
Imaging Features of Patients with Coronavirus Disease 2019 with/without Underlying Diseases
-
摘要: 目的:探讨合并基础病和未合并基础病的新型冠状病毒感染(COVID-19)患者的影像学特征。材料与方法:回顾性收集首都医科大学附属北京世纪坛医院于2022年11月16日至2022年12月16确诊为COVID-19的患者153例。患者均自发病后1~14 d行胸部薄层CT平扫检查。根据或者有无基础病将其分为两组,其中合并基础病患者42例,未合并基础病患者111例,对比分析两组患者的差异。结果:两组患者在发病年龄、咳嗽、双肺分布、弥漫性分布、肺内蜂窝样改变、斑片状分布、大片状分布、束带样分布、铺路石征、空气支气管征、牵拉性支气管扩张及胸腔积液上差异有统计学意义。结论:COVID-19患者临床以发热和咳嗽症状最多见,胸部CT可见双肺多发病灶,病灶类型以支气管血管束增厚及GGO为著。合并基础病的患者在蜂窝样改变、铺路石征、空气支气管征、牵拉性支气管扩张及胸腔积液上较未合并基础病的患者更多。胸部薄层CT扫描对疾病的早期发现及诊断提供了关键的参考。Abstract: Objective: To explore the imaging characteristics of patients with novel coronavirus pneumonia (COVID-19) combined with different underlying diseases. Materials and methods: COVID-19 was diagnosed in 153 patients at Beijing Shijitan Hospital, Capital Medical University, from November 16, 2022 to December 16, 2022, and data were retrospectively collected. All patients underwent chest CT scan from 1 to 14 days after onset and were divided into two groups based on the presence or absence of underlying diseases. Forty-three patients had underlying diseases, and 110 patients had none. We compared the differences between the two groups. Result: The comparison between the two groups showed statistically significant differences in age, cough, bilateral lung distribution, diffuse distribution, honeycomb-like changes in the lungs, patchy distribution, large patchy distribution, band distribution, crazy-paving sign, air bronchogram sign, traction bronchiectasis, and pleural effusion. Conclusion: Fever and cough are the most common clinical symptoms in patients with COVID-19. Chest CT showed multiple lesions in both lungs. The most common types of lesions were thickening of bronchovascular bundle and GGO. Patients with underlying diseases had more honeycomb-like changes, crazy-paving sign, air bronchogram sign, traction bronchiectasis, and pleural effusion than those without underlying diseases. Chest thin-slice CT scan provides a key reference for the early detection and diagnosis of the disease.
-
Keywords:
- X-ray computer /
- tomography /
- COVID-19 /
- underlying disease
-
新型冠状病毒感染(COVID-19)是肺部特殊类型的病毒感染,以呼吸道飞沫及密切接触为主要传播途径,是一种致病性和感染性较高的传染性疾病[1-2]。COVID-19患者在影像学上的病变的累及范围、形态等变化多样,所以对其早期发现和诊断对疾病的治疗及预后十分关键。有文献报道合并基础病的COVID-19患者肺部症状和全身症状更重、更多,且住院率高出未合并基础病患者6倍,死亡率高出12倍[3-4]。我国COVID-19死亡病例中75% 以上合并有心血管疾病等1种以上的基础病[5]。
本研究纳入2022年11月16日至2022年12月16日于首都医科大学附属北京世纪坛医院确诊的153例COVID-19患者,其中合并基础病患者42例,未合并基础病患者111例,对比分析两组患者的差异,从而进一步了解探讨合并与未合并基础病患者的临床及影像特点。
1. 材料与方法
1.1 一般资料
回顾性收集首都医科大学附属北京世纪坛医院于2022年11月16日至2022年12月16日确诊为COVID-19的患者153例。诊断均符合中华人民共和国国家卫生健康委员会发布的《新型冠状病毒感染诊疗方案(试行第十版)》[6]。
153例患者中男性81例,女性72例,发病年龄26~95岁,临床症状包括发热67例、胸闷35例、咳嗽48例、肌肉酸痛1例、骨痛1例等。153例患者中,合并基础病患者42例(A组),未合并基础病者111例(B组)。42例患者中26例合并肺气肿、10例合并肺间质纤维化、9例患者合并冠心病、8例合并慢性支气管炎、7例合并肺结核、4例合并支气管扩张、1例合并肺占位。
1.2 影像检查方法
应用32排CT扫描仪(北京赛诺威盛Insitum-CT 338)对患者进行扫描。扫描参数:管电压120 kV,管电流150 mAs,螺距1.0,矩阵512×512,FOV 380~450。
扫描完成后对原始数据传入工作站进行MPR等后处理重建,重建层厚为肺窗1.5 mm和纵隔窗5 mm。肺窗的窗宽和窗位分别为1600和 -600,纵隔窗的窗宽和窗位分别为400和40。
1.3 图像分析
由初级或者中级影像诊断医师对患者就诊时的首次CT图像独立诊断,观察结果不一致时由高级医师评价。
观察指标包括:①病灶数量及累及部位:单发或多发,累及单叶、单肺、双肺;②病灶分布:胸膜下、胸膜内、弥漫性、血管束、对称分布、非叶段分布;③病变类型:磨玻璃影、实变、网格、蜂窝、血管束增厚、混合;④病变形态:结节、肿块、树芽、斑片(10~30 mm)、大片(>30 mm)、束带样、混合性;⑤病灶边缘:模糊、不规则、分叶、毛刺;⑥伴随征象:晕征、反晕征、铺路石征、空气支气管征、空气潴留征、马赛克征、牵拉性支气管扩张、胸腔积液。
1.4 统计学分析
采用SPSS 26.0统计学软件。符合正态分布的计量资料用(均数±标准差)表示,组间差异用方差分析,不符合正态分布的计量资料用中位数(四分位间距)表示,组间差异采用秩和检验。两组患者临床及影像之间的差异,如性别、症状、病变部位、肺内异常CT表现,采用卡方检验或Fisher精确检验。P<0.05为差异有统计学意义。
2. 结果
两组患者的一般资料中,A组发病年龄高于B组,差异有统计学意义,性别和病程无统计学差异(表1)。
表 1 是否合并基础病的COVID-19患者一般资料比较Table 1. Comparison of general data of COVID-19 patients with or without underlying diseases一般情况 组别 统计检验 A组(n=42)/例(%) B组(n=111)/例(%) $\chi^2$ P 性别 男性 25(59.5) 56(50.5) 1.007 0.316 女性 17(40.5) 55(49.5) 发病中位数年龄/岁(四分位间距) 83.0(11.0) 63.0(16.0) - <0.001 病程/d ≤7 29(69.0) 75(67.6) 0.031 0.861 >7 13(31.0) 36(32.4) 临床症状方面,B组患者的咳嗽多于A组患者,差异有统计学意义;发热、胸闷、肌肉酸痛和骨痛的差异无统计学意义(表2)。
表 2 是否合并基础病的COVID-19患者临床症状比较Table 2. Comparison of clinical symptoms of COVID-19 patients with or without underlying diseases临床症状 组别 统计检验 A组(n=42) B组(n=111) $\chi^2$ P 发热 16(38.1) 51(45.9) 0.763 0.382 胸闷 6(14.3) 29(26.1) 2.421 0.120 咳嗽 7(16.7) 41(36.9) 5.815 0.016 肌肉酸痛 0(0.0) 1(0.9) - 1.000 骨痛 0(0.0) 1(0.9) - 1.000 肺内病灶的分布情况上,A组患者的双肺分布和弥漫性分布均较B组患者多见,差异有统计学意义(表3)。
表 3 是否合并基础病的COVID-19患者肺内病灶分布情况对比Table 3. Comparison of lesion distribution of COVID-19 patients with or without underlying diseases分布情况 组别 统计检验 A组(n=42) B组(n=111) $\chi^2$ P 数量 单发 1(2.4) 5(4.5) 0.019 0.891 多发 41(97.6) 106(95.5) 0.019 0.891 累及部位 单叶 1(2.4) 16(14.4) 3.332 0.068 单肺 2(4.8) 6(5.4) 0.000 1.000 双肺 40(95.2) 88(79.3) 3.836 0.050 分布 胸膜下 32(76.2) 77(69.4) 0.692 0.405 胸膜内 39(92.9) 101(91.0) 0.002 0.964 弥漫性 35(83.3) 11(9.9) 78.125 <0.001 血管束 38(90.5) 90(81.1) 1.968 0.161 对称分布 26(61.9) 54(48.6) 2.146 0.143 非叶段分布 39(92.9) 90(81.1) 3.195 0.074 肺内异常征象方面,A组患者的肺内蜂窝样改变、斑片状分布、大片状分布、束带样分布、铺路石征、空气支气管征、牵拉性支气管扩张及胸腔积液均较B组患者多见,差异有统计学意义(表4,图1~图4)。
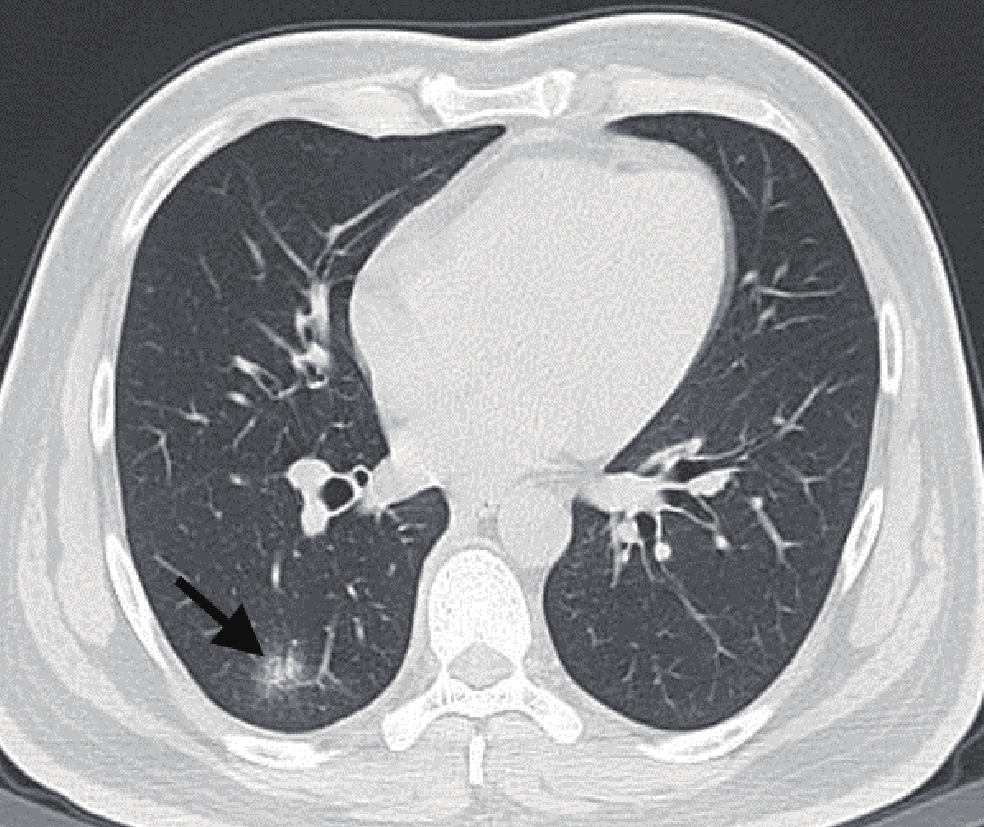
![]() 图 2 男性,70岁,合并基础病的COVID-19患者常规胸部CT平扫肺窗示左肺下叶背段“蜂窝样”改变(黑短箭),另双肺胸膜下见多发斑片状GGO(白星号)。Figure 2. Male, 70-year-old patient with COVID-19 with underlying diseases
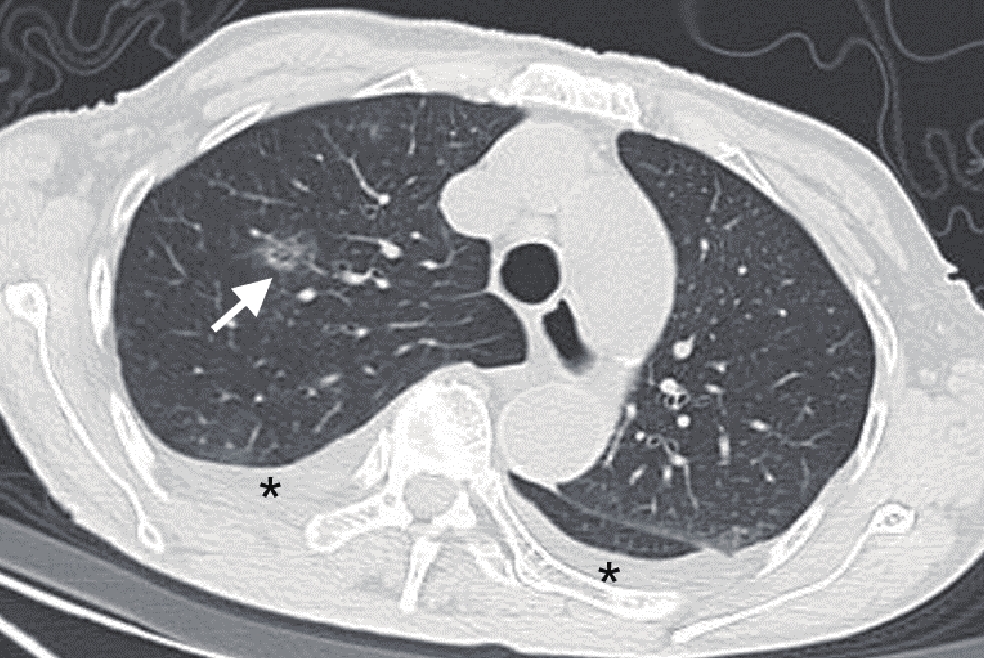
图 2 男性,70岁,合并基础病的COVID-19患者常规胸部CT平扫肺窗示左肺下叶背段“蜂窝样”改变(黑短箭),另双肺胸膜下见多发斑片状GGO(白星号)。Figure 2. Male, 70-year-old patient with COVID-19 with underlying diseases![]() 图 3 为同一患者,男性,79岁,合并基础病的COVID-19患者Figure 3. Male, 79-year-old patient with COVID-19 with underlying diseases表 4 是否合并基础病的COVID-19患者肺内异常征象比对Table 4. Comparison of abnormal pulmonary signs in COVID-19 patients with or without underlying diseases
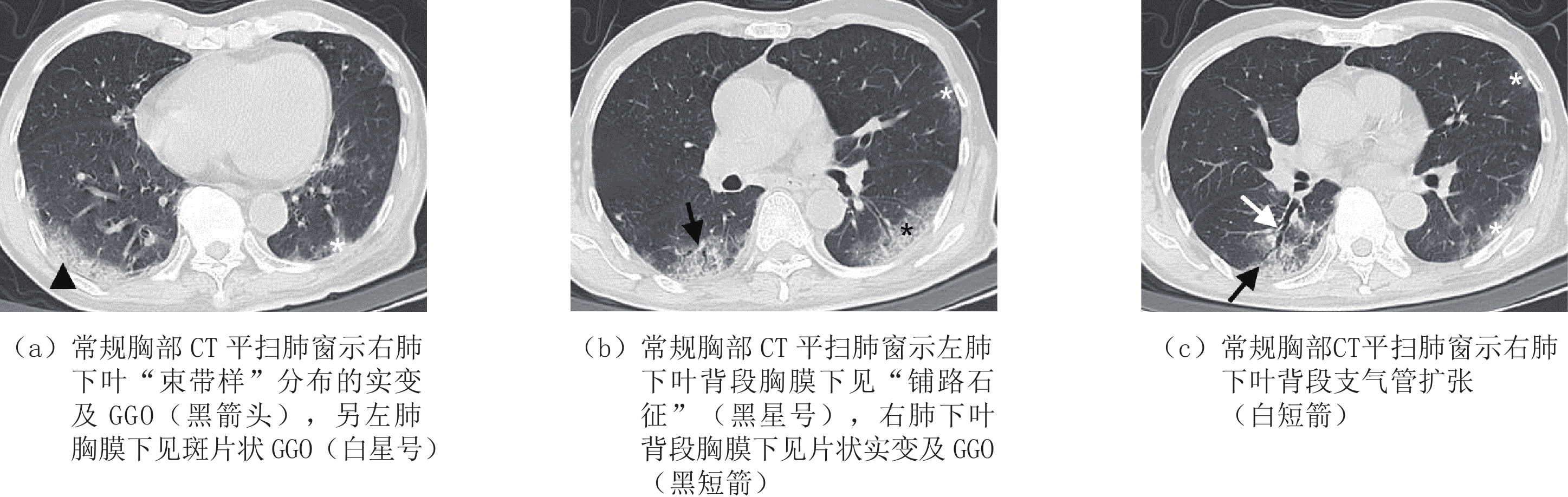
图 3 为同一患者,男性,79岁,合并基础病的COVID-19患者Figure 3. Male, 79-year-old patient with COVID-19 with underlying diseases表 4 是否合并基础病的COVID-19患者肺内异常征象比对Table 4. Comparison of abnormal pulmonary signs in COVID-19 patients with or without underlying diseases影像学征象 组别 统计检验 A组(n=42) B组(n=111) $\chi^2$ P 病变类型 GGO 41(97.6) 99(89.2) 1.806 0.179 实变 19(45.2) 50(45.0) 0.000 0.983 网格 37(88.1) 85(76.6) 2.502 0.114 蜂窝 7(16.7) 4(3.6) 5.958 0.015 血管束增厚 42(100.0) 102(91.9) 2.302 0.129 混合 41(97.6) 95(85.6) 3.332 0.068 病变形态 结节 31(73.8) 93(83.8) 1.973 0.160 肿块 1(2.4) 1(0.9) - 0.475 树芽 11(26.2) 42(37.8) 1.826 0.177 斑片 39(92.9) 88(79.3) 3.982 0.046 大片 32(76.2) 52(46.8) 10.597 0.001 束带样 24(57.1) 32(28.8) 10.527 0.001 混合 40(95.2) 93(83.8) 3.518 0.061 病灶边缘 模糊 19(45.2) 63(56.8) 1.626 0.202 不规则 18(42.9) 54(48.6) 0.410 0.522 分叶 1(2.4) 15(13.5) 2.932 0.087 毛刺 21(50.0) 46(41.4) 0.907 0.341 伴随征象 晕征 31(73.8) 80(72.1) 0.046 0.830 反晕征 17(40.5) 38(34.2) 0.516 0.473 铺路石征 34(81.0) 54(48.6) 13.013 0.000 空气支气管征 37(88.1) 72(64.9) 8.026 0.005 空气潴留征 15(35.7) 34(30.6) 0.362 0.548 马赛克征 24(57.1) 44(39.6) 3.781 0.052 牵拉性支气管扩张 29(69.0) 54(48.6) 5.109 0.024 胸腔积液 4(9.5) 1(0.9) - 0.022 ![]() 图 1 男性,41岁,未合并基础病的COVID-19患者常规胸部CT平扫肺窗示右肺下叶背段斑片状GGO(黑短箭)。Figure 1. Male, 39-year-old patient with COVID-19 without underlying diseases
图 1 男性,41岁,未合并基础病的COVID-19患者常规胸部CT平扫肺窗示右肺下叶背段斑片状GGO(黑短箭)。Figure 1. Male, 39-year-old patient with COVID-19 without underlying diseases3. 讨论
SARS-CoV-2是一种有包膜的单链RNA冠状病毒,可感染多种脊椎动物,容易在人与人之间传播[7]。COVID-19患者的肺部病理表现为弥漫性肺泡损伤,并有单核细胞和巨噬细胞浸润气腔,肺泡壁弥漫性增厚形成透明膜[8-9]。
本研究两组患者的性别差异统计学无意义,A组患者的发病年龄为83.0(11.0)岁,B组患者发病年龄为63.0(16.0)岁,两者差异有统计学意义,与文献报道一致[10]。本研究的COVID-19患者最常见的临床表现是发热和咳嗽,与文献报道一致[11],但B组患者的出现咳嗽较A组患者多,与文献不一致。国家卫生健康委员会发布的新型冠状病毒感染诊疗方案(试行第十版)指出,COVID-19的诊断根据流行病学史、临床表现、实验室检查等综合分析作出诊断。新冠病毒核酸检测阳性为确诊的首要标准,但有文献报道核酸检测的灵敏度仅60%[12],因此胸部CT对于疾病的诊断也存在价值[13]。本研究发现A组患者的影像表现较B组患者更重。
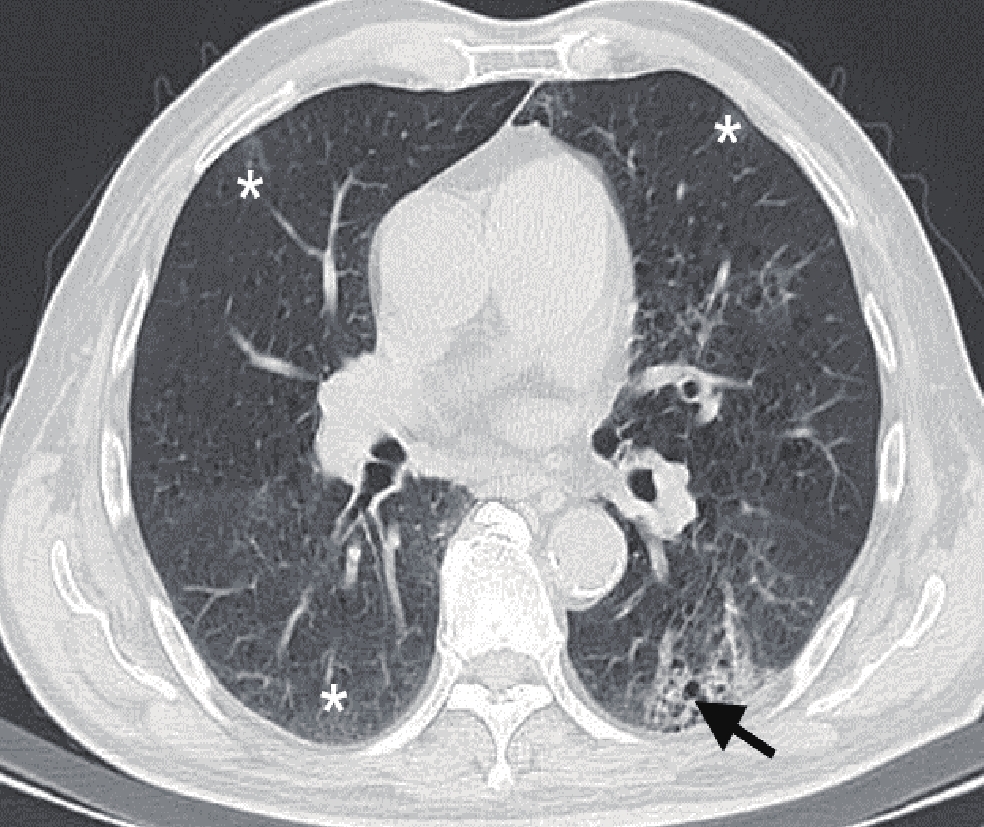
![]() 图 4 女性,87岁,合并基础病的COVID-19患者常规胸部CT平扫肺窗示双侧胸腔见弧形液性密度(黑星号),右肺上叶前段见斑片状GGO(白短箭)。Figure 4. Female, 87-year-old patient with COVID-19 with underlying diseases
图 4 女性,87岁,合并基础病的COVID-19患者常规胸部CT平扫肺窗示双侧胸腔见弧形液性密度(黑星号),右肺上叶前段见斑片状GGO(白短箭)。Figure 4. Female, 87-year-old patient with COVID-19 with underlying diseases本研究153例患者95% 以上的病灶均以多发为主,且病变累及广泛,均以双肺受累最多见,A组患者较B组更多见,差异有统计学意义。但文献报道COVID-19患者病变初期以单肺分布为主,随着疾病进展演变为双侧分布[7,14],病变的单肺或双肺分布是否与合并基础病相关未见文献报道,我们猜测合并基础病患者的免疫力低,炎症反应更重,可能会加速疾病的进程,因此A组双肺分布较B组多。此外,B组患者病灶以胸膜下分布最多,与A组差异无统计学意义,与文献报道一致[15-17]。A组患者病灶的优势分布以弥漫性分布为主,病变范围较B组患者更广泛,差异有统计学意义,与文献报道一致[18]。
本研究两组患者均以血管束增粗、磨玻璃影(ground glass opacity,GGO)为最多及次多见的病变类型,差异均无统计学意义。前者考虑是血管周围间质水肿所致,并不是血管内径的增粗[19],后者因肺泡腔内渗出物是否完全填充、肺泡间隔充血程度及小叶间隔水肿程度的不同表现为纯GGO或混杂GGO,部分患者合并小叶间隔增厚或小叶内间质增厚而表现为“铺路石征”,是COVID-19疾病早期最多见及典型的征象,与文献报道一致[20]。
两组患者的蜂窝样改变及牵拉性支气管扩张均以A组患者较多见,差异有统计学意义。A组患者合并基础病,易引起小气道的损伤,可能导致肺内蜂窝样改变及牵拉性支气管扩张。此外,COVID-19患者的病变形态多样,例如结节、肿块、树芽、片状、束带样及混合改变,与文献报道一致[21-22]。
此外,合并基础病与未合并基础病的COVID-19患者还在空气支气管征、胸腔积液上的差异有统计学意义,以上征象均为A组更多见。空气支气管征和胸腔积液均为COVID-19疾病进展时出现的征象,前者可因小气道疾病引起气体潴留所致,由于A组合并基础病,小气道更易受损,因此较B组多见。当疾病进展,炎性改变累及胸膜时,胸腔积液才会出现,与文献报道一致[18,23]。
综上所述,COVID-19患者临床以发热和咳嗽症状最多见,胸部CT可见双肺多发病灶,病灶类型以支气管血管束增厚及GGO为著。合并基础病的患者在蜂窝样改变、铺路石征、空气支气管征、牵拉性支气管扩张及胸腔积液上较未合并基础病的患者更多。胸部CT对疾病的早期发现及诊断提供了关键的参考。
本研究的局限性:①未对 2组患者的实验室指标、血氧饱和度及预后进行对比研究;②合并基础病患者的样本量较小,今后将纳入更多相关病例进行研究。
-
![]()
图 2 男性,70岁,合并基础病的COVID-19患者
常规胸部CT平扫肺窗示左肺下叶背段“蜂窝样”改变(黑短箭),另双肺胸膜下见多发斑片状GGO(白星号)。
Figure 2. Male, 70-year-old patient with COVID-19 with underlying diseases
![]()
图 3 为同一患者,男性,79岁,合并基础病的COVID-19患者
Figure 3. Male, 79-year-old patient with COVID-19 with underlying diseases
![]()
图 1 男性,41岁,未合并基础病的COVID-19患者
常规胸部CT平扫肺窗示右肺下叶背段斑片状GGO(黑短箭)。
Figure 1. Male, 39-year-old patient with COVID-19 without underlying diseases
![]()
图 4 女性,87岁,合并基础病的COVID-19患者
常规胸部CT平扫肺窗示双侧胸腔见弧形液性密度(黑星号),右肺上叶前段见斑片状GGO(白短箭)。
Figure 4. Female, 87-year-old patient with COVID-19 with underlying diseases
表 1 是否合并基础病的COVID-19患者一般资料比较
Table 1 Comparison of general data of COVID-19 patients with or without underlying diseases
一般情况 组别 统计检验 A组(n=42)/例(%) B组(n=111)/例(%) $\chi^2$ P 性别 男性 25(59.5) 56(50.5) 1.007 0.316 女性 17(40.5) 55(49.5) 发病中位数年龄/岁(四分位间距) 83.0(11.0) 63.0(16.0) - <0.001 病程/d ≤7 29(69.0) 75(67.6) 0.031 0.861 >7 13(31.0) 36(32.4)  下载: 导出CSV
下载: 导出CSV
表 2 是否合并基础病的COVID-19患者临床症状比较
Table 2 Comparison of clinical symptoms of COVID-19 patients with or without underlying diseases
临床症状 组别 统计检验 A组(n=42) B组(n=111) $\chi^2$ P 发热 16(38.1) 51(45.9) 0.763 0.382 胸闷 6(14.3) 29(26.1) 2.421 0.120 咳嗽 7(16.7) 41(36.9) 5.815 0.016 肌肉酸痛 0(0.0) 1(0.9) - 1.000 骨痛 0(0.0) 1(0.9) - 1.000
下载: 导出CSV
表 3 是否合并基础病的COVID-19患者肺内病灶分布情况对比
Table 3 Comparison of lesion distribution of COVID-19 patients with or without underlying diseases
分布情况 组别 统计检验 A组(n=42) B组(n=111) $\chi^2$ P 数量 单发 1(2.4) 5(4.5) 0.019 0.891 多发 41(97.6) 106(95.5) 0.019 0.891 累及部位 单叶 1(2.4) 16(14.4) 3.332 0.068 单肺 2(4.8) 6(5.4) 0.000 1.000 双肺 40(95.2) 88(79.3) 3.836 0.050 分布 胸膜下 32(76.2) 77(69.4) 0.692 0.405 胸膜内 39(92.9) 101(91.0) 0.002 0.964 弥漫性 35(83.3) 11(9.9) 78.125 <0.001 血管束 38(90.5) 90(81.1) 1.968 0.161 对称分布 26(61.9) 54(48.6) 2.146 0.143 非叶段分布 39(92.9) 90(81.1) 3.195 0.074
下载: 导出CSV
表 4 是否合并基础病的COVID-19患者肺内异常征象比对
Table 4 Comparison of abnormal pulmonary signs in COVID-19 patients with or without underlying diseases
影像学征象 组别 统计检验 A组(n=42) B组(n=111) $\chi^2$ P 病变类型 GGO 41(97.6) 99(89.2) 1.806 0.179 实变 19(45.2) 50(45.0) 0.000 0.983 网格 37(88.1) 85(76.6) 2.502 0.114 蜂窝 7(16.7) 4(3.6) 5.958 0.015 血管束增厚 42(100.0) 102(91.9) 2.302 0.129 混合 41(97.6) 95(85.6) 3.332 0.068 病变形态 结节 31(73.8) 93(83.8) 1.973 0.160 肿块 1(2.4) 1(0.9) - 0.475 树芽 11(26.2) 42(37.8) 1.826 0.177 斑片 39(92.9) 88(79.3) 3.982 0.046 大片 32(76.2) 52(46.8) 10.597 0.001 束带样 24(57.1) 32(28.8) 10.527 0.001 混合 40(95.2) 93(83.8) 3.518 0.061 病灶边缘 模糊 19(45.2) 63(56.8) 1.626 0.202 不规则 18(42.9) 54(48.6) 0.410 0.522 分叶 1(2.4) 15(13.5) 2.932 0.087 毛刺 21(50.0) 46(41.4) 0.907 0.341 伴随征象 晕征 31(73.8) 80(72.1) 0.046 0.830 反晕征 17(40.5) 38(34.2) 0.516 0.473 铺路石征 34(81.0) 54(48.6) 13.013 0.000 空气支气管征 37(88.1) 72(64.9) 8.026 0.005 空气潴留征 15(35.7) 34(30.6) 0.362 0.548 马赛克征 24(57.1) 44(39.6) 3.781 0.052 牵拉性支气管扩张 29(69.0) 54(48.6) 5.109 0.024 胸腔积液 4(9.5) 1(0.9) - 0.022
下载: 导出CSV
-
[1] XIE J, WANG Q, XU Y, et al. Clinical characteristics, laboratory abnormalities and CT findings of COVID-19 patients and risk factors of severe disease: A systematic review and meta-analysis[J]. Annals of Palliative Medicine, 2021, 10(2): 1928−1949. doi: 10.21037/apm-20-1863
[2] TANG Y, LIAO H, WU Q, et al. Chest CT imaging characteristics and their evolution of 48 patients with COVID-19 in Hengyang, China[J]. American Journal of Translational Research, 2021, 13(9): 9983−9992.
[3] CHAN J F W, YUAN S, KOK K H, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to- person transmission: A study of a family cluster[J]. Lancet, 2020, 395(10223): 514−523. doi: 10.1016/S0140-6736(20)30154-9
[4] STOKES E K, ZAMBRANO L D, ANDERSON K N, et al. Coronavirus disease 2019 case Surveillance-United States, January 22-May 30, 2020[J]. Morbidity and Mortality Weekly Report, 2020, 69(24): 759−765. doi: 10.15585/mmwr.mm6924e2
[5] 中华人民共和国国家卫生健康委员会. 国家卫生健康委员会新闻发布会[EB/OL]. [2020-02-04]. http://news. cctv.com/zhibo/tuwen2016/gjwjw/index.shtml. [6] 中华人民共和国国家卫生健康委员会, 新型冠状病毒感染诊疗方案(试行第十版)[EB/OL]. [2023-01-05]. http://www.gov.cn/zhengce/zhengceku/2023-01/06/5735343/files/5844ce04246b431dbd322d8ba10afb48.pdf. [7] ASSELAH T, DURANTEL D, PASMANT E, et al. COVID-19: Discovery, diagnostics and drug development[J]. Journal of Hepatology, 2021, 74(1): 168−184. doi: 10.1016/j.jhep.2020.09.031
[8] XU Z, SHI L, WANG Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome[J]. The Lancet Respiratory Medicine, 2020, 8(4): 420−422. doi: 10.1016/S2213-2600(20)30076-X
[9] ZHU N, ZHANG D, WANG W, et al. A novel coronavirus from patients with pneumonia in China, 2019[J]. The New England Journal of Medicine, 2020, 382(8): 727−733. doi: 10.1056/NEJMoa2001017
[10] 仕丽, 丁欢, 王檀, 等. 134例合并不同基础疾病新型冠状病毒肺炎患者转重率分析[J]. 吉林中医药, 2021,41(11): 1458−1461. doi: 10.13463/j.cnki.jlzyy.2021.11.016 SHI L, DING H, WNAG T, et al. An analysis on the aggravation rate of the 134 COVID-19 patients combined with different underlying diseases[J]. Jilin Journal of Traditional Chinese Medicine, 2021, 41(11): 1458−1461. (in Chinese). doi: 10.13463/j.cnki.jlzyy.2021.11.016
[11] HUANG C, WANG Y, LI X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China[J]. Lancet, 2020, 395(10223): 497−506.
[12] KANNE J P, LITTLE B P, CHUNG J H, et al. Essentials for radiologists on COVID-19: An update-radiology scientific expert panel[J]. Radiology, 2020, 296(2): E113−E114. doi: 10.1148/radiol.2020200527
[13] 黄璐, 韩瑞, 于朋鑫, 等. 新型冠状病毒肺炎不同临床分型间CT和临床表现的相关性研究[J]. 中华放射学杂志, 2020,54(4): 300−304. doi: 10.3760/cma.j.cn112149-20200205-00087 HUANG L, HAN R, YU P X, et al. A correlation study of CT and clinical features of different clinical types of COVID-19[J]. Chinese Journal of Radiology, 2020, 54(4): 300−304. (in Chinese). doi: 10.3760/cma.j.cn112149-20200205-00087
[14] SHI H, HAN X, JIANG N, et al. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study[J]. The Lancet Infectious Disease, 2020, 20(4): 425−434. doi: 10.1016/S1473-3099(20)30086-4
[15] HU Q, GUAN H, SUN Z, et al. Early CT features and temporal lung changes in COVID-19 pneumonia in Wuhan, China[J]. European Journal of Radiology, 2020, 128: 109017. doi: 10.1016/j.ejrad.2020.109017
[16] ZHAO W, ZHONG Z, XIE X, et al. Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study[J]. American Journal of Roentgenology, 2020, 214(5): 1072−1077. doi: 10.2214/AJR.20.22976
[17] ZHOU S, ZHU T, WANG Y, et al. Imaging features and evolution on CT in 100 COVID-19 pneumonia patients in Wuhan, China[J]. European Radiology, 2020, 30(10): 5446−5454. doi: 10.1007/s00330-020-06879-6
[18] 李运江, 叶云峰, 宣伟玲, 等. 有无基础疾病的新型冠状病毒肺炎患者首次胸部高分辨率CT表现比较[J]. 浙江医学, 2021,43(14): 1575−1578, 1585. doi: 10.12056/j.issn.1006-2785.2021.43.14.2020-4418 [19] 史河水, 韩小雨, 樊艳青, 等. 新型冠状病毒(2019-nCoV)感染的肺炎临床特征及影像学表现[J]. 临床放射学杂志, 2020,39(1): 8−11. doi: 10.13437/j.cnki.jcr.20200206.002 SHI H S, HAN X Y, FAN Y Q, et al. Radiologic features of patients with 2019-nCoV infection[J]. Journal of Clinical Radiology, 2020, 39(1): 8−11. (in Chinese). doi: 10.13437/j.cnki.jcr.20200206.002
[20] MACHNICKI S, PATEL D, SINGH A, et al. The usefulness of chest CT imaging in patients with suspected or diagnosed COVID-19: A review of literature[J]. Chest, 2021, 160(2): 652−670.
[21] PAREKH M, DONURU A, BALASUBRAMANYA R, et al. Review of the chest CT differential diagnosis of ground-glass opacities in the COVID era[J]. Radiology, 2020, 297(3): E289−E302. doi: 10.1148/radiol.2020202504
[22] 孙莹, 李玲, 刘晓燕, 等. 早期新型冠状病毒肺炎的胸部薄层平扫CT表现特征[J]. CT理论与应用研究, 2023,32(1): 131−138. DOI: 10.15953/j.ctta.2023.006. SUN Y, LI L, LIU X Y, et al. Imaging features of early COVID-19 on chest thin-slice non-enhanced CT[J]. CT Theory and Applications, 2023, 32(1): 131−138. DOI: 10.15953/j.ctta.2023.006. (in Chinese).
[23] KOO H J, LIM S, CHOE J, et al. Radiographic and CT features of viral pneumonia[J]. Radiographics, 2018, 38(3): 719−739. doi: 10.1148/rg.2018170048
计量
- 文章访问数: 165
- HTML全文浏览量: 52
- PDF下载量: 13


