
CT Diagnosis of Median Arcuate Ligament Compression Syndrome with Spontaneous Isolated Superior Mesenteric Artery Dissection: A Case Report
-
摘要: 本文探讨1例正中弓状韧带压迫综合征合并肠系膜上动脉夹层的CT表现及转归,多层螺旋CT血管成像三维重建能清晰地观察到腹腔干狭窄程度、侧支循环建立、肠系膜上动脉夹层转归和重塑的动态过程,有助于判断病情,指导临床治疗。Abstract: This article explores the CT findings and outcome of a case involving median arcuate ligament compression syndrome complicated with spontaneous isolated superior mesenteric artery dissection. Three-dimensional reconstruction of multi-detector spiral CT angiography can effectively display the degree of abdominal trunk stenosis, development of collateral circulation, and dynamic process of superior mesenteric artery dissection remodeling. This approach is valuable for evaluating the disease and guiding the clinical treatment.
-
1. 临床资料
患者,男,54岁。因“间断腹痛5 d,加重7 h”入院。5天前进食早餐后出现上腹部隐痛,之后连及后背及脐周,进行性加重为绞痛,伴棕黄色水样便4~5次,无发热恶寒,无恶心呕吐,自行服用2片颠茄片缓解。入院当日早餐后再次出现上腹部撕裂样疼痛,呈持续加重,伴软便及水样便1次,无发热恶寒,遂就诊于我院急诊,给予盐酸哌替啶50 mg止痛后逐渐好转。患者既往体健,无高血压和外伤史。个人史:吸烟30年余,约10支/d;饮酒30年余,约100 g/d。
辅助检查:血压118/83 mmHg,心率59次/min。化验检查:WBC 6.12×109/L,NEUT% 66.7%,Hgb 150 g/L,PLT 226×109/L,PT 12.5 s,FIB 4.17 g/L,APTT 29.7 s,D-D 0.14 mg/L,FDP 1.26 mg/L。床边超声:双下肢深静脉未见血栓。心内结构及血流未见异常,心功能未见异常。诊疗经过:入院后患者采取内科保守治疗,胃肠减压,静脉营养,以罂粟碱注射液60 mg Q8 h解痉,洛赛克40 mg Qd抑酸、善宁0.1 mg Q8 h抑制胃肠道分泌,低分子肝素钠6000 iu Q12 h抗凝治疗2周。出院后患者服用肝素钠1周,因牙龈出血停药,此后患者未服用任何药物,平时注意饮食,戒烟戒酒。
2. 腹部增强CT和CT血管成像(CTA)检查
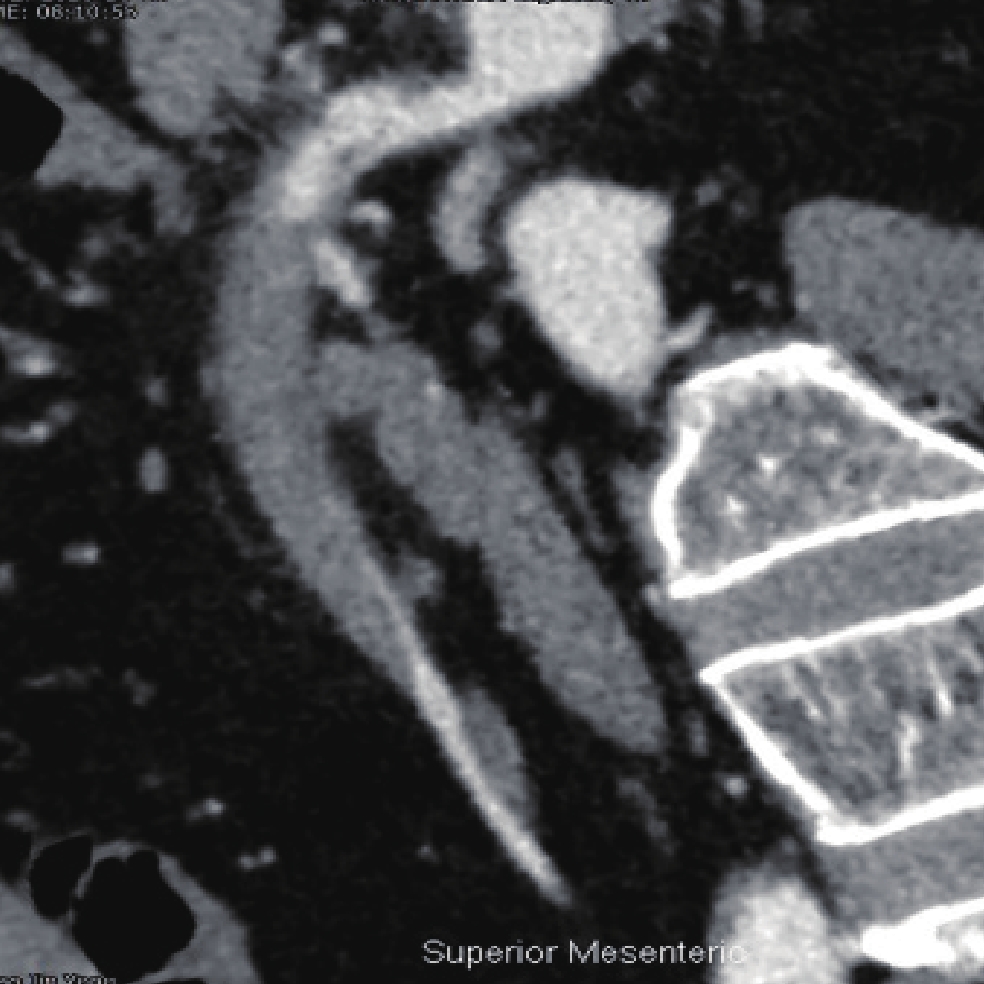
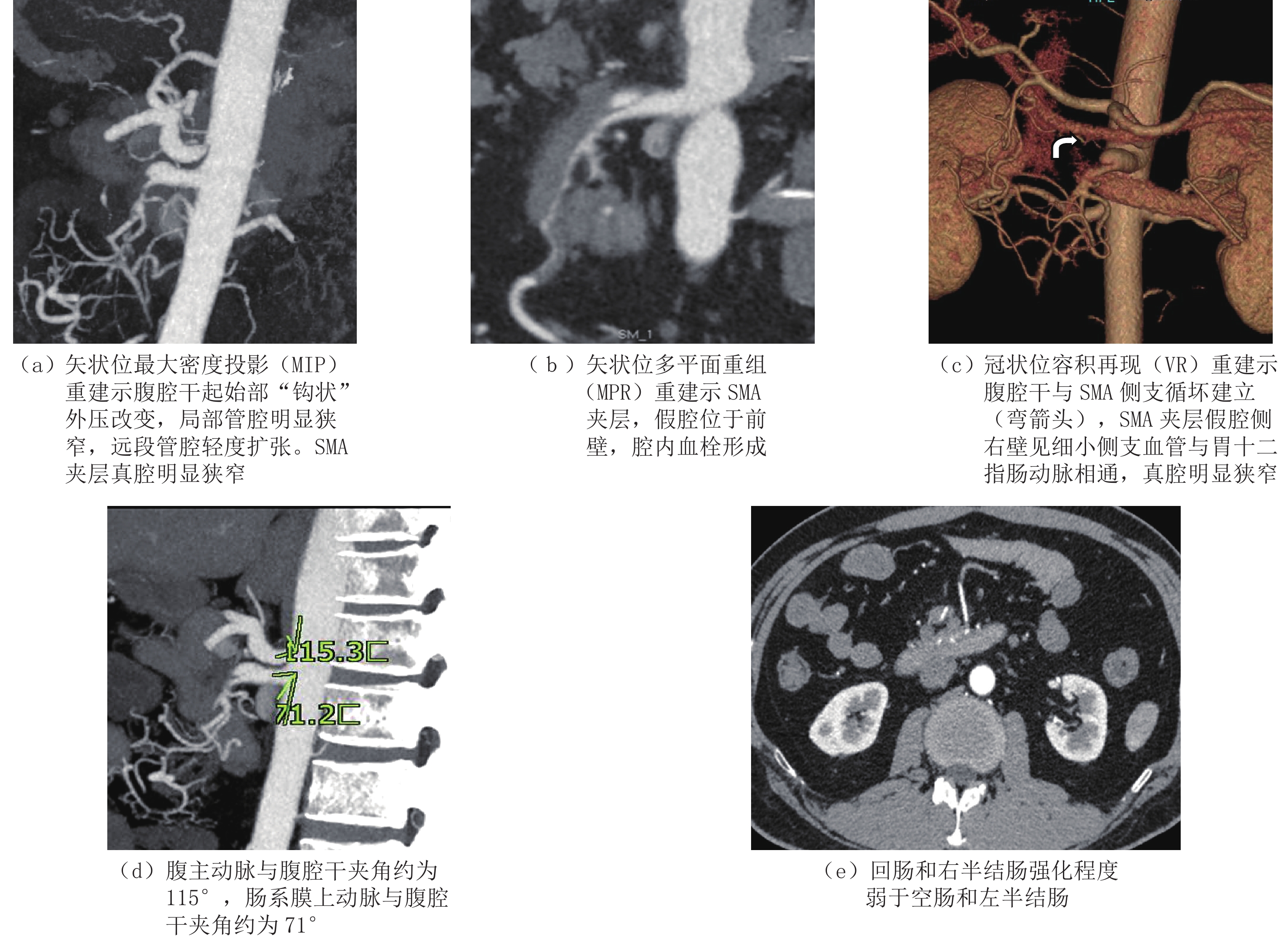
入院当日CTA(图1):肠系膜上动脉(superior mesenteric artery,SMA)近段增粗,可见双层管腔,破口距起始部约15 mm,长径约11 mm;假腔位于前壁,内见血栓,长度约88 mm,累及3大分支,管壁周围可见少许渗出;真腔明显狭窄。腹腔干起始部呈“钩状”凹陷外压改变,并见横行带状影,腹主动脉与腹腔干夹角约115°,肠系膜上动脉与腹主动脉夹角约为71°,管腔重度狭窄,狭窄处宽约2.4 mm,长径约7 mm,其远段管腔轻度扩张。腹腔干与SMA之间侧支循坏形成,SMA夹层假腔的右侧壁见一条细小血管与胃十二指肠动脉相通。其余腹部血管未见夹层征象。回肠和右半结肠强化程度弱于空肠和左半结肠,增强扫描回肠的最大CT值约46 HU,同层空肠的最大CT值约78 HU。CT诊断为正中弓状韧带压迫综合征,合并孤立性肠系膜上动脉夹层。
![]() 图 1 入院当日MDCTA显示正中弓状韧带压迫综合征并肠系膜上动脉夹层Figure 1. MDCTA on the admission day shows median arcuate ligament compression syndrome with superior mesenteric artery dissection
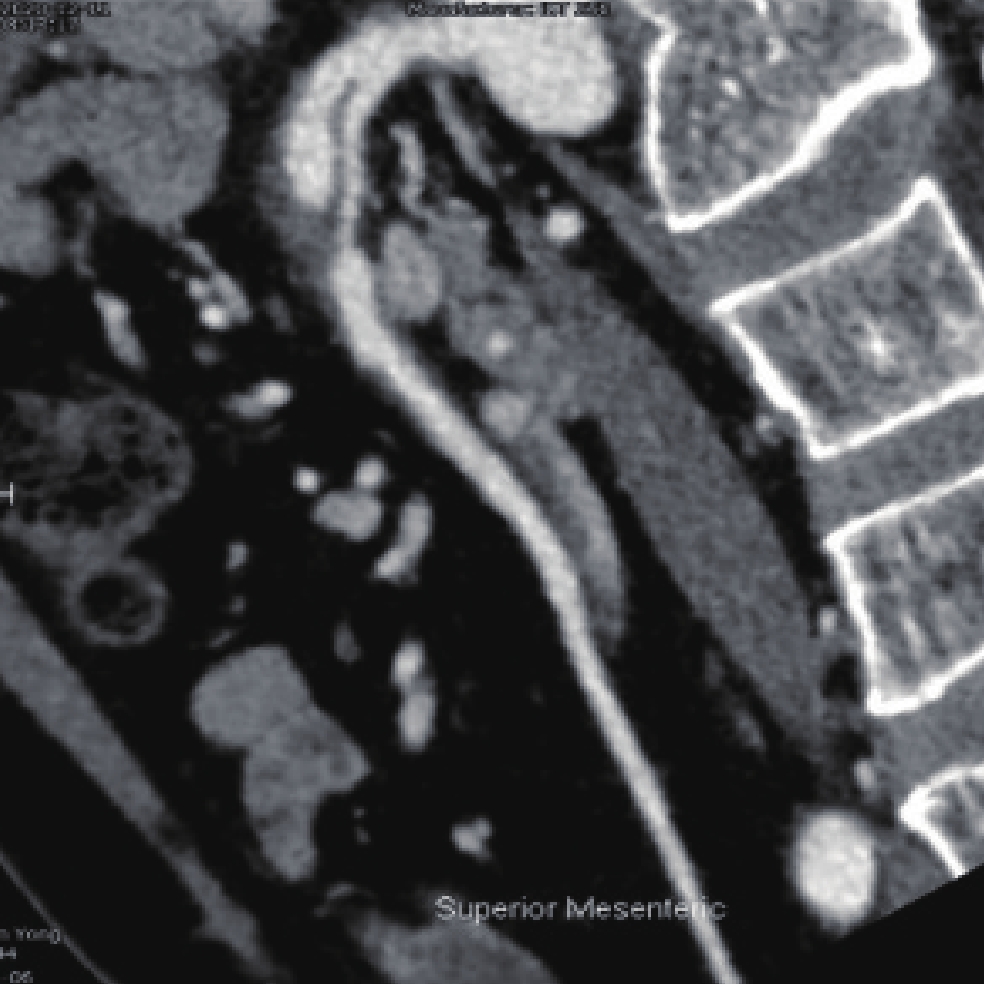
图 1 入院当日MDCTA显示正中弓状韧带压迫综合征并肠系膜上动脉夹层Figure 1. MDCTA on the admission day shows median arcuate ligament compression syndrome with superior mesenteric artery dissection入院后第5日CT显示,SMA夹层的内膜片较前模糊;假腔范围较前增大,形态不规则;假腔内血栓范围较前增大,周围渗出较前吸收。肠管强化程度未见明显减低(图2)。
![]() 图 2 入院第五日矢状位MPR重建示夹层内膜片模糊,假腔范围增大,形态不规则Figure 2. Sagittal MPR reconstruction on the fifth day post admission shows blurred diaphragms and enlarged pseudolumen, with irregular morphology
图 2 入院第五日矢状位MPR重建示夹层内膜片模糊,假腔范围增大,形态不规则Figure 2. Sagittal MPR reconstruction on the fifth day post admission shows blurred diaphragms and enlarged pseudolumen, with irregular morphology发病后2个月CT显示,SMA近段局限性增粗,内膜片较前清晰,仍见真假腔;假腔呈囊袋状,形态较前规则,假腔内血栓较前明显吸收;真腔较前通畅(图3)。
![]() 图 3 二个月后矢状位MPR重建示假腔呈囊袋状,腔内血栓明显吸收Figure 3. Sagittal MPR reconstruction two months post admission shows a bag-like pseudolumen with obvious thrombus absorption
图 3 二个月后矢状位MPR重建示假腔呈囊袋状,腔内血栓明显吸收Figure 3. Sagittal MPR reconstruction two months post admission shows a bag-like pseudolumen with obvious thrombus absorption发病后8.5个月CT显示,SMA近段局限性增粗,动脉夹层的内膜片和假腔范围较前次CT明显缩小,假腔右侧壁细小的侧支血管较前增粗,假腔内血栓完全吸收(图4)。
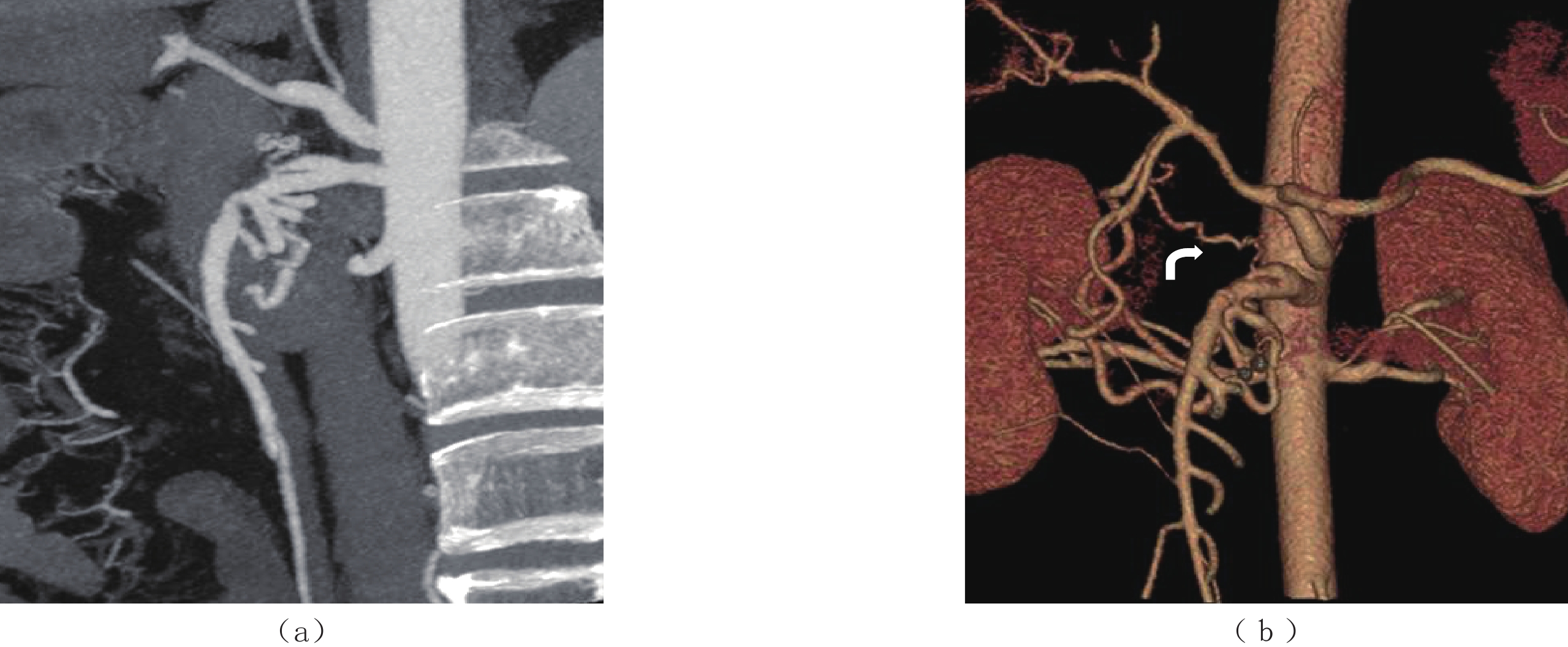
![]() 图 4 8.5个月后薄层MIP(a)和VR(b)重建示假腔缩小,血栓完全吸收,假腔右侧壁侧支血管较前增粗(弯箭头)Figure 4. After 8.5 months of admission, thin-layer MIP (a) and VR (b) reconstruction show reduced pseudolumen, complete thrombus absorption, and dilatated collateral vessels in the right lateral wall of the pseudolumen (curved arrow)
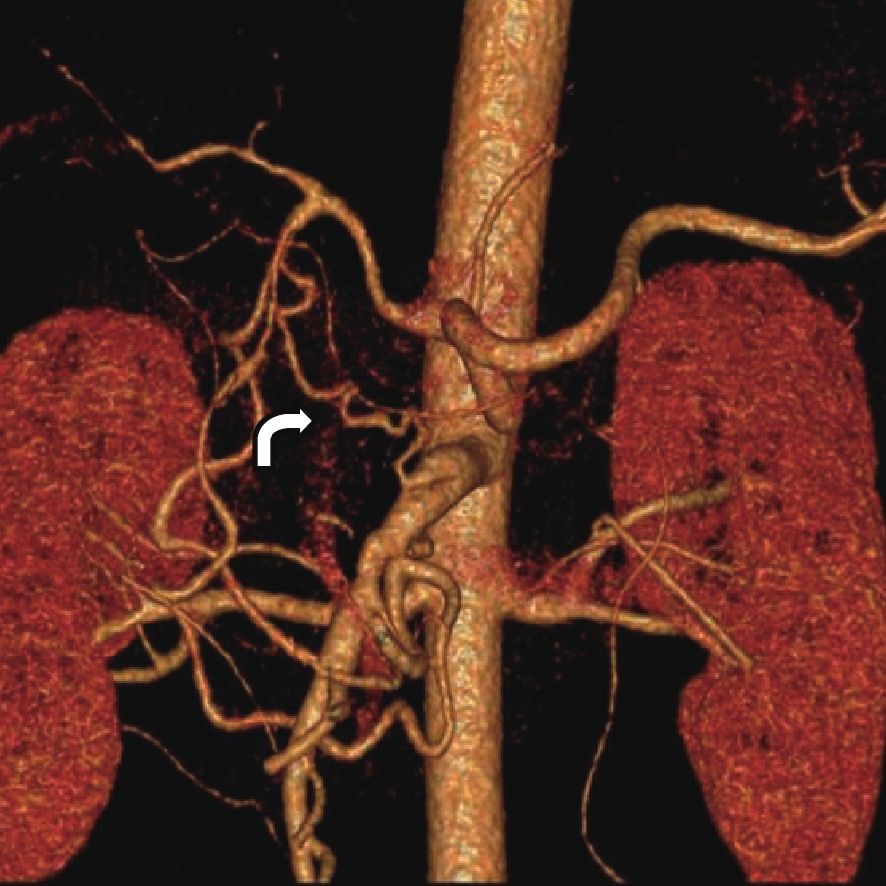
图 4 8.5个月后薄层MIP(a)和VR(b)重建示假腔缩小,血栓完全吸收,假腔右侧壁侧支血管较前增粗(弯箭头)Figure 4. After 8.5 months of admission, thin-layer MIP (a) and VR (b) reconstruction show reduced pseudolumen, complete thrombus absorption, and dilatated collateral vessels in the right lateral wall of the pseudolumen (curved arrow)发病后25个月CT显示,SMA近段局限性增粗,动脉夹层的内膜片和假腔范围与前次CT相仿,假腔右上壁侧支血管进一步增粗,夹层重塑(图5)。
![]() 图 5 25个月后VR重建示假腔右侧壁侧支血管(弯箭头)进一步增粗,夹层重塑Figure 5. VR reconstruction 25 months post admission shows further dilatation of collateral vessels in the right lateral wall of the pseudolumen (curved arrow) and remodeling of the dissection
图 5 25个月后VR重建示假腔右侧壁侧支血管(弯箭头)进一步增粗,夹层重塑Figure 5. VR reconstruction 25 months post admission shows further dilatation of collateral vessels in the right lateral wall of the pseudolumen (curved arrow) and remodeling of the dissection3. 讨论
正中弓状韧带(median arcuate ligament,MAL)综合征,也称为腹腔动脉压迫综合征,是由于正中弓状韧带的膈肌脚附着点过低或腹腔干在腹主动脉的起始位置过高,弓状韧带压迫腹腔干,尤其是在呼气期间,致使腹腔干狭窄及远段局限性管腔扩张,引起了严重临床症状,称为正中弓状韧带压迫综合征(median arcuate ligament compression syndrome,MALS)。这是一种少见的疾病。临床表现包括体重减轻、慢性餐后腹痛、恶心、呕吐和腹泻,这些症状被认为是间歇性肠缺血的继发症状。部分患者可以表现为慢性持续性上腹疼痛,向患者左侧腹部或背部放射。深呼气会加剧腹部疼痛,而吸气可以减轻疼痛。深吸气通过将腹腔动脉和主动脉向尾侧和MAL向腹侧移动,最大限度地减少压迫,降低上腹部疼痛的强度。
MDCT以其方便、血管空间分辨率高以及三维重建等优点,可以准确无创地诊断MALS,并可以显示横膈膜以及横膈膜和腹腔动脉之间的解剖关系。MALS的CTA诊断标准为:①腹腔干近端受外压改变,使血管壁上缘呈“V”形凹陷,严重时呈“钩”形改变,这种特征性的“钩状外观”有助于区分MALS狭窄与动脉粥样硬化狭窄[1];②CT上可观察到腹腔干受前上方的膈肌脚纤维压迫,这是MALS的的直接征象;③吸气末期腹腔干的狭窄程度减轻,而呼气末期腹腔干的狭窄程度加重;④腹腔干与肠系膜上动脉有不同程度的侧支循环血管形成[2]。本例MALS患者影像学特征符合上述诊断标准,腹腔干与肠系膜上动脉侧支交通属于胰十二指肠动脉弓型,与相关文献报道的CTA表现相似[3-4]。
孤立性肠系膜上动脉夹层(isolated superior mesenteric artery dissection,ISMAD)是指血管夹层仅发生于肠系膜上动脉(superior mesenteric artery,SMA),但不合并腹主动脉夹层。ISMAD经常在SMA近端1~3 cm之间,假腔常发生于SMA前壁(98.1%),其余好发生于SMA的右侧壁,夹层的平均长度为6.3 cm(1.1~20.6 cm)[5]。ISMAD的确切病因目前还不清楚,可能与动脉硬化、高血压、外伤、肌纤维发育不良等因素有关。
有研究对该病提出“剪切应力损伤”学说,认为SMA起始段走行于胰腺的后方,并被周围组织包裹,使其位置相对固定,但是SMA的远端向下弯曲走行于肠系膜内,二者移行部弯曲程度大,并且可随体位和活动出现相对位移。这样就使距SMA开口1.5~3.0 cm处前壁产生特殊的血流剪切力而损伤血管的内膜,导致夹层的发生,此部位正是SMA夹层第一破口的好发位置[6-7]。Wu等[8]研究表明,SMA与腹主动脉之间的夹角是ISMAD的独立危险因素,并且该夹角越大,ISMAD的发病风险就越高。
本例患者出现急性腹痛,CTA诊断为肠系膜上动脉夹层时意外发现MALS。推测本例发病机制为MAL导致腹腔干起始部明显狭窄,SMA血流量增大,即使SMA与腹腔干侧支交通,管腔内压力仍然较大,再加上血流剪切力造成内膜损伤,最终导致血管内膜撕裂,血管夹层形成。ISMAD手术治疗的指征[9-10]包括动脉破裂、动脉瘤扩张(直径>2 cm)、肠梗死、腹膜刺激征阳性以及保守治疗后进行性或持续性腹痛。本例由于缺乏手术指征,采取保守治疗,随访期间本例无肠系膜缺血、SMA动脉瘤和其他动脉夹层形成,保守治疗后无症状。
MDCTA最常用于ISMAD患者的诊断和随访。ISMAD诊断标准:①CTA:SMA显示双腔影,管腔内可见线样间隔(内膜片),假腔中可见对比剂充盈或血栓形成,部分患者可以观察到假腔的入口和出口;真腔可见不同程度的受压变窄,甚至闭塞。②平扫:SMA管径增粗,管腔内见环状偏心性或新月形高密度影,与同层主动脉CT值比较增高10~20 HU,增强扫描后未见强化,提示假腔内有血栓及壁间血肿形成;周围脂肪间隙模糊,提示病变具有活动性[11-14]。
ISMAD的影像表现类型,推荐使用Yun等[15]的分型,共分3型:显示真腔和假腔,其中假腔可以看到入口以及出口为Ⅰ型;显示假腔的入口但未显示出口为Ⅱ型(假腔无血栓形成,即假腔盲袋为Ⅱa型;假腔内未见血流,即血栓形成性假腔为Ⅱb型);Ⅲ 型:SMA夹层伴闭塞。本例初始形态学为Ⅱb型,经内科保守治疗后转为Ⅱa型,随访过程中发现胃十二指肠动脉与SMA夹层假腔侧壁的交通血管逐渐增粗,最终SMA夹层重塑。
本例患者正中弓状韧带压迫综合征合并肠系膜上动脉夹层在临床实属罕见,MDCTA三维重建能清晰地观察到腹腔干狭窄程度、侧支循环建立、肠系膜上动脉夹层转归和重塑的动态过程,有助于判断病情,指导临床治疗[16-18]。
-
![]()
图 1 入院当日MDCTA显示正中弓状韧带压迫综合征并肠系膜上动脉夹层
Figure 1. MDCTA on the admission day shows median arcuate ligament compression syndrome with superior mesenteric artery dissection
![]()
图 2 入院第五日矢状位MPR重建示夹层内膜片模糊,假腔范围增大,形态不规则
Figure 2. Sagittal MPR reconstruction on the fifth day post admission shows blurred diaphragms and enlarged pseudolumen, with irregular morphology
![]()
图 3 二个月后矢状位MPR重建示假腔呈囊袋状,腔内血栓明显吸收
Figure 3. Sagittal MPR reconstruction two months post admission shows a bag-like pseudolumen with obvious thrombus absorption
![]()
图 4 8.5个月后薄层MIP(a)和VR(b)重建示假腔缩小,血栓完全吸收,假腔右侧壁侧支血管较前增粗(弯箭头)
Figure 4. After 8.5 months of admission, thin-layer MIP (a) and VR (b) reconstruction show reduced pseudolumen, complete thrombus absorption, and dilatated collateral vessels in the right lateral wall of the pseudolumen (curved arrow)
-
[1] HORTON K M, TALAMINI M A, FISHMAN E K. Median arcuate ligament syndrome: Evaluation with CT angiography[J]. Radiographics, 2005, 25(5): 1177−1182. doi: 10.1148/rg.255055001
[2] GÜMÜ H, GÜMÜ M, TEKBA G, et al. Clinical and multidetector computed tomography findings of patients with median arcuate ligament syndrome[J]. Clinical Imaging, 2012, 36(5): 522−525. doi: 10.1016/j.clinimag.2011.11.031
[3] 陈奇元, 杨萍, 张鹏天, 等. 正中弓状韧带压迫腹腔干综合征伴侧支循环形成1例[J]. 医学影像学杂志, 2022,32(8): 1448−1449. CHEN Q Y, YANG P, ZHANG P T, et al. MSCTA findings of celiac trunk syndrome with collateral circulation formed by compression of median arcuate ligament: One case report[J]. Journal of Medical Imaging, 2022, 32(8): 1448−1449. (in Chinese).
[4] 秦甜甜, 王盼, 于晓辉. 正中弓状韧带压迫综合征1例并文献复习[J]. 疑难病杂志, 2022,21(3): 307−308. doi: 10.3969/j.issn.1671-6450.2022.03.020 QIN T T, WANG P, YU X H. Median arcuate ligament syndrome. one case report and literature review[J]. Chinese Journal of Difficult and Complicated Case, 2022, 21(3): 307−308. (in Chinese). doi: 10.3969/j.issn.1671-6450.2022.03.020
[5] 中国医师协会介入医师分会外周血管介入专业委员会. 孤立性肠系膜上动脉夹层诊治专家共识[J]. 中华放射学杂志, 2021,55(4): 352−358. doi: 10.3760/cma.j.cn112149-20200506-00649 Chinese College of Interventionalists Committee on Peripheral Vascular Intervention. Expert consensus on the management of isolated superior mesenteric artery dissection[J]. Chinese Journal of Radiology, 2021, 55(4): 352−358. (in Chinese). doi: 10.3760/cma.j.cn112149-20200506-00649
[6] SOLIS M M, RANVAL T J, MCFARLAND D R, et al. Surgical treatment of superior mesenteric artery dissecting aneurysm and simultaneous celiac artery compression[J]. Annals of Vascular Surgery, 1993, 7(5): 457−462. doi: 10.1007/BF02002130
[7] 杨进军, 张桂平, 班允清. 孤立性肠系膜上动脉夹层的超声影像学特征及预后分析[J]. 中国超声医学杂志, 2022,38(11): 1268−1271. doi: 10.3969/j.issn.1002-0101.2022.11.018 ZHANG J J, ZHANG G P, BAN Y Q. Analysis of ultrasonographic features and prognosis of isolated superior mesenteric artery dissection[J]. Chinese Journal of Ultrasound in Medicine, 2022, 38(11): 1268−1271. (in Chinese). doi: 10.3969/j.issn.1002-0101.2022.11.018
[8] WU Z, YI J, XU H, et al. The significance of the angle between superior mesenteric artery and aorta in spontaneous isolated superior mesenteric artery dissection[J]. Annals of Vascular Surgery, 2017, 11(45): 117−126.
[9] SATOKAWA H, TAKASE S, SETO Y, et al. Management strategy of isolated spontaneous dissection of the superior mesenteric artery[J]. Annals of Vascular Diseases, 2014, 7(3): 232−238. doi: 10.3400/avd.oa.14-00071
[10] TOMITA K, OBARA H, SEKIMOTO Y, et al. Evolution of computed tomographic characteristics of spontaneous isolated superior mesenteric artery dissection during conservative management[J]. Circulation Journal, 2016, 80(6): 1452−1459. doi: 10.1253/circj.CJ-15-1369
[11] 孙敏, 罗彩华, 苏秦, 等. CT平扫在自发性孤立性肠系膜上动脉夹层诊断中的意义[J]. 医学影像学杂志, 2018,28(1): 113−116. SUN M, LUO C H, SU Q, et al. The significance of non-contrast-enhanced computed tomography scan in the diagnosis of spontaneous isolated superior mesenteric artery dissection[J]. Journal of Medical Imaging, 2018, 28(1): 113−116. (in Chinese).
[12] 曹阿丹, 宋敏, 武乐乐, 等. 正中弓状韧带压迫综合征双源CT血管造影表现[J]. 临床放射学杂志, 2021,40(6): 1235−1238. CAO A D, SONG M, WU L L, et al. Imaging features of dual-source CT angiography of median arcuate ligament compression syndrome[J]. Journal of Clinical Radiology, 2021, 40(6): 1235−1238. (in Chinese).
[13] 黎艳, 李玉民, 刘向华, 等. MSCT在自发性孤立性肠系膜上动脉夹层诊断中的应用[J]. 国际医学放射学杂志, 2021,44(4): 471−475. LI Y, LI Y M, LIU X H, et al. Application of multislice spiral CT in the diagnosis of spontaneous isolated superior mesenteric artery dissection[J]. International Journal of Medical Radiology, 2021, 44(4): 471−475. (in Chinese).
[14] 倪国庆, 苏浩波, 陈国平, 等. 孤立性肠系膜上动脉夹层分型及治疗策略[J]. 介入放射学杂志, 2019,28(7): 701−705. NI G Q, SU H B, CHEN G P, et al. The classification and management strategy of isolated superior mesenteric artery dissection[J]. Journal of Interventional Radiology, 2019, 28(7): 701−705. (in Chinese).
[15] YUN W S, KIM Y W, PARK K B, et al. Clinical and angiographic follow-up of spontaneous isolated superior mesenteric artery dissection[J]. European Journal of Vascular and Endovascular Surgery, 2009, 37(5): 572−577. doi: 10.1016/j.ejvs.2008.12.010
[16] 周喜田, 周卫忠, 刘海日, 等. 胰十二指肠切除术后急性正中弓状韧带压迫综合征介入治疗一例[J]. 中华放射学杂志, 2021,55(9): 989−991. ZHOU X T, ZHOU W Z, LIU H R, et al. Interventional treatment of acute median arcuate ligament syndrome after pancreaticoduodenectomy: A case report[J]. Chinese Journal of Radiology, 2021, 55(9): 989−991. (in Chinese).
[17] 靳明旭, 尤佳, 张娣, 等. 自发孤立性肠系膜上动脉夹层: MSCTA特征及保守治疗后影像学转归[J]. 中国医学计算机成像杂志, 2021,27(2): 136−141. JIN M X, YOU J, ZHANG D, et al. Spontaneous isolated superior mesenteric artery dissection: MSCTA characteristics and radiological outcomes after conservative treatment[J]. Chinese Computed Medical Imaging, 2021, 27(2): 136−141. (in Chinese).
[18] 连利珊, 张喆, 张志文, 等. 自发性孤立性肠系膜上动脉夹层治疗策略的影响因素分析[J]. 国际外科学杂志, 2022,49(6): 427−432. LIAN L S, ZHANG Z, ZHANG Z W, et al. Analysis of influencing factors of therapeutic strategies for spontaneous isolated superior mesenteric artery dissection[J]. International Journal of Surgery, 2022, 49(6): 427−432. (in Chinese).
-
期刊类型引用(2)
1. 李琳琨,杨星烨,李琳杰. 上消化道钡餐造影联合64排螺旋CT对肠系膜上动脉综合征的诊断价值分析. 影像研究与医学应用. 2024(01): 32-35 .  百度学术
百度学术
2. 徐昌民,芦春花,罗艳,李岩,邢姗姗. CT血管成像对肠系膜上动脉压迫综合征的诊断价值. 中国当代医药. 2024(19): 82-85 . 百度学术
其他类型引用(0)
 下载:
下载:
计量
- 文章访问数: 332
- HTML全文浏览量: 156
- PDF下载量: 27
- 被引次数: 2


