mimicking a hilar cholangiocarcinoma[J]. Endoscopy, 2022. DOI: 10.1055/a-1778-3393.
[26] HARADA Y, MIHARA K, AMEMIYA R, et al. Isolated IgG4-related cholecystitis with localized gallbladder wall thickening mimicking gallbladder cancer: A case report and literature review[J]. BMC Gastroenterol, 2022, 22(1): 99. DOI: 10.1186/s12876-022-02179-z.
[27] WATANABE K, KAMISAWA T, CHIBA K, et al. Gallbladder wall thickening in patients with IgG4-related diseases, with special emphasis on IgG4-related cholecystitis[J]. Scandinavian Journal of Gastroenterology, 2021, 56(12): 1456−1461. DOI: 10.1080/00365521.2021.1971758.
[28] 丁航, 郑琳琳, 刘源, 等. 自身免疫性胰腺炎及其合并IgG4相关硬化性胆管炎的临床特征和预后比较[J]. 临床肝胆病杂志, 2021,37(4): 888−892. doi: 10.3969/j.issn.1001-5256.2021.04.032 DING H, ZHENG L L, LIU Y, et al. Clinical features and prognosis of autoimmune pancreatitis alone or with IgG4-related sclerosing cholangitis[J]. Journal of Clinical Hepatology, 2021, 37(4): 888−892. (in Chinese). doi: 10.3969/j.issn.1001-5256.2021.04.032
[29] LIN W, LU S, CHEN H, et al. Clinical characteristics of immunoglobulin G4-related disease: A prospective study of 118 Chinese patients[J]. Rheumatology, 2015, 54(11): 1982−1990. DOI: 10.1093/rheumatology/kev203.
[30] KAWASHIRI S, ORIGUCHI T, UMEDA M, et al. Association of serum levels of fibrosis-related biomarkers with disease activity in patients with IgG4-related disease[J]. Arthritis Research & Therapy, 2018, 20(1). DOI: 10.1186/s13075-018-1777-7.
-
期刊类型引用(0)
其他类型引用(2)


























计量
- 文章访问数: 256
- HTML全文浏览量: 137
- PDF下载量: 23
- 被引次数: 2


