
The Diagnosis of Cronkhite-Canada Syndrome with CT Enterography: A Clinical Case Analysis
-
摘要: Cronkhite-Canada综合征(CCS)是一组以胃肠道弥漫性息肉和外胚层变化为特征的综合征,其临床表现主要为慢性腹泻和吸收不良,由于发病率罕见,早期发现和诊断对医生来说是一个挑战。本文报告1例CCS病例,58岁男性,临床表现为慢性水样腹泻、便血、体重减轻和皮肤变化,包括指甲营养不良和色素沉着;实验室检查结果提示贫血和低蛋白血症;CT小肠造影检查发现全消化道黏膜息肉样增生,高度怀疑CCS,随后行内镜检查证实了该诊断。患者经治疗后,症状明显好转,在近1年的随访中,CT小肠造影和内镜检查均提示明显缓解。本文对该疾病进行文献综述,旨在总结其CT小肠造影表现,以提高临床医生对本病的认识,为CCS的早期诊断提供一定的思路。
-
关键词:
- CT小肠造影 /
- 息肉-色素沉着-脱发-指(趾)甲营养不良综合征 /
- 诊断
Abstract: Cronkhite-Canada syndrome (CCS) is a rare cause of chronic diarrhea and malabsorption where patients develop multiple polyps throughout the gastrointestinal (GI) tract, accompanied by ectodermal changes. Due to its rarity, its early detection and diagnosis can be challenging for physicians. This case report described a 58-year-old male patient with CCS who presented with chronic watery diarrhea, hematochezia, weight loss, and skin changes including nail dystrophy and hyperpigmen-tation. Laboratory results showed anemia and hypoalbuminemia. He underwent CT enterography (CTE) which identified diffuse edematous polyposis in the GI tract. The CTE results were highly suspicious of CCS and a subsequent endoscopic examination confirmed the diagnosis. The patient received supportive treatment which improved his symptoms. Based on CTE and endoscopy at 1-year follow-up, the patient was deemed to be in remission. We included a literature review of CCS. The case report aimed to improve the understanding of CCS and explored the key CTE features relevant to its early diagnosis.-
Keywords:
- CT enterography /
- Cronkhite-Canada syndrome /
- diagnosis
-
Cronkhite-Canada综合征(Cronkhite-Canada syndrome,CCS),又称息肉-色素沉着-脱发-指(趾)甲营养不良综合征。由Cronkhite和Canada于1955年首次报道[1],是一组以外胚层异常和胃肠道弥漫性息肉改变为特征伴有蛋白质丢失的非遗传性罕见病[2]。CCS的主要临床表现为脱发、皮肤色素过度沉着和指(趾)甲营养不良,其他突出的症状包括体重减轻、蛋白丢失性肠病、腹泻、腹痛、恶心、呕吐、味觉障碍和萎缩性舌炎[3],主要分布分群为中老年男性[4]。我国相关病例报道仅80余例[5]。
目前临床对CCS认知较少,尚未有文献总结其CT小肠造影(CT enterography,CTE)表现。为提高对CCS的认识,现将我院收治1例CCS患者分析报道,主要对其CTE特点进行归纳和总结。
1. 病历资料
1.1 临床表现与实验室检查
患者男性,58岁,以“反复腹泻合并便血1年,加重2个月”为主诉予入院,伴纳差、乏力、体重减轻。查体毛发稀疏,脸面及全身黑褐色色素沉着,以指(趾)关节为著;指(趾)甲萎缩,甲板从甲床远端虫蚀样脱落(图1)。
![]() 图 1 CCS患者脚趾和手指图像显示指(趾)甲萎缩,甲板从甲床远端虫蚀样脱落,指间关节色素沉着。Figure 1. Images of toes and fingers of the patient with CCS
图 1 CCS患者脚趾和手指图像显示指(趾)甲萎缩,甲板从甲床远端虫蚀样脱落,指间关节色素沉着。Figure 1. Images of toes and fingers of the patient with CCS实验室检查:大便潜血试验阳性,血红蛋白128 g/L,总蛋白45 g/L,白蛋白29 g/L,提示贫血和低蛋白血症。
1.2 CTE表现
观察方面包括息肉的部位、大小、形态、分布、边界、供血动脉、强化方式、并发症、肠管周围及肠系膜淋巴结。
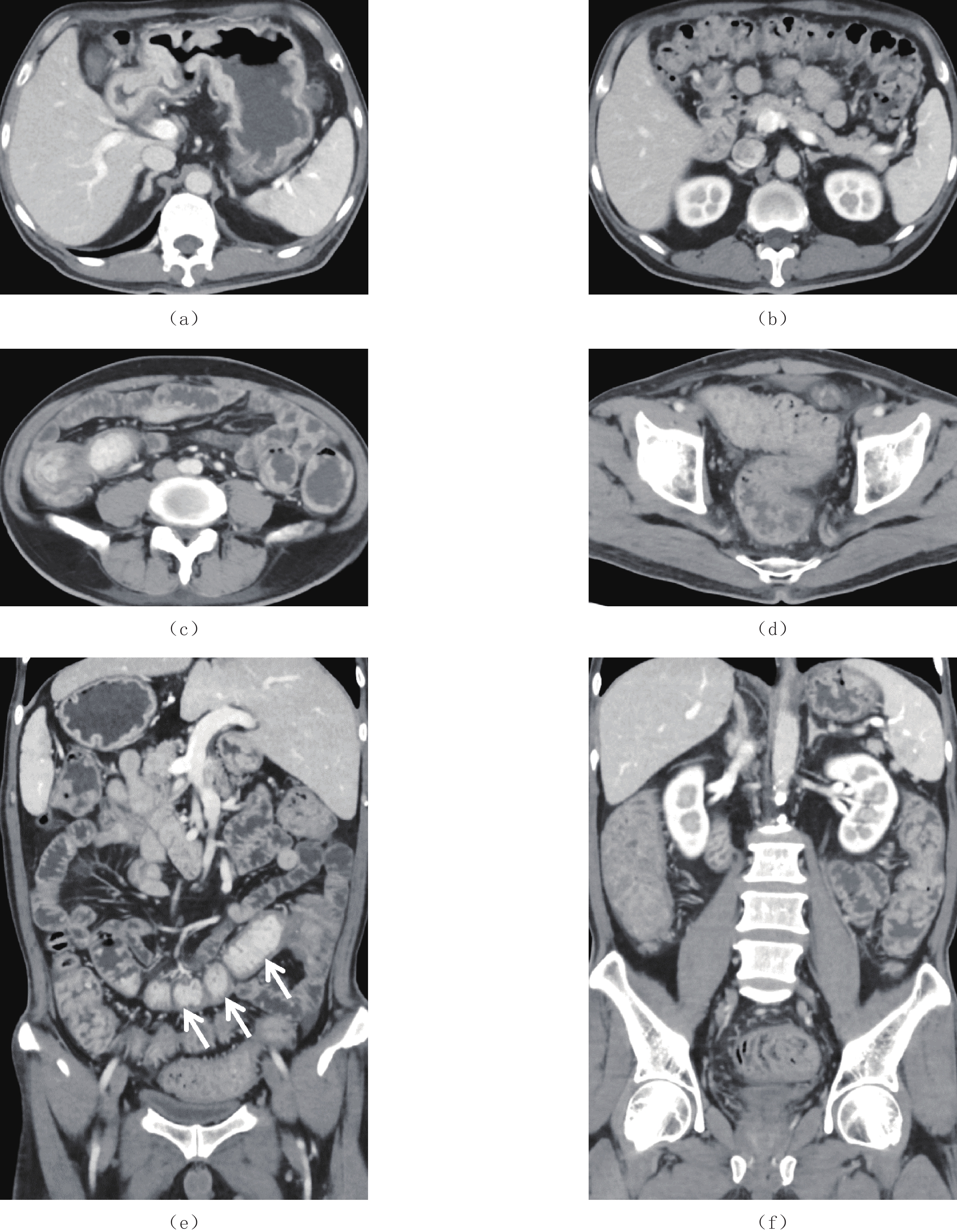
CCS的CT小肠造影表现:①息肉的发病部位除食道外,布满整个消化道;②息肉的大小不等,小者4 mm,大者可达到2 cm,小肠的病变以末端回肠息肉较大,大肠则以右半结肠为著;③息肉的形态呈圆形、椭圆形、指状,基底较宽,蒂并不明显;④息肉呈弥漫性均匀分布、地毯式覆盖整个消化道黏膜;⑤息肉与消化道黏膜分界不清,在胃及末端回肠形成巨大息肉样黏膜皱襞;⑥增强扫描明显强化,末端回肠强化更明显;⑦未见明显肠系膜动脉分支与息肉相连;⑧末端回肠有套入右半结肠趋势,其他部位未见明显套叠改变;未见明显癌变征象;⑨肠腔外脂肪间隙清晰,未见肠系膜淋巴结增大(表1和图2)。
表 1 CCS CTE表现Table 1. CT enterographic features of CCS息肉 CTE特点 部位 胃底、胃体、胃角、胃窦、十二指肠球降段、空肠、回肠下段、末端回肠、回盲部、大肠 大小 大小不等,小者4 mm,大者2 cm,小肠中以末端回肠为著,大肠中以右半结肠为著 形态 椭圆形、指状,基底宽,蒂不明显 分布 弥漫性分布、地毯式覆盖 边界(与黏膜分界) 与黏膜分界不清,形成巨大息肉样黏膜皱襞 供血动脉 未见明显肠系膜供血动脉与其相连 强化方式 明显强化,尤以末端回肠强化更明显 并发症 末端回肠有套入右半结肠趋势,其他部位未见明显套叠;未见明显癌变征象;其他脏器未
见异常肠管周围及肠系膜淋巴结 肠管周围脂肪间隙清晰,未见肠系膜淋巴结增大 ![]() 图 2 CCS患者CTE图像(a)~(d)为静脉期横断面增强图像,依次显示胃体、十二指肠球降段、末端回肠、乙状结肠和直肠黏膜多发息肉样增生,呈弥漫性分布,胃体和末端回肠呈现息肉样黏膜皱襞;(e)和(f)为冠状面重建图像,更加清晰显示息肉分布范围、形态,以末端回肠黏膜息肉样增生强化更明显(白箭)。Figure 2. CT enterographic images of the patient with CCS
图 2 CCS患者CTE图像(a)~(d)为静脉期横断面增强图像,依次显示胃体、十二指肠球降段、末端回肠、乙状结肠和直肠黏膜多发息肉样增生,呈弥漫性分布,胃体和末端回肠呈现息肉样黏膜皱襞;(e)和(f)为冠状面重建图像,更加清晰显示息肉分布范围、形态,以末端回肠黏膜息肉样增生强化更明显(白箭)。Figure 2. CT enterographic images of the patient with CCS1.3 内镜表现
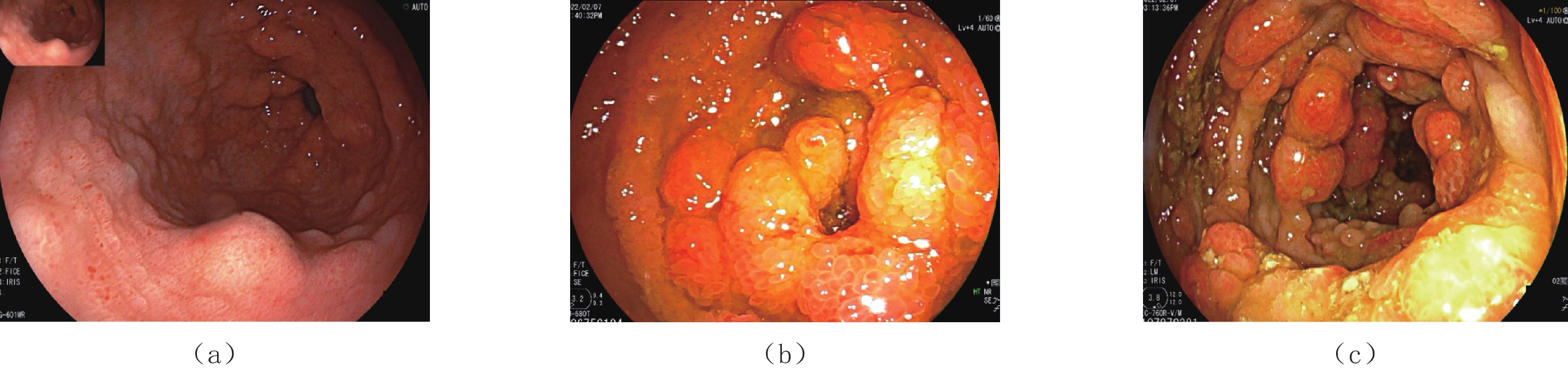
胃镜所见全胃满布息肉样隆起,表面发红,十二指肠球降部多发息肉样隆起;双气囊小肠镜提示回肠下段、大肠多发密集分布息肉样增生,部分为亚蒂,部分为广基,部分头端分叶(图3)。因患者低蛋白血症,未予以活检。
![]() 图 3 CCS患者胃镜和经肛双气囊小肠镜图像(a)~(c)依次为胃体、末端回肠和升结肠,显示黏膜息肉样增生,表面腺体增生间裂,头端充血水肿。Figure 3. Gastroscopic and transanal double balloon enteroscopic images of the patient with CCS
图 3 CCS患者胃镜和经肛双气囊小肠镜图像(a)~(c)依次为胃体、末端回肠和升结肠,显示黏膜息肉样增生,表面腺体增生间裂,头端充血水肿。Figure 3. Gastroscopic and transanal double balloon enteroscopic images of the patient with CCS1.4 治疗
CTE高度提示CCS,内镜检查证实该诊断。给予患者肠外营养及甲强龙冲击,辅以抑酸护胃治疗,后序贯以泼尼松20 mg bid口服,患者腹泻次数明显减少后出院,出院后每2周将泼尼松减量5 mg,患者未再出现腹泻,好转出院。
1.5 随访
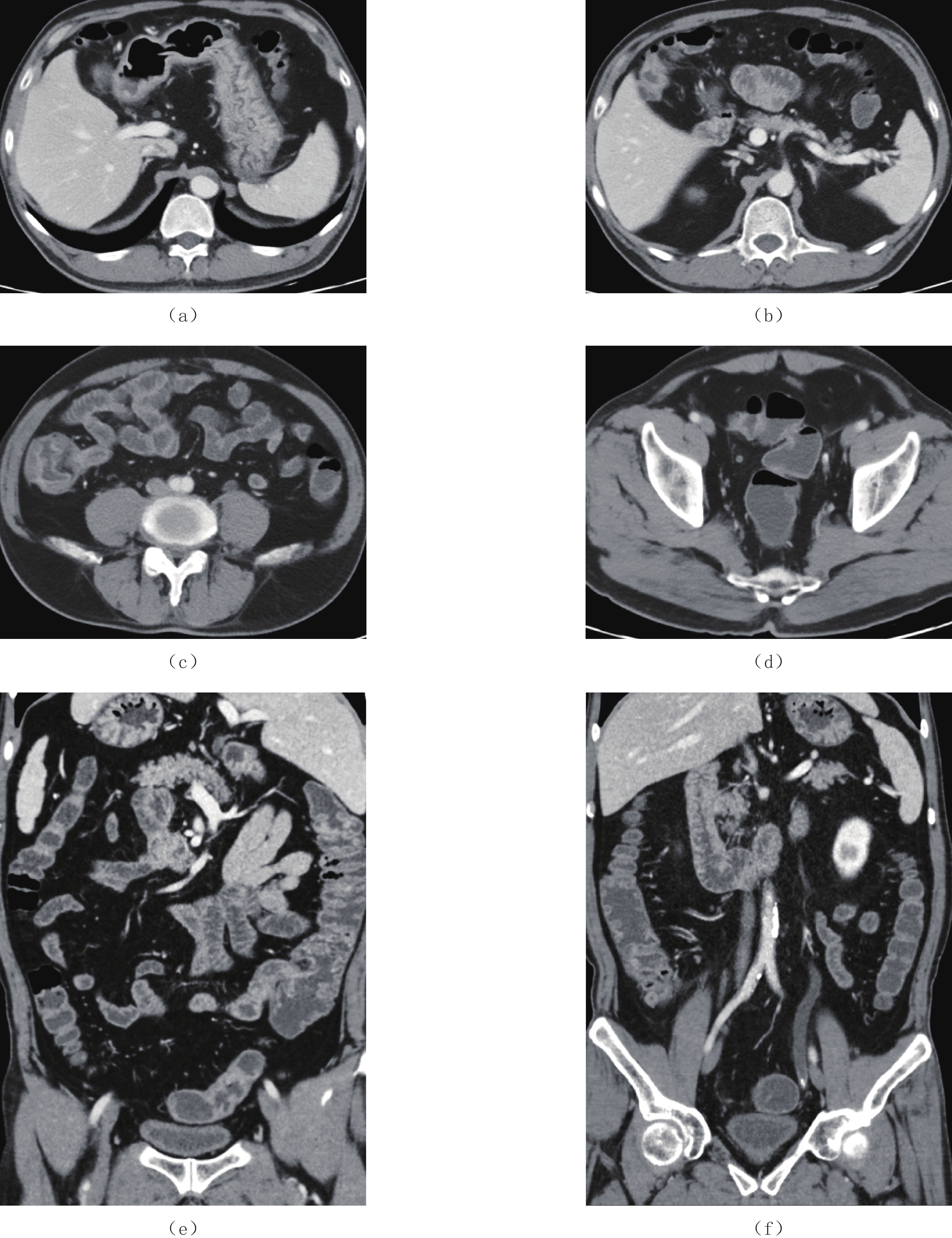
患者在接近1年治疗后,为复查再次收治入院。临床表现无明显不适,血红蛋白、总蛋白和白蛋白均恢复正常水平,实验室检查前后对照见表2。CTE(图4)和内镜均提示明显缓解,并予以内镜下多部位取材活检,均未见癌变,病理图片见图5。
表 2 CCS患者实验室检查结果前后对照Table 2. Laboratory results of the patient with CCS before and after treatment实验室检查项目 第一次入院 随访 血红蛋白/(g/L) 128 141 总蛋白/(g/L) 45 65 白蛋白/(g/L) 29 39 ![]() 图 4 CCS患者治疗后随访CTE图像(a)~(d)为静脉期横断面增强图像,依次显示经过治疗后,胃体、十二指肠球降段、末端回肠、乙状结肠和直肠黏膜多发息肉样增生明显好转,息肉变稀疏甚至消失,部分结肠仍可见黏膜息肉样增生;(e)和(f)为冠状面重建图像,更加清晰显示整个病变范围。Figure 4. CTE images after treatment in patient with CCS
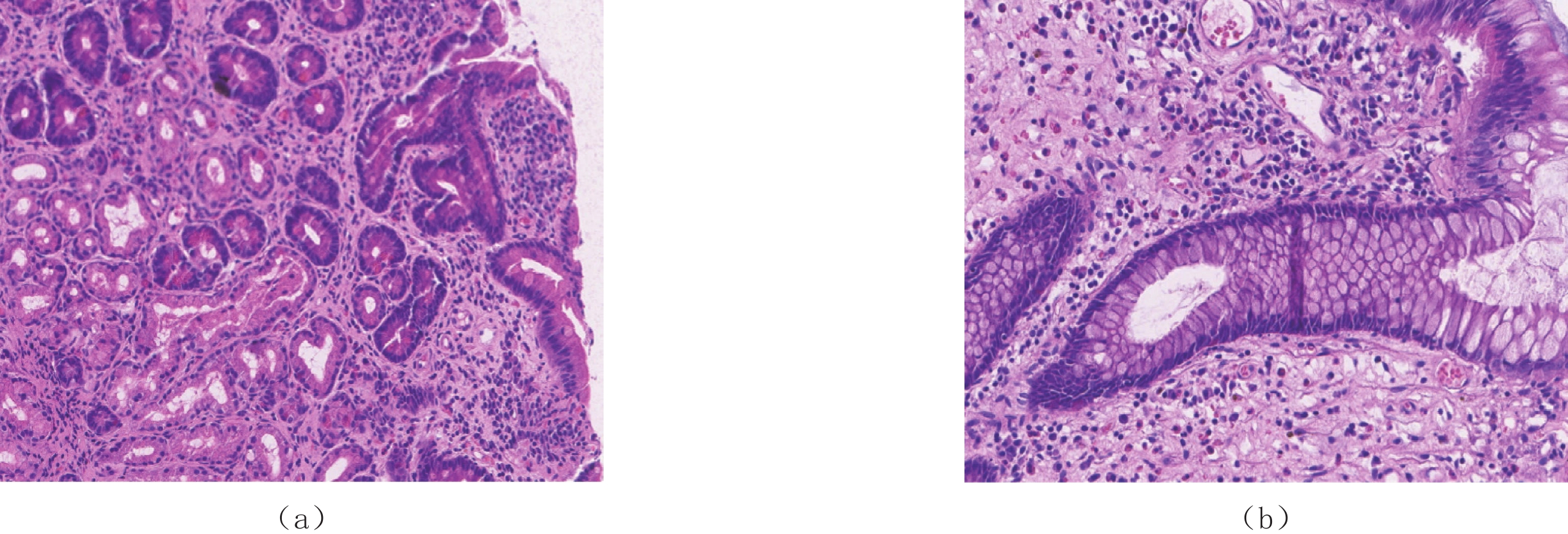
图 4 CCS患者治疗后随访CTE图像(a)~(d)为静脉期横断面增强图像,依次显示经过治疗后,胃体、十二指肠球降段、末端回肠、乙状结肠和直肠黏膜多发息肉样增生明显好转,息肉变稀疏甚至消失,部分结肠仍可见黏膜息肉样增生;(e)和(f)为冠状面重建图像,更加清晰显示整个病变范围。Figure 4. CTE images after treatment in patient with CCS![]() 图 5 CCS患者治疗后病理图像(a)和(b)分别为胃体和升结肠(HE 20×),显示腺上皮无明显异型性,间质一定量淋巴细胞、浆细胞和嗜酸性粒细胞浸润。Figure 5. Pathological images after treatment in patient with CCS
图 5 CCS患者治疗后病理图像(a)和(b)分别为胃体和升结肠(HE 20×),显示腺上皮无明显异型性,间质一定量淋巴细胞、浆细胞和嗜酸性粒细胞浸润。Figure 5. Pathological images after treatment in patient with CCS2. 讨论
CCS又称为息肉色素沉着-脱发-指甲营养不良综合征,是一种罕见的病因不明的非遗传性疾病。
2.1 病因及发病机制
CCS的病因及发病机制尚未明确,目前研究认为CCS的发生可能与自身免疫性疾病相关[5]。另外遗传易感因素与基因突变、幽门螺杆菌感染、精神压力、劳累、应激反应、微量元素缺乏等也可能是其诱发因素[3]。
2.2 临床特征
我国一项83例CCS统计分析显示,CCS的平均发病年龄为53.94岁(18~80岁),以男性居多,男︰女=2.61︰1,呈散发性,其中以北京在全国的占比最高,约为26.5%[5]。CCS临床主要表现为胃肠道多发性息肉、消化道症状和外胚层改变;CCS患者的实验室检查多呈非特异性改变,包括缺铁性贫血、低蛋白血症等,本例患者表现为贫血和低蛋白血症,与文献报道一致[6]。CCS常伴发自身免疫疾病如甲状腺功能减退症、重症急性胰腺炎、系统性红斑狼疮、类风湿性关节炎、硬皮病、白癜风和膜性肾病等,偶尔伴有骨髓增生异常综合征、骨巨细胞瘤、精神分裂症、肺栓塞甚至癌变倾向[7-9],外胚层异常改变可能与长期吸收功能障碍引发的营养不良相关[10-11]。本例患者经过近1年的治疗,达到临床缓解,内镜下取活检未发现癌变。
日本学者Goto[12]根据CCS的首发症状及发病过程,将其分为5型:Ⅰ型为腹泻型;Ⅱ型为味觉异常型;Ⅲ 型为口腔干燥型;Ⅳ 型为腹部不适型,表现为除腹泻以外的腹部症状,如慢性胃灼热感、非特异性腹痛等;Ⅴ型为毛发脱落型,表现为头发、胡须、眉毛、睫毛、腋毛及阴毛脱落,指(趾)甲萎缩。本病例表现为反复腹泻及指(趾)甲萎缩、脱落,结合文献报道,应为Ⅰ型和Ⅴ型混合表现。
2.3 CTE表现
CTE作为一种无创性检查手段,不仅可看到肠腔内的病变,而且还可以同时观察到肠腔外、肠壁和肠系膜的病变[13]。目前尚未有文献报道CCS的CTE表现,本文首次总结其表现:①息肉的发病部位除食道外,布满整个消化道;②息肉的大小不等,小者4 mm,大者可达到2 cm,小肠的病变以末端回肠息肉较大,大肠则以右半结肠为著;③息肉的形态呈圆形、椭圆形、指状,基底较宽,蒂并不明显;④息肉呈弥漫性均匀分布、地毯式覆盖整个消化道黏膜;⑤息肉与消化道黏膜分界不清,在胃及末端回肠形成巨大息肉样黏膜皱襞;⑥增强扫描明显强化,本例见末端回肠强化更明显,这可能与末端回肠淋巴滤泡增生有关;⑦未见明显肠系膜动脉分支与息肉相连;⑧肠套叠、癌变等并发症[5],本病例见末端回肠有套入右半结肠趋势,其他部位未见明显套叠改变;未见明显癌变征象;⑨肠腔外脂肪间隙清晰,未见肠系膜淋巴结增大。
2.4 内镜表现
CCS患者内镜下可见胃肠道弥漫性多发息肉,以结直肠和胃多见, 也可累及十二指肠和小肠,而在食管极为罕见[3]。本病例未见食管累及,与文献报道一致。息肉多为无蒂或亚蒂,形态不一,呈结节状、葡萄状或珊瑚样,直径多为2~5 cm,表面常充血水肿,可伴有糜烂或出血。息肉的病理类型以增生性息肉、腺瘤性息肉和错构瘤性息肉较为常见,主要的组织学表现为腺体囊性扩张伴间质水肿,部分囊腺充满蛋白样液体或浓缩黏液,伴有明显的炎性细胞浸润,通常以嗜酸性粒细胞、淋巴细胞和中性粒细胞浸润为主[13-14]。
该疾病虽然进展为胃肠道肿瘤较为罕见,但随着确诊患者逐渐增多,目前的研究也发现CCS同样存在并发胃肠道肿瘤的风险[9],本病例经治疗后病情好转,内镜下多部位活检并未发现癌变,但仍需定期随访。
2.5 治疗及转归
基于CCS疾病的罕见性及对其病因研究认识的缺乏性,目前关于CCS最佳的临床治疗方案仍处于探索阶段。目前常推荐的治疗方案是糖皮质激素、PPI及营养支持联合治疗, 其临床症状及息肉数目和大小几乎均于治疗1年内得以有效缓解[14]。
本病例经过接近1年的糖皮质激素治疗,病情得到明显缓解。本病预后差,目前研究认为CCS疾病5年死亡率高达55%,其中营养不良、低蛋白血症、反复感染、败血症、心力衰竭和胃肠道出血为本病常见的死亡原因[15]。因此在疾病的治疗进程中需要定期监测随访,包括电话随访及内镜随访等,以期降低CCS的死亡率。
2.6 诊断与鉴别诊断
CCS的诊断应依据病史、体格检查、内镜检查和病理组织学结果综合考虑。以胃肠道弥漫性息肉、指(趾)甲营养不良、脱发、皮肤色素沉着、腹泻、体重减轻和味觉障碍为表现的患者需要考虑本病。国内有学者提出:中老年起病、无遗传背景、临床表现、内镜表现和病理改变的诊断5要素[5]。本病例在内镜检查前先行CTE这一项无创性检查,高度怀疑CCS,提示其CT表现具有一定特征性,提示可将其作为一项诊断参考意见。
CCS常需与Menetrier病以及其他息肉综合征鉴别,例如幼年息肉病、Peutz-Jeghers综合征、Cowden综合征、Turcot综合征和家族性腺瘤性息肉病。
①Menetrier病又称巨大肥厚性胃炎,是一种罕见的胃黏膜腺体增生病,由于胃黏膜的过度增生而使胃壁广泛增厚。它是一种罕见的慢性病,最常累及胃体大弯侧及胃底部,少数累及胃窦部,多见于30~60岁的男性。②幼年性息肉是肠道错构瘤性息肉,是儿童最常见的息肉类型,以学龄前及学龄儿童多见,少数可见于青少年,息肉数目多、体积大,大小、数目不等,表现为有蒂或亚蒂的球形息肉,主要分布在直肠和远段结肠,少数见于小肠或胃。③Peutz-Jeghers综合征以儿童、青少年多发;典型表现为皮肤和黏膜特定部位出现色素斑,同时胃肠道多发性息肉,息肉可发生于全消化道,但以小肠居多,大小不等,多数小于1 cm,CTE表现为肠腔内圆形或分叶状软组织影,与黏膜分界清晰,宽基底或带蒂,重建图像可见肿块由肠系膜动脉直接供血,息肉所在肠段常因缺血而呈肠壁水肿表现,多发息肉常引起肠套叠,呈同心圆结构。④Cowden综合征又名多发性错构瘤综合征,是一种以胃肠道多发性息肉伴面部丘疹、口腔黏膜乳头状瘤以及肢端角化为特征的常染色体显性遗传性疾病,Cowden为患者家族之姓,而非通常的发现者或报道者;息肉可见于整个消化道,尤其是乙状结肠和直肠,大小数毫米到数厘米不等,本病需要临床综合分析,并参考基因检测和家族史。⑤Turcot综合征由加拿大外科医师Turcot最先报道,是一种肠道腺瘤病合并中枢神经系统恶性肿瘤为特征的常染色体显性遗传疾病,也称胶质瘤-息肉病综合征。息肉数量多数在100个以内,但多数直径在数厘米,常并发肠梗阻和恶变。⑥家族性腺瘤性息肉病为 APC基因种系突变导致的青少年时期发病,以结肠为主的常染色体显性遗传病。息肉在结肠内分布具有弥漫性密集状特征,大多数在1 cm以内,无蒂或半球状,并有远端结肠重,近端结肠轻的特点。
本文报道1例CCS的诊疗并进行文献复习,对患者的临床表现、实验室检查、CT小肠造影表现、内镜下表现及诊治过程进行阐述,目的在于对广大医师加深对该疾病的认识提供一定的帮助,尤其是其CT小肠造影表现,从而提高该疾病的诊断和治疗水平,减少误诊。
-
![]()
图 1 CCS患者脚趾和手指图像
显示指(趾)甲萎缩,甲板从甲床远端虫蚀样脱落,指间关节色素沉着。
Figure 1. Images of toes and fingers of the patient with CCS
![]()
图 2 CCS患者CTE图像
(a)~(d)为静脉期横断面增强图像,依次显示胃体、十二指肠球降段、末端回肠、乙状结肠和直肠黏膜多发息肉样增生,呈弥漫性分布,胃体和末端回肠呈现息肉样黏膜皱襞;(e)和(f)为冠状面重建图像,更加清晰显示息肉分布范围、形态,以末端回肠黏膜息肉样增生强化更明显(白箭)。
Figure 2. CT enterographic images of the patient with CCS
![]()
图 3 CCS患者胃镜和经肛双气囊小肠镜图像
(a)~(c)依次为胃体、末端回肠和升结肠,显示黏膜息肉样增生,表面腺体增生间裂,头端充血水肿。
Figure 3. Gastroscopic and transanal double balloon enteroscopic images of the patient with CCS
![]()
图 4 CCS患者治疗后随访CTE图像
(a)~(d)为静脉期横断面增强图像,依次显示经过治疗后,胃体、十二指肠球降段、末端回肠、乙状结肠和直肠黏膜多发息肉样增生明显好转,息肉变稀疏甚至消失,部分结肠仍可见黏膜息肉样增生;(e)和(f)为冠状面重建图像,更加清晰显示整个病变范围。
Figure 4. CTE images after treatment in patient with CCS
![]()
图 5 CCS患者治疗后病理图像
(a)和(b)分别为胃体和升结肠(HE 20×),显示腺上皮无明显异型性,间质一定量淋巴细胞、浆细胞和嗜酸性粒细胞浸润。
Figure 5. Pathological images after treatment in patient with CCS
表 1 CCS CTE表现
Table 1 CT enterographic features of CCS
息肉 CTE特点 部位 胃底、胃体、胃角、胃窦、十二指肠球降段、空肠、回肠下段、末端回肠、回盲部、大肠 大小 大小不等,小者4 mm,大者2 cm,小肠中以末端回肠为著,大肠中以右半结肠为著 形态 椭圆形、指状,基底宽,蒂不明显 分布 弥漫性分布、地毯式覆盖 边界(与黏膜分界) 与黏膜分界不清,形成巨大息肉样黏膜皱襞 供血动脉 未见明显肠系膜供血动脉与其相连 强化方式 明显强化,尤以末端回肠强化更明显 并发症 末端回肠有套入右半结肠趋势,其他部位未见明显套叠;未见明显癌变征象;其他脏器未
见异常肠管周围及肠系膜淋巴结 肠管周围脂肪间隙清晰,未见肠系膜淋巴结增大  下载: 导出CSV
下载: 导出CSV
表 2 CCS患者实验室检查结果前后对照
Table 2 Laboratory results of the patient with CCS before and after treatment
实验室检查项目 第一次入院 随访 血红蛋白/(g/L) 128 141 总蛋白/(g/L) 45 65 白蛋白/(g/L) 29 39
下载: 导出CSV
-
[1] CRONKHITE L W, CANADA W J. Generalized gastrointestinal polyposis; An unusual syndrome of polyposis, pigmentation, alopecia and onychotrophia[J]. New England Journal of Medicine, 1955, 252(4): 1011−10152.
[2] WATANABE C, KOMOTO S, TOMITA K, et al. Endoscopic and clinical evaluation of treatment and prognosis of Cronkhite-Canada syndrome: A Japanese nationwide survey[J]. Journal of gastroenterology, 2016, 51(4): 327−336. doi: 10.1007/s00535-015-1107-7
[3] 陈鑫, 李变霞, 朱兰平, 等. 罕见的息肉病-Cronkhite-Canada综合征[J]. 世界华人消化杂志, 2019,27(16): 977−983. [4] IQBAL U, CHAUDHARY A, KARIM M A, et al. Cronkhite-Canada syndrome: A rare cause of chronic diarrhea[J]. Gastroenterology Research, 2017, 10(3): 196−198. doi: 10.14740/gr820w
[5] 晁帅恒, 李修岭, 张梦婷, 等. Cronkhite-Canada综合征83例临床分析[J]. 中国临床研究, 2018,31(3): 397−399. doi: 10.13429/j.cnki.cjcr.2018.03.028 [6] SWEETSER S, AHLQUIST D A, OSBORN N K, et al. Clinicopathologic features and treatment outcomes in Cronkhite-Canada syndrome: Support for autoimmunity[J]. Digestive Diseases and Sciences, 2012, (2): 496−502.
[7] TAYLOR S A, KELLY J, LOOMES D E. Cronkhite-Canada syndrome: Sustained clinical response with Anti-TNF therapy[J]. Case Reports in Medicine, 2018: 9409732. DOI: 10.1155/2018/9409732.
[8] TRIANTAFILLIDIS J K, KOUGIOUMTZIAN A, LEIVADITOU A. et al. Cronkhite-Canada syndrome associated with a giant cell bone tumor[J]. Journal of Gastrointestinal and Liver Diseases, 2012, 21(4): 345.
[9] WANG J, ZHAO L, MA N, et al. Cronkhite-Canada syndrome associated with colon cancer metastatic to liver: A case report[J]. Medicine, 2017, 96(38): e7466. doi: 10.1097/MD.0000000000007466
[10] PIRACCINI B M, RECH G, SISTI A, et al. Twenty nail onychomadesis: An unusual finding in Cronkhite-Canada syndrome[J]. Journal of the American Academy of Dermatology, 2010, 63(1): 172−174. doi: 10.1016/j.jaad.2009.04.036
[11] YASUDA T, UEDA T, MATSUMOTO I, et al. Cronkhite-Canada syndrome presenting as recurrent severe acute pancreatitis[J]. Gastrointestinal Endoscopy, 2008, 67(3): 570−572. doi: 10.1016/j.gie.2007.07.041
[12] GOTO A. Cronkhite-Canada syndrome: Epidemiological study of 110 cases reported in Japan[J]. Nippon Geka Hokan. Archiv Für Japanische Chirurgie, 1995, 64(1): 3−14.
[13] CHRISTIAN M, ANDREAS S, VAVRICKA S R, et al. ECCO-ESGAR guideline for diagnostic assessment in IBD part 1: Initial diagnosis, monitoring of known IBD, detection of complications[J]. Journal of Crohn's and Colitis, 2019, 13(2): 144−164. doi: 10.1093/ecco-jcc/jjy113
[14] UEYAMA H, FU K, OGURA K, et al. Successful treatment for Cronkhite-Canada syndrome with endoscopic mucosal resection and salazosulfapyridine[J]. Techniques in Coloproctology, 2014, 18(5): 503−507. doi: 10.1007/s10151-012-0863-0
[15] SLAVIK T, MONTGOMERY E A. Cronkhite-Canada syndrome six decades on: The many faces of an enigmatic disease[J]. Journal of Clinical Pathology, 2014, 67(10): 891−897. doi: 10.1136/jclinpath-2014-202488

计量
- 文章访问数: 804
- HTML全文浏览量: 231
- PDF下载量: 123


