
Analysis of Prognosis of Coronavirus Disease 2019 Using Quantitative Measurement of Deep Learning
-
摘要: 目的:分析基于深度学习定量测量新型冠状病毒感染(COVID-19)患者胸部CT炎性病灶的特征,预警重症的发生,提高对COVID-19预后的认识。方法:回顾性分析477例首次确诊为中型COVID-19患者的胸部CT,男276例,女201例,根据是否转为重症(重型/危重型)分为A组(未转为重症)、B组(转为重症),比较两组病例病灶分布、累及肺叶侧别、数目等CT基本征象及基于深度学习的病灶体积、体积占比和密度等的差异。结果:477例COVID-19患者均有流行病学史,年龄、性别在两组间的差异无统计学意义。B组全肺及各肺叶病灶体积及体积占比高于A组。A组病灶以右肺下叶为主,占比高于其它肺叶,达3.32%;其次为左肺下叶,占比为2.08%;左肺上叶病灶体积占比较其他肺叶低,仅为0.25%。A组部分患者右肺上叶、右肺中叶及左肺上叶无病灶。B组病灶呈双肺分布,各肺叶均有;其中以右肺下叶、左肺下叶分布为主,占比最高,分别为57.86% 和54.76%;右肺中叶体积占比较其他肺叶低,为34.73%。各组病灶均以磨玻璃密度影为主。A组以密度为 -570~-470 HU病灶为主,占比达13.89%;其次为 -470~-370 HU,占比为11.07%;密度为30~70 HU实性病灶及密度为 -70~30 HU较少,占比仅3.22% 和4.75%。B组大部分呈磨玻璃密度影,以病灶密度为 -570~-470 HU、-470~-370 HU与 -370~-270 HU为主,占比分别为13.18%、12.58%、12.52%;密度为 -570~-470 HU的病灶占比与A组差异无统计学意义,余各密度病灶体积及体积占比高于A组,呈病灶密度越高,B组占比较A组越高的趋势。结论:感染病灶体积较大、实性成分较多及多种CT征象并存常提示肺部炎症较重,容易进展为重症,基于深度学习的胸部CT定量测量有助于评估COVID-19预后及预警重症。Abstract: Objective: To analyze the differences of chest computed tomography (CT) inflammatory lesions in patients with coronavirus disease 2019 (COVID-19), which were quantitatively measured based on deep learning, to warn the occurrence of severe cases and improve the understanding of the prognosis of COVID-19. Methods: The chest CT scans of 477 local patients with COVID-19 diagnosed for the first time at Inner Mongolia Autonomous Region People's Hospital were retrospectively analyzed. A total of 276 men and 201 women were divided into group A (not serious) and group B (serious) based on whether their diseases turned serious (severe/critical). Comparison was made between the two groups on the basic CT signs, such as lesion distribution, involved lobe side, number, differences in lesion volume, volume proportion, and density based on deep learning. Results: All 477 patients with COVID-19 had epidemiological history, and no statistical difference was noted in age and gender between the two groups. The volume and proportion of the lesions in the whole lung and each lobe of the lung in group B were higher than those in group A. The lesions in group A were mainly in the lower lobe of the right lung, accounting for 3.32% more than that in other lobes. The lower lobe of the left lung was the next, accounting for 2.08%. The volume of lesions in the upper lobe of the left lung was lower than that in other lobes, accounting for only 0.25%. No lesions were noted in the upper lobe of the right lung, middle lobe of the right lung, and upper lobe of the left lung in part of group A. In group B, the lesions were distributed in both lungs and in each lung lobe. The lower lobes of the right lung and left lung were predominant, accounting for 57.86% and 54.76%, respectively. The volume of the middle lobe of the right lung was 34.73% compared with the other lobes. The main lesions in each group were ground-glass density shadows, and the main lesions in group A were −570 ~ −470 HU density, accounting for 13.89%, followed by −470 ~ −370 HU, accounting for 11.07%. Only 3.22% and 4.75% of solid lesions with densities of 30 ~ 70 HU and −70 ~ 30 HU were found. Most of the lesions in group B were ground-glass density shadows, and the focal densities were mainly −570 ~ −470 HU, −470 ~ −370 HU, and −370 ~ −270 HU, accounting for 13.18%, 12.58%, and 12.52%, respectively. No statistical difference was noted between the proportion of lesions with a density of −570 ~ −470 HU and that of group A; however, the volume and proportion of other lesions with different densities were higher than those of group A, showing a trend that the higher the density of the lesions, the higher the proportion of group B was compared with group A. Conclusion: Larger infection volume, more lesion solid components, and multiple CT signs often indicate more severe lung inflammation, which easily progresses to severe disease. Quantitative measurement of chest CT based on deep learning is helpful for the prognosis assessment of COVID-19 and the early warning of severe outcome.
-
Keywords:
- deep learning /
- tomography /
- X-ray computed /
- coronavirus disease 2019
-
新型冠状病毒感染(coronavirus disease 2019,COVID-19)疫情自2019年底开始的在世界各国频发,成为全球性的重大公共卫生事件。随着我国防控政策的科学调整[1],“保健康、防重症”成为现阶段常态化防控的工作重心。医生在诊断过程中面临着门诊患者流行病学史越来越模糊的局面。COVID-19的诊断主要依赖核酸检测与CT;相比核酸检测用时较长且存在假阴性等缺点,胸部CT具有实时性高、敏感性好、不易漏诊等优势,特别胸部薄层平扫CT可在COVID-19的早期发现病灶、精准诊断和鉴别、评判临床分期和疗效预后等方面提供重要影像依据[2-3]。既往胸部CT分析主要依靠诊断医生肉眼主观视觉评估,缺乏客观依据。近年来深度学习定量分析软件不断优化,为客观评估病灶性质提供了新的途径,其能够准确分割病灶并计算病灶体积、密度以及病灶非实性占比等多种参数。
本研究回顾性分析就诊的COVID-19患者的胸部CT资料,通过深度学习肺炎定量工具客观地对肺内病变进行多参数定量分析,探讨病变演变规律,为预后判断提供客观依据。
1. 资料与方法
1.1 病例资料
参照国家卫生健康委员会《新型冠状病毒感染诊疗方案(试行第十版)》[4]胸部影像学部分,回顾性分析内蒙古自治区人民医院2022年12月1日至2022年12月31日感染奥密克戎(Omicron)BF.7的477例COVID-19患者,男性276例(57.9%),女性201例(42.1%),均有流行病学史,初诊时发热466例,咳嗽114例。根据是否转为重症(重型/危重型)分为A组(未转为重症)、B组(转为重症)。
纳入标准:临床资料完善;首诊为COVID-19临床分型中型且影像资料完整、图像无伪影病例。排除标准:首诊为临床分型轻型、重型、危重型COVID-19本土病例及图像伪影重,AI无法识别者;无薄层图像者。
1.2 影像检查方法
使用GE LightSpeed VCT 64排CT机。扫描参数:管电压120 kV,管电流自动毫安输出,正常体型设置为60~80 mAs,层厚5.00 mm,重建层厚1.25 mm,层间距1 mm,矩阵512×512。所有患者均采取仰卧位,深吸气后屏气状态下由肺尖至肺底扫描。
1.3 CT图像分析及模型检测
将胸部CT图像导入AI肺炎辅助诊断系统(北京推想科技有限公司,Inferead CT Pneumonia)进行处理,该系统利用迁移学习技术及标记好的COVID-19数据进行训练,然后自动划分肺叶,通过深度学习分割模型对肺病灶区域进行勾画并测量肺炎病灶的密度、体积及肺炎病灶的体积占肺叶及整肺体积的百分比。
1.4 资料分析
由影像医学科胸组两位具有丰富工作经验的副主任医师双盲独立阅片,对胸部CT图像病灶分布、形态、组成、胸腔积液及纵隔淋巴结情况及对基于人工智能标注的结果进行校对、修正、补充。意见不一致时由第3位胸组主任医师加入协商,达成一致。
1.5 统计学方法
统计学分析采用SPSS 22.0软件。经正态性检验,数据不服从正态分布,采用中位数(四分位间距描述);A组(未转为重症)与B组(转为重症)两组比较时采用非参数Kruskal-Wallis检验及Mann-Whitney U检验;检验水准α=0.05,以P≤0.05为差异具有统计学意义。
2. 结果
2.1 患者分组情况
A组患者450人,男女比(260/190),B组患者27人,男女比(16/11),两组患者性别比例差异无统计学意义;A组患者平均年龄(68.4±14.5)岁,B组患者平均年龄(72.7±13.0)岁,两组患者年龄差异无统计学意义;A组和B组患者胸部CT图像进行AI深度学习定量分析。
2.2 病灶体积、密度及占比特点
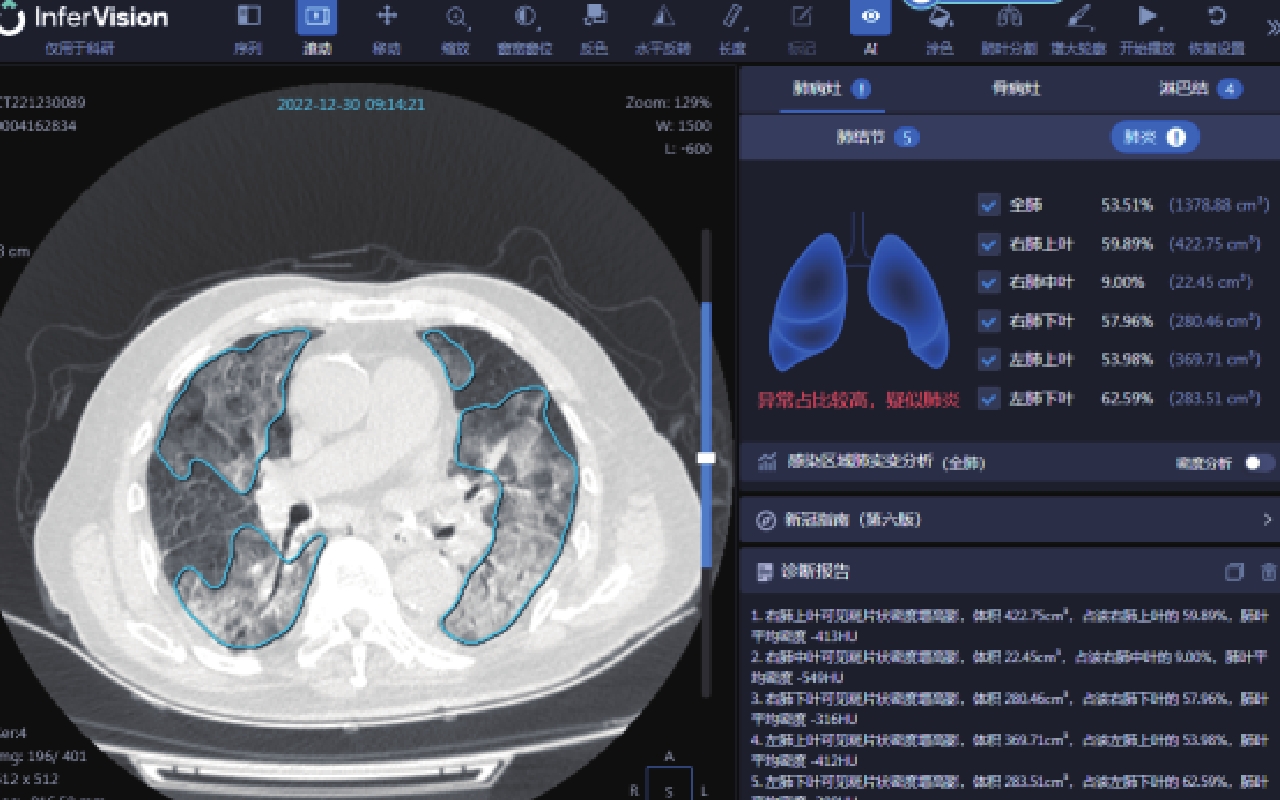
本研究应用北京推想科技有限公司的AI肺炎辅助诊断系统对两组新型冠状病毒奥密克戎变异株感染患者胸部CT的炎症病灶进行勾画,并计算全肺及各肺叶炎症病灶体积及占比(图1)。
![]() 图 1 推想人工智能评估新型冠状病毒奥密克戎变异株感染患者肺内病灶体积示意图患者,男,86岁,确诊为新型冠状病毒奥密克戎变异株感染。Figure 1. Schematic diagram of InferVision artificial Intelligence evaluating the volume of lesions in the lung of patients infected with the COVID-19 omicron variant
图 1 推想人工智能评估新型冠状病毒奥密克戎变异株感染患者肺内病灶体积示意图患者,男,86岁,确诊为新型冠状病毒奥密克戎变异株感染。Figure 1. Schematic diagram of InferVision artificial Intelligence evaluating the volume of lesions in the lung of patients infected with the COVID-19 omicron variantB组全肺及各肺叶(右肺上叶、中叶、下叶及左肺上叶、下叶)病灶体积及体积占比高于A组。A组病灶以右肺下叶为主,占比较其它肺叶高,达3.32%;其次为左肺下叶,占比为2.08%;左肺上叶病灶体积占比较其他肺叶低,仅为0.25%。A组部分患者右肺上叶、右肺中叶及左肺上叶无病灶。B组病灶呈双肺分布,各肺叶均有分布;其中以右肺下叶、左肺下叶分布为主,占比最高,分别为57.86% 和54.76%;右肺中叶体积占比较其他肺叶低,为34.73%(表1)。
表 1 A组和B组全肺及各肺叶病灶体积及体积占比Table 1. The lesion volume and proportion of the whole lung and each lung lobe in groups A and B指标 组别 统计检验 A组(n=450) B组(n=27) Z P 全肺病灶体积占比/% 2.43(0.45~7.43) 40.45(33.47~46.60) 75.868 <0.001 全肺病灶体积 87.12(17.73~262.20) 1239.21(841.54~1395.12) 72.842 <0.001 右肺上叶病灶体积占比/% 0.50(0~3.00) 35.70(20.84~50.32) 69.027 <0.001 右肺上叶病灶体积 4.56(0~24.22) 225.10(120.17~317.48) 64.978 <0.001 右肺中叶病灶体积占比/% 0.53(0~4.45) 34.73(20.29~51.61) 64.665 <0.001 右肺中叶病灶体积 1.87(0~12.77) 101.87(54.41~153.72) 62.733 <0.001 右肺下叶病灶体积占比/% 3.32(0.42~14.45) 57.96(38.89~63.36) 67.346 <0.001 右肺下叶病灶体积 28.11(3.75~86.83) 292.99(219.19~430.41) 62.544 <0.001 左肺上叶病灶体积占比/% 0.25(0~2.49) 36.66(19.28~53.40) 72.725 <0.001 左肺上叶病灶体积 2.46(0~22.60) 217.79(128.16~347.07) 70.645 <0.001 左肺下叶病灶体积占比/% 2.08(0.20~12.09) 54.76(37.02~64.50) 57.120 <0.001 左肺下叶病灶体积 15.62(1.64~73.52) 283.51(168.11~329.39) 53.018 <0.001 各组病灶均以磨玻璃密度影(ground glass opacity,GGO)为主,A组以密度为 -570~-470 HU病灶为主,占比达13.89%;其次为 -470~-370 HU,占比为11.07%;密度为30~70 HU实性病灶及密度为 -70~30 HU较少,占比仅3.22%、4.75%。B组大部分呈磨玻璃密度影,以病灶密度为 -570~-470 HU、-470~-370 HU与 -370~-270 HU为主,占比分别为13.18%、12.58% 和12.52%。A组和B组密度为 -570~-470 HU的病灶占比差异无统计学意义。余各密度病灶体积及体积占比高于A组,呈病灶密度越高,B组占比较A组越高的趋势(表2)。
表 2 A组和B组病灶密度及各密度病灶体积占比Table 2. Lesion densities and volume proportion of each density in groups A and B病灶密度(HU)及占比 组别 统计检验 A组 B组 Z P -570~-470体积 12.15(2.46~35.315) 141.75(101.24~197.83) 70.193 <0.001 -570~-470体积占比/% 13.89(11.38~16.24) 13.18(11.11~15.10) 0.662 0.416 -470~-370体积 9.79(1.91~28.07) 144.65(113.14~181.30) 73.162 <0.001 -470~-370体积占比/% 11.07(8.58~13.55) 12.58(10.80~15.05) 8.352 0.004 -370~-270体积 7.42(1.37~21.21) 125.49(100.26~174.70) 73.630 <0.001 -370~-270体积占比/% 8.48(6.12~10.93) 12.52(9.88~15.32) 22.392 <0.001 -270~-170体积 5.28(1.03~15.84) 107.73(84.18~174.06) 72.647 <0.001 -270~-170体积占比/% 6.27(4.32~8.95) 10.10(8.18~14.70) 22.871 <0.001 -170~-70体积 3.76(0.72~12.42) 88.10(55.36~146.54) 68.923 <0.001 -170~-70体积占比/% 4.75(2.76~7.27) 7.69(6.34~11.04) 17.093 <0.001 -70~30体积 2.33(0.44~9.57) 62.38(29.04~83.22) 63.385 <0.001 -70~30体积占比/% 3.22(1.49~5.77) 5.25(3.41~6.60) 9.336 0.002 30~70体积 0.47(0.05~2.08) 10.84(5.74~18.90) 57.192 <0.001 30~70体积占比/% 0.60(0.18~1.50) 1.27(0.60~1.63) 5.928 0.015 其他 39.63(8.42~110.95) 307.92(250.60~534.06) 57.426 <0.001 其他占比/% 47.91(35.69~59.69) 36.02(23.45~42.65) 16.879 <0.001 2.3 病灶影像征象
A组主要表现为单个(图2和图3)或2个及2个以上肺叶(图4、图5和图7)大小不等片状磨玻璃阴影、实变影,部分较淡薄,胸膜下、肺叶外周带分布多见(图3~图5和图7),右肺中叶受累相对少见,病灶形态呈不规则斑片状、小片状、条片状,也可呈边缘模糊、伴有晕征的小叶中心结节(图2~图7),无胸腔积液及淋巴结肿大。
![]() 图 2 新型冠状病毒感染中型未转重症患者男,34岁,右肺上叶胸膜下斑片状磨玻璃密度影,可见小血管穿行。Figure 2. COVID-19 medium type that was not converted to a severe case
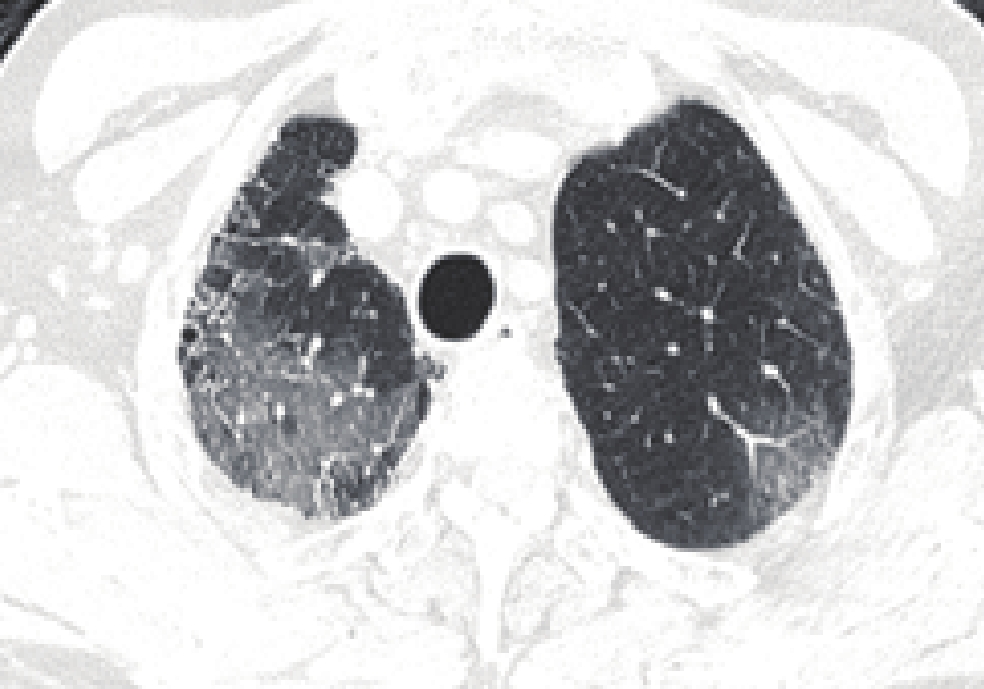
图 2 新型冠状病毒感染中型未转重症患者男,34岁,右肺上叶胸膜下斑片状磨玻璃密度影,可见小血管穿行。Figure 2. COVID-19 medium type that was not converted to a severe case![]() 图 4 新型冠状病毒感染中型未转重症患者女,59岁,左肺上叶胸膜下束带状实变影、周围磨玻璃影。Figure 4. COVID-19 medium type that was not converted to a severe case
图 4 新型冠状病毒感染中型未转重症患者女,59岁,左肺上叶胸膜下束带状实变影、周围磨玻璃影。Figure 4. COVID-19 medium type that was not converted to a severe case![]() 图 3 新型冠状病毒感染中型未转重症患者男,52岁,双肺下叶多发斑片状、小片状或小结节状磨玻璃密度影及条索,外带为主,可见小血管穿行。Figure 3. COVID-19 medium type that was not converted to a severe case
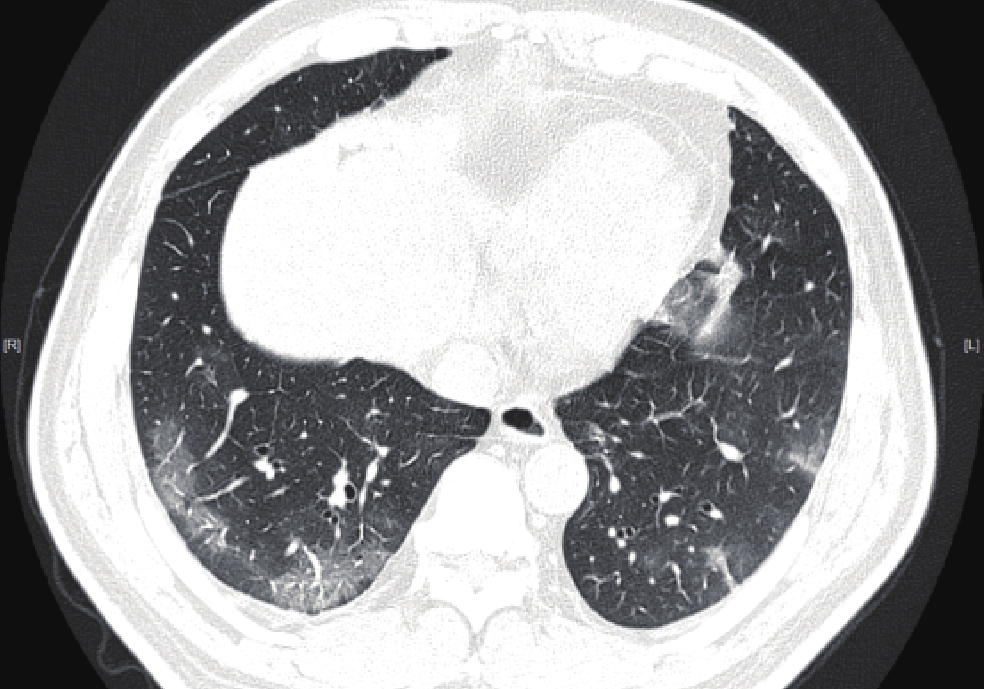
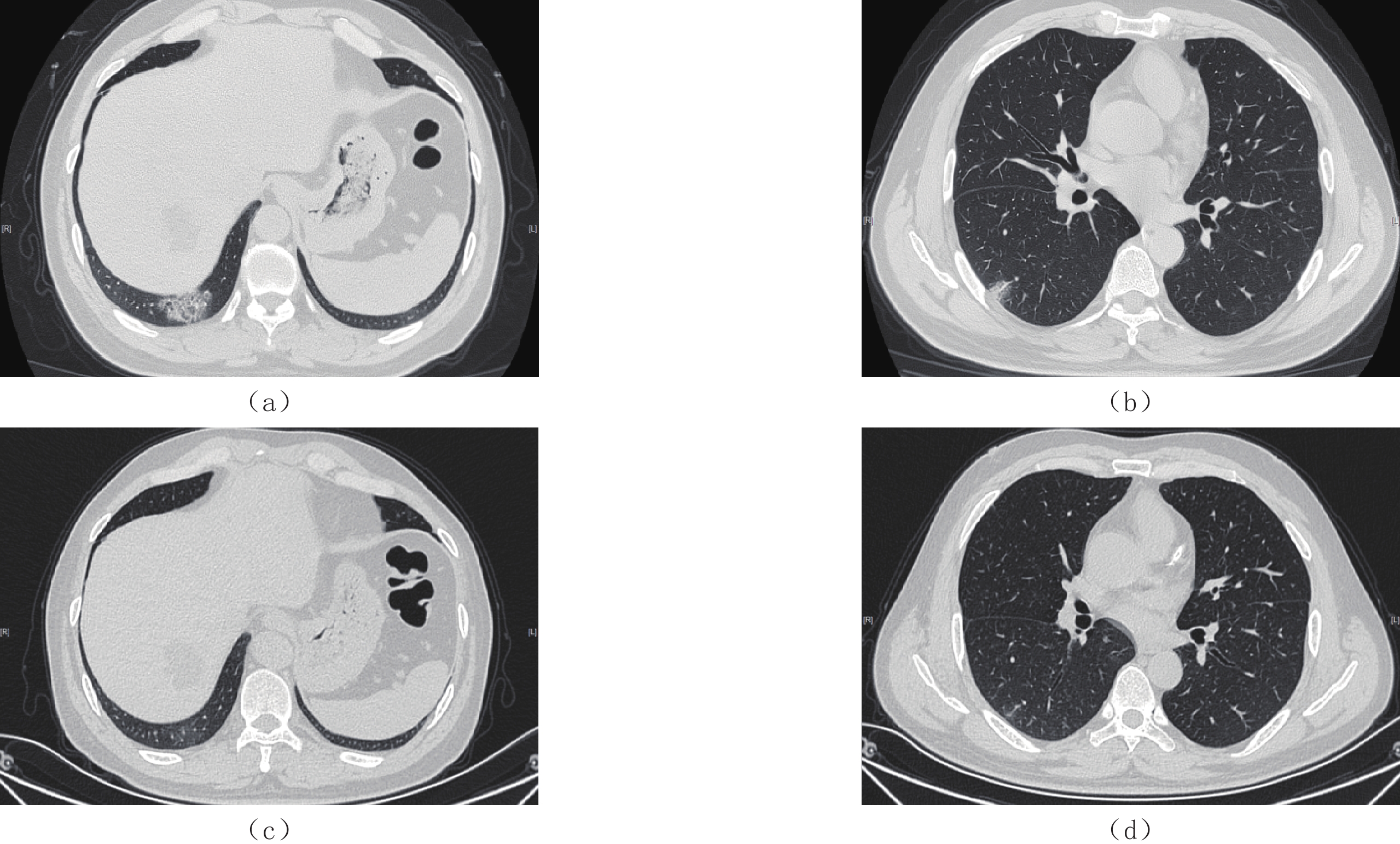
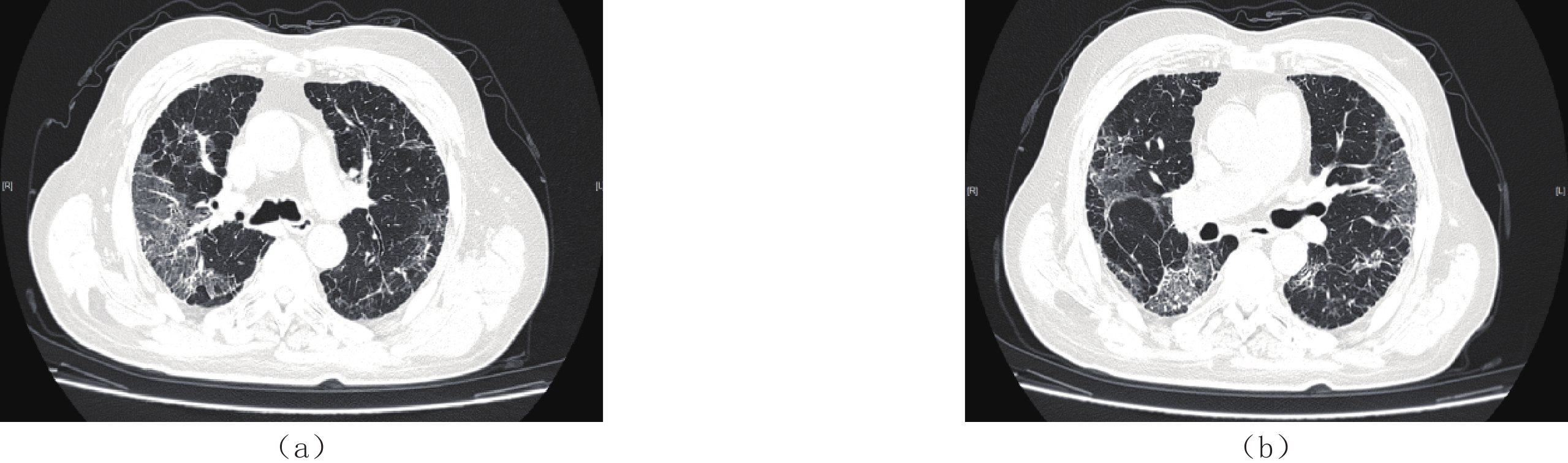
图 3 新型冠状病毒感染中型未转重症患者男,52岁,双肺下叶多发斑片状、小片状或小结节状磨玻璃密度影及条索,外带为主,可见小血管穿行。Figure 3. COVID-19 medium type that was not converted to a severe case![]() 图 5 新型冠状病毒感染中型未转重症患者男性,53岁。(a)和(b)2022.12.15右肺下叶胸膜下斑片状磨玻璃密度影,边缘模糊、内可见增粗小血管。(c)和(d)2023.01.06复查,病灶基本吸收,可见淡薄磨玻璃影残留。Figure 5. COVID-19 medium type that was not converted to a severe case
图 5 新型冠状病毒感染中型未转重症患者男性,53岁。(a)和(b)2022.12.15右肺下叶胸膜下斑片状磨玻璃密度影,边缘模糊、内可见增粗小血管。(c)和(d)2023.01.06复查,病灶基本吸收,可见淡薄磨玻璃影残留。Figure 5. COVID-19 medium type that was not converted to a severe case![]() 图 6 新型冠状病毒感染中型未转重症患者男性,66岁,右肺上叶片状GGO,左肺上叶斑片状GGO,可见小叶间隔增厚及增粗小血管。Figure 6. COVID-19 medium type that was not converted to a severe case
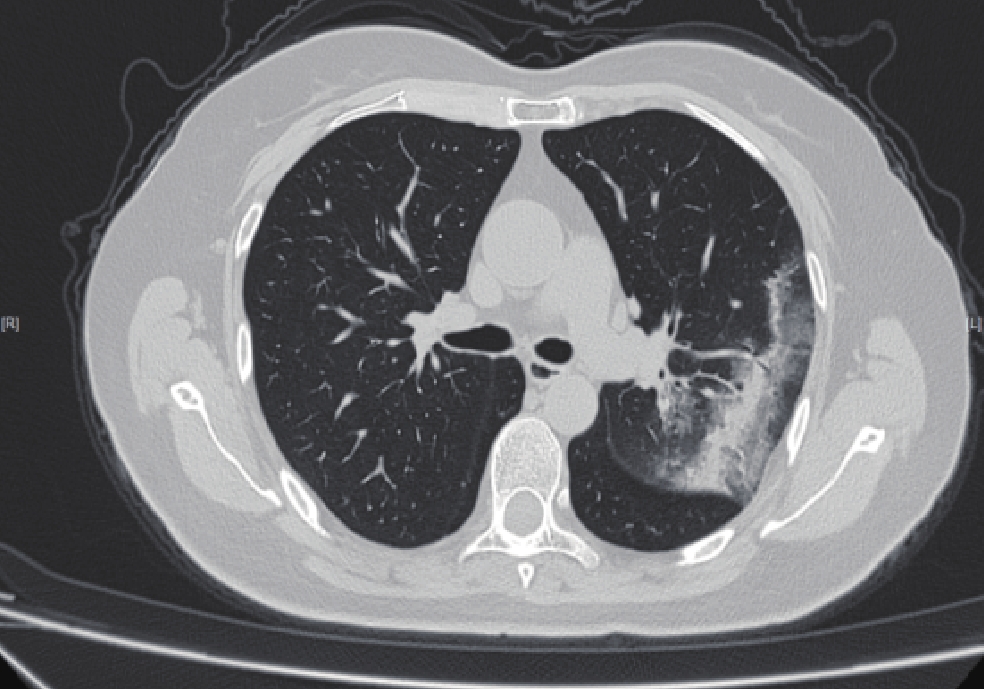
图 6 新型冠状病毒感染中型未转重症患者男性,66岁,右肺上叶片状GGO,左肺上叶斑片状GGO,可见小叶间隔增厚及增粗小血管。Figure 6. COVID-19 medium type that was not converted to a severe case![]() 图 7 新型冠状病毒感染中型转重症患者男性,67岁,双肺外周带分布磨玻璃密度影,沿支气管血管束分布,内见网格影、条索,血管增粗及胸膜增厚。Figure 7. COVID-19 medium type that was converted to a severe case
图 7 新型冠状病毒感染中型转重症患者男性,67岁,双肺外周带分布磨玻璃密度影,沿支气管血管束分布,内见网格影、条索,血管增粗及胸膜增厚。Figure 7. COVID-19 medium type that was converted to a severe caseB组呈双肺广泛分布的GGO、网状结构、条索、微囊性改变或混合表现,更容易出现的特征为实性病灶或实性病灶与磨玻璃病灶并存、铺路石征、支气管充气征、支气管壁增厚、牵连性支气管扩张、胸膜下线、血管增粗等,病变密度较高,实变范围较大,大多沿支气管血管束及胸膜下、肺外带分布为主(图7)。
3. 讨论
COVID-19主要传播途径为呼吸道传播[5-6],传染性较高,人群普遍易感,新型冠状病毒(SARS-CoV-2)变异影响病毒与人体细胞的亲和力,改变病毒的传染性和致病性。Omicron变异株由于传染和免疫逃避能力增强,成为全球流行优势毒株,其致病力较早期毒株明显下降,但仍有部分患者迅速进展为重症。
2022年12月《关于进一步优化落实新冠肺炎疫情防控措施的通知》、《关于印发对新型冠状病毒感染实施“乙类乙管”总体方案的通知》陆续发布,我国的新型冠状病毒感染疫情防控“关口前移”,基层医疗机构面临感染人数突增、重症患者明显增多、医护人员大面积感染等问题,重症患者的救治成为医务人员的工作重点。胸部CT平扫快捷、高效,在COVID-19排查及病情评估中具有不可替代的作用,特别是薄层高分辨率CT可准确显示肺部病灶的细微结构,是当前筛查与鉴别COVID-19的重要手段之一[7]。
COVID-19胸部CT表现多为肺外带、胸膜下的磨玻璃斑片影或磨玻璃结节,较重者表现为双肺多发实变影,体积较大,双肺广泛实变者形成白肺。COVID-19重症患者病情危重、进展迅速,缺乏有效的治疗手段,病死率较高;早期评估COVID-19肺部病变体积、密度等参数可为临床治疗提供依据;然而预测COVID-19是否会进展为重症具有挑战性。客观准确的认识对判断疾病的预后至关重要,而既往影像诊断医师对病变的认识多依赖于主观经验,近年来随着空间识别能力强大的深度学习与医学影像技术的结合,可以从原始图像自适应学习识别并提取高层特征,并不断进行自我学习,优化读片效果,疾病诊断能力取得了突破性的进展[8]。
深度学习可定量分析针对COVID-19的胸部CT表现进行算法的迭代和优化,通过计算肺炎病灶的密度、体积及占比来判断病变的严重程度,可对病灶范围及严重程度进行量化。有研究表明目前已开发的COVID-19相关AI模型诊断准确率可达94.00%~95.24%[9];Yang等[10]的研究显示深度学习可识别 COVID-19并与细菌性肺炎相鉴别,灵敏度达96%;有研究[11]利用AI系统及CT影像和临床数据成功地预测了患者进展为重症的时间,对患者进行准确分类并确定了高危患者,具有进行个性化治疗的潜在价值。
本研究中A组450例患者胸部CT多呈双肺多叶段分布边缘模糊的GGO,也可呈伴有晕征的小叶中心结节,可能原因为肺泡内渗出和水肿并不明显[12];部分可见小血管增粗、局部小叶间隔网格状增厚及空气支气管征,原因为不同程度的弥漫性肺泡损伤,可能由炎性细胞因子风暴引起[13];病灶多以胸膜下肺外周分布为主是由于新冠病毒颗粒小,经呼吸道吸入后直达肺泡位置,胸膜下区是肺的最末梢结构,病毒与该区域的Ⅱ型肺泡上皮细胞结合,引起肺泡壁损伤;病灶密度为磨玻璃最多,依次为实性周围磨玻璃影、实性,也可各种征象共存,可能原因[14-17]是肺泡上皮受到病毒侵犯,炎症及渗出液导致肺泡间隔增厚、肺泡部分萎陷。本研究中,非重症组更容易出现的CT征象为磨玻璃密度结节,甚至结节边缘可见毛刺、与邻近胸膜牵拉,需通过复查与周围型肺癌鉴别。
转为重症的B组胸部CT多表现为以双肺多叶受累、弥漫分布的实变影合并GGO,可见多发条索及空气支气管征,同之前的研究一致[18],感染肺叶数以及各肺叶感染体积占比、总感染体积占比均高于A组,且病灶累及肺叶较A组多,各肺叶感染体积及双肺感染总体积均高于A组。吸收后胸部CT表现为轻微的胸膜下网状结构、磨玻璃影或两者都有。A组和B组均未见胸腔积液与纵隔、肺门淋巴结肿大。以上结果表明感染肺叶数多、病变以弥漫性实变为主,感染体积较大、占比较高者,容易转为重症。非重症组和重症组无明显差异的CT征象包括磨玻璃病灶、小叶间隔增厚、网状改变、胸膜下分布分布。
综上,病灶分布、病灶成分、CT征象在新型冠状病毒感染未转为重症组和转为重症组间具有显著差异,转为重症组更易出现实性病灶、磨玻璃与实性混合型病灶、铺路石征、血管增粗等多种征象并存的现象。应用深度学习定量测量技术准确分析病灶可对COVID-19的预后提前做出判断,指导临床及早调整治疗策略,起到预警重症作用。
现阶段COVID-19主要需结合流行病学与甲型H1N1流感鉴别。甲型H1N1流感致急性肺损伤很少见到磨玻璃密度向肺实变密度发展,一般经治疗后均逐渐消失[19],且大部分消散较快。有研究认为,磨玻璃影、实变和支气管增厚是甲型流感肺炎的常见HRCT影像学表现,但无小叶间隔增厚[2,7,20]。在COVID-19疫情暴发期间,大多数病毒性肺炎是由COVID-19引起,胸部CT筛查行之有效。在非流行期胸部CT可以用来判断患者是否感染了病毒性肺炎,而由哪种病毒引起单纯通过影像明确诊断较为困难。因此在COVID-19流行期基于深度学习建立的胸部CT诊断模型可快速有效筛查COVID-19。
本研究的局限性:①病例均来自于门诊,未纳入发热后未至医院行CT检查的病例及胸部CT无肺炎表现的轻型COVID-19病例,且本研究去除了由于图像缺陷未能进行病灶的AI定量分析的病例,可能存在病例选择性偏倚;②肺炎 AI定量工具准确性仍需进一步验证。
综上所述,感染体积较大、病灶偏实性及多种CT征象并存常提示肺部炎症较重,容易进展为重症。基于深度学习的COVID-19肺炎定量工具能够客观分析胸部CT病灶,较为精确的评估病变严重程度,对有重症转归倾向的病例可起到预警作用,有利于指导临床进一步预测病情发展、制定合理的诊疗方案。
-
![]()
图 1 推想人工智能评估新型冠状病毒奥密克戎变异株感染患者肺内病灶体积示意图
患者,男,86岁,确诊为新型冠状病毒奥密克戎变异株感染。
Figure 1. Schematic diagram of InferVision artificial Intelligence evaluating the volume of lesions in the lung of patients infected with the COVID-19 omicron variant
![]()
图 2 新型冠状病毒感染中型未转重症患者
男,34岁,右肺上叶胸膜下斑片状磨玻璃密度影,可见小血管穿行。
Figure 2. COVID-19 medium type that was not converted to a severe case
![]()
图 4 新型冠状病毒感染中型未转重症患者
女,59岁,左肺上叶胸膜下束带状实变影、周围磨玻璃影。
Figure 4. COVID-19 medium type that was not converted to a severe case
![]()
图 3 新型冠状病毒感染中型未转重症患者
男,52岁,双肺下叶多发斑片状、小片状或小结节状磨玻璃密度影及条索,外带为主,可见小血管穿行。
Figure 3. COVID-19 medium type that was not converted to a severe case
![]()
图 5 新型冠状病毒感染中型未转重症患者
男性,53岁。(a)和(b)2022.12.15右肺下叶胸膜下斑片状磨玻璃密度影,边缘模糊、内可见增粗小血管。(c)和(d)2023.01.06复查,病灶基本吸收,可见淡薄磨玻璃影残留。
Figure 5. COVID-19 medium type that was not converted to a severe case
![]()
图 6 新型冠状病毒感染中型未转重症患者
男性,66岁,右肺上叶片状GGO,左肺上叶斑片状GGO,可见小叶间隔增厚及增粗小血管。
Figure 6. COVID-19 medium type that was not converted to a severe case
![]()
图 7 新型冠状病毒感染中型转重症患者
男性,67岁,双肺外周带分布磨玻璃密度影,沿支气管血管束分布,内见网格影、条索,血管增粗及胸膜增厚。
Figure 7. COVID-19 medium type that was converted to a severe case
表 1 A组和B组全肺及各肺叶病灶体积及体积占比
Table 1 The lesion volume and proportion of the whole lung and each lung lobe in groups A and B
指标 组别 统计检验 A组(n=450) B组(n=27) Z P 全肺病灶体积占比/% 2.43(0.45~7.43) 40.45(33.47~46.60) 75.868 <0.001 全肺病灶体积 87.12(17.73~262.20) 1239.21(841.54~1395.12) 72.842 <0.001 右肺上叶病灶体积占比/% 0.50(0~3.00) 35.70(20.84~50.32) 69.027 <0.001 右肺上叶病灶体积 4.56(0~24.22) 225.10(120.17~317.48) 64.978 <0.001 右肺中叶病灶体积占比/% 0.53(0~4.45) 34.73(20.29~51.61) 64.665 <0.001 右肺中叶病灶体积 1.87(0~12.77) 101.87(54.41~153.72) 62.733 <0.001 右肺下叶病灶体积占比/% 3.32(0.42~14.45) 57.96(38.89~63.36) 67.346 <0.001 右肺下叶病灶体积 28.11(3.75~86.83) 292.99(219.19~430.41) 62.544 <0.001 左肺上叶病灶体积占比/% 0.25(0~2.49) 36.66(19.28~53.40) 72.725 <0.001 左肺上叶病灶体积 2.46(0~22.60) 217.79(128.16~347.07) 70.645 <0.001 左肺下叶病灶体积占比/% 2.08(0.20~12.09) 54.76(37.02~64.50) 57.120 <0.001 左肺下叶病灶体积 15.62(1.64~73.52) 283.51(168.11~329.39) 53.018 <0.001  下载: 导出CSV
下载: 导出CSV
表 2 A组和B组病灶密度及各密度病灶体积占比
Table 2 Lesion densities and volume proportion of each density in groups A and B
病灶密度(HU)及占比 组别 统计检验 A组 B组 Z P -570~-470体积 12.15(2.46~35.315) 141.75(101.24~197.83) 70.193 <0.001 -570~-470体积占比/% 13.89(11.38~16.24) 13.18(11.11~15.10) 0.662 0.416 -470~-370体积 9.79(1.91~28.07) 144.65(113.14~181.30) 73.162 <0.001 -470~-370体积占比/% 11.07(8.58~13.55) 12.58(10.80~15.05) 8.352 0.004 -370~-270体积 7.42(1.37~21.21) 125.49(100.26~174.70) 73.630 <0.001 -370~-270体积占比/% 8.48(6.12~10.93) 12.52(9.88~15.32) 22.392 <0.001 -270~-170体积 5.28(1.03~15.84) 107.73(84.18~174.06) 72.647 <0.001 -270~-170体积占比/% 6.27(4.32~8.95) 10.10(8.18~14.70) 22.871 <0.001 -170~-70体积 3.76(0.72~12.42) 88.10(55.36~146.54) 68.923 <0.001 -170~-70体积占比/% 4.75(2.76~7.27) 7.69(6.34~11.04) 17.093 <0.001 -70~30体积 2.33(0.44~9.57) 62.38(29.04~83.22) 63.385 <0.001 -70~30体积占比/% 3.22(1.49~5.77) 5.25(3.41~6.60) 9.336 0.002 30~70体积 0.47(0.05~2.08) 10.84(5.74~18.90) 57.192 <0.001 30~70体积占比/% 0.60(0.18~1.50) 1.27(0.60~1.63) 5.928 0.015 其他 39.63(8.42~110.95) 307.92(250.60~534.06) 57.426 <0.001 其他占比/% 47.91(35.69~59.69) 36.02(23.45~42.65) 16.879 <0.001
下载: 导出CSV
-
[1] 中华人民共和国国家卫生健康委员会. 关于印发对新型冠状病毒感染实施“乙类乙管”总体方案的通知 [EB/OL]. (2022-12-26)[2023-01-05]. http://www.nhc.gov.cn/xcs/zhengcwj/202212/e97e4c449d7a475794624b8ea12123c6.shtml. [2] 中华医学会放射学分会. 新型冠状病毒肺炎的放射学诊断: 中华医学会放射学分会专家推荐意见(第一版)[J]. 中华放射学杂志, 2020,54: E001−E001. DOI: 10.3760/cma.j.issn.1005-1201.2020.0001. Chinese Society of Radiology. Radiological diagnosis of new coronavirus infected pneumonitis: Expert recommendation from the Chinese Society of Radiology (First edition)[J]. Chinese Journal of Radiology, 2020, 54: E001−E001. DOI: 10.3760/cma.j.issn.1005-1201.2020.0001. (in Chinese).
[3] 孙莹, 李玲, 刘晓燕, 等. 早期新型冠状病毒肺炎的胸部薄层平扫CT表现特征[J]. CT理论与应用研究, 2023,32(1): 131−138. DOI: 10.15953/j.ctta.2023.006. SUN Y, LI L, LIU X Y, et al. Imaging features of early COVID-19 on chest thin-slice non-enhanced CT[J]. CT Theory and Applications, 2023, 32(1): 131−138. DOI: 10.15953/j.ctta.2023.006. (in Chinese).
[4] 中华人民共和国国家卫生健康委员会. 新型冠状病毒感染诊疗方案(试行第十版)[EB/OL]. (2023-01-06)[2023-01-20]. http://www.nhc.gov.cn/ylyjs/pqt/202301/32de5b2ff9bf4eaa88e75bdf7223a65a.shtml. [5] LI Q, GUAN X, WU P, et al. Early transmission dynamics in Wuhan, china, of novel coronavirus infected pneumonia[J]. The New England Journal of Medicine, 2020, 382(13): 1199−1207. DOI: 10.1056/NEJMoa2001316.
[6] MUNSTER V J, KOOPMANS M, VAN D N, et al. A novel coronavirus emerging in China-key questions for impact assessment[J]. The New England Journal of Medicine, 2020, 382(8): 692−694. DOI: 10.1056/NEJMp2000929.
[7] 靳英辉, 蔡林, 程真顺, 等. 新型冠状病毒 (2019-nCoV) 感染的肺炎诊疗快速建议指南(标准版)[J]. 解放军医学杂志, 2020,45(1): 1−20. DOI: 10.11855/j.issn.0577-7402.2020.01.01. JIN Y H, CAI L, CHENG Z S, et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (Standard version)[J]. Medical Journal of Chinese People's Liberation Army, 2020, 45(1): 1−20. DOI: 10.11855/j.issn.0577-7402.2020.01.01. (in Chinese).
[8] KERMANY D S, GOLDBAUM M, CAI W J, et al. Identifying medical diagnoses and treatable diseases by image-based deep learning[J]. Cell, 2018, 172(5): 1122−1131. DOI: 10.1016/j.cell.2018.02.010.
[9] CHEN J, WU L L, ZHANG J, et al. Deep learning-based model for detecting 2019 novel coronaviruspneumonia on high-resolution computed tomography[J]. Scientificreports, 2020, 10(1): 1−11. DOI: 10.1038/s41598-020-76282-0.
[10] YANG S, JIANG L, CAO Z, et al. Deep learning for detecting corona virus disease 2019 (COVID-19) on high resolution computed tomography: A pilot study[J]. Annals of Translational Medicine, 2020, 8(7): 450. DOI: 10.21037/atm.2020.03.132.
[11] WANG R, JIAO Z, YANG L, et al. Artificial intelligence for prediction of COVID-19 progression using CT imaging and clinical data[J]. European Radiology, 2022, 32(1): 205−212. DOI: 10.1007/s00330-021-08049-8.
[12] NICHOLLS J M, POON L L, LEE K C, et al. Lung pathology of severe acute respiratory syndrome[J]. Lancet, 2003, 361(9371): 1773−1778. DOI: 10.1016/s0140-6736(03)13413-7.
[13] HUANG C L, WANG Y M, LI X W, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China[J]. Lancet, 2020, 395(10223): 497−506. DOI: 10.1016/S0140-6736(20)30183-5.
[14] 黄益龙, 张振光, 李翔, 等. CT影像组学联合征象鉴别新型冠状病毒肺炎与其他病毒性肺炎的价值[J]. 中华放射学杂志, 2022,56(1): 36−42. DOI: 10.3760/cma.j.cn112149-20201220-01318. HUANG Y L, ZHANG Z G, LI X, et al. The value of CT signs combined with radiomics in the differentiation of COVID-19 from other viral pneumonias[J]. Chinese Journal of Radiology, 2022, 56(1): 36−42. DOI: 10.3760/cma.j.cn112149-20201220-01318. (in Chinese).
[15] 赵小二, 邓克学, 王朋. 不同阶段新型冠状病毒肺炎的CT影像演变分析[J]. 实用放射学杂志, 2021,37(8): 1254−1257. doi: 10.3969/j.issn.1002-1671.2021.08.008 ZHAO X E, DENG K X, WANG P. Analysis of the CT manifestations changes of COVID-19 at different stages[J]. Journal of Practical Radiology, 2021, 37(8): 1254−1257. (in Chinese). doi: 10.3969/j.issn.1002-1671.2021.08.008
[16] 吴杰, 肖安岭, 顾金凤. 多层螺旋CT对新型冠状病毒肺炎的临床诊断价值[J]. 实用放射学杂志, 2021,37(5): 746−748. DOI: 10.3969/j.issn.1002-1671.2021.05.013. WU J, XIAO A L, GU J F. Clinical value of MSCT in the diagnosis of COVID-19[J]. Journal of Practical Radiology, 2021, 37(5): 746−748. DOI: 10.3969/j.issn.1002-1671.2021.05.013. (in Chinese).
[17] 余成成, 杨彦鸿, 胡天丽, 等. 新型冠状病毒B.1.617.2变异株感染者高分辨率CT与临床特点[J]. 中华放射学杂志, 2021,55(10): 1054−1058. DOI: 10.3760/cma.j.cn112149-20210618-00574. YU C C, YANG Y H, HU T L, et al. High resolution CT findings and clinical features of the novel corona-virus B.1.617.2 variant[J]. Chinese Journal of Radiology, 2021, 55(10): 1054−1058. DOI: 10.3760/cma.j.cn112149-20210618-00574. (in Chinese).
[18] 赵建华, 柴军, 张晓琴, 等. 基于深度学习的新型冠状病毒肺炎转归胸部CT评价[J]. 国际放射医学核医学杂志, 2020,44(12): 737−743. DOI: 10.3760/cma.j.cn121381-202004048-00101. ZHAO J H, CHAI J, ZHANG X Q, et al. Chest CT evaluation of COVID-19 outcome based on deep learning[J]. International Journal of Radiation Medicine and Nuclear Medicine, 2020, 44(12): 737−743. DOI: 10.3760/cma.j.cn121381-202004048-00101. (in Chinese).
[19] 谢正平, 戴峰, 蒋燕, 等. 重症甲型H1N1流感急性肺损伤的高分辨率CT影像学分析[J]. 现代医学, 2012,40(3): 276−280. doi: 10.3969/j.issn.1671-7562.2012.03.007 XIE Z P, DAI F, JIANG Y, et al. HRCT imaging analysis of influenza a H1N1 complicated with severe lung injury[J]. Modern Medical Journal, 2012, 40(3): 276−280. (in Chinese). doi: 10.3969/j.issn.1671-7562.2012.03.007
[20] 刘玉建, 仲建全, 冯浩, 等. 新型冠状病毒肺炎患者的高分辨率CT影像学特征[J]. 医疗装备, 2022,35(11): 1−4. doi: 10.3969/j.issn.1002-2376.2022.11.001 LIU Y J, ZHONG J Q, FENG H, et al. Imaging characteristics of high resolution CT for patients with corona virus disease 2019[J]. Medical Equipment, 2022, 35(11): 1−4. (in Chinese). doi: 10.3969/j.issn.1002-2376.2022.11.001

计量
- 文章访问数: 207
- HTML全文浏览量: 61
- PDF下载量: 28


