
Analysis of Chest Computed Tomography Manifestations of Coronavirus Disease 2019 in Different Age Groups
-
摘要: 目的:分析不同年龄人群新型冠状病毒感染(COVID-19)胸部CT影像特征,提高对不同年龄人群COVID-19影像表现的认识。方法:回顾性分析476例COVID-19的胸部CT资料,男275例,女201例,按照不同年龄段分为A组(0~45岁)33人、B组(45~60岁)72人、C组(60~75岁)203人、D组(75岁以上)168人,共4组,比较4组病例胸部CT病灶累及肺叶侧别、数目、密度和病灶分布等CT基本征象及基于深度学习的病灶体积、体积占比和密度等的差异。结果:476例COVID-19患者均有流行病学史,性别在各组间差异无统计学意义。4组病例双肺下叶病灶最为多见,A组病灶多位于单侧肺,C组和D组病灶以双肺分布多见。各组病灶体积、体积占比随年龄增大呈递增趋势,且分布均以双肺下叶为主,其中A、C和D组均以右肺下叶最为常见且体积及体积占比最大,B组以左肺下叶病灶体积及占比较大;与A组比较,C组各项指标增大,差异均有统计学意义,且右肺下叶病灶体积与B组比较差异有统计学意义;D组左肺上叶病灶体积与A组比较明显增大,占比较A组和B组明显增大,余D组全肺及右肺上叶、中叶、下叶及左肺下叶病灶体积及体积占比较A、B和C组均明显增大,且差异有统计学意义。病灶均以磨玻璃密度影及实变为主,A组以纯磨玻璃密度最多见,混合磨玻璃密度次之,实变密度少见;D组病灶以实变密度较多见,大多呈混合磨玻璃密度;B和C组纯磨玻璃、混合磨玻璃、实变密度病灶出现情况介于A组和D组之间;各组病灶密度均以磨玻璃密度为主,CT值区间以 -570 ~-470 HU及 -470 ~ -370 HU为主,D组各CT值区间病灶体积均较A、B和C组高,体积占比均较A组高且差异有统计学意义。结论:本组研究COVID-19患者均有流行病学史,熟悉不同年龄人群胸部CT特征可使临床诊疗工作更具针对性,可为COVID-19病情监测以及个体化防治措施提供参考。Abstract: Objective: This study aimed to analyze the chest computed tomography (CT) imaging features of coronavirus disease 2019 (COVID-19) in people of different ages and improve the understanding of the imaging manifestations of COVID-19. Methods: Chest CT data of 476 cases with COVID-19 were retrospectively analyzed, including 275 males and 201 females. The patients were divided into four groups according to different age groups: groups A (0~45 years old) 33, B (45~60 years old) 72, C (60~75 years old) 203, and D (over 75 years old) 168. A comparison was made between the four groups of patients with chest CT lesions involving lobe side, number and density, distribution, and other basic CT signs, as well as differences in lesion volume, volume proportion, and density based on deep learning. Results: All the 476 patients with COVID-19 had an epidemiological history, and there was no statistically significant difference in sex between the groups. The lesions in the lower lobes of both lungs were the most common in the four groups. The lesions in group A were mostly located in the unilateral lung, while those in groups C and D were mostly distributed in both lungs. The volume and proportion of lesions increased with age in each group, and the distribution was mainly in the lower lobe of both lungs. In groups A, C, and D, the right lower lobe was the most common and had the largest volume and proportion, while in group B, the left lower lobe had the largest volume and proportion. Compared with group A, all indexes of group C increased, and the difference was statistically significant; the lesion volume of the right inferior lobe of the lung was statistically significant compared with group B. The volume of lesions in the left upper lobe of the lung in group D was significantly increased compared with that in groups A and B, and the volume and proportion of lesions in the whole lung, upper, middle, and lower lobes of the right lung, and the lower lobe of the left lung in group D were significantly increased compared with that in groups A, B and C, and the difference was statistically significant. In group A, the density of pure ground glass was the most common, followed by the density of mixed ground glass, and the density of solid change was rare. The solid density of lesions in group D was more common, most of which showed mixed ground glass density. The incidence of pure ground glass, mixed ground glass, and solid density lesions was higher in groups B and C than that in groups A and D. The lesion density in each group was mainly ground glass density, and the CT value ranged from −570 to −470 HU and −470 to −370 HU. The lesion volume in each CT value range of group D was higher than that in groups A, B, and C, and the volume proportion was higher than that in group A, and the difference was statistically significant. Conclusion: All patients with COVID-19 in this group have an epidemiological history. Being familiar with chest CT features of people of different ages can make clinical diagnosis and treatment more targeted and provide a reference for COVID-19 disease monitoring and individualized prevention and treatment measures.
-
Keywords:
- tomography /
- X -ray computed /
- coronavirus disease 2019
-
-
![]()
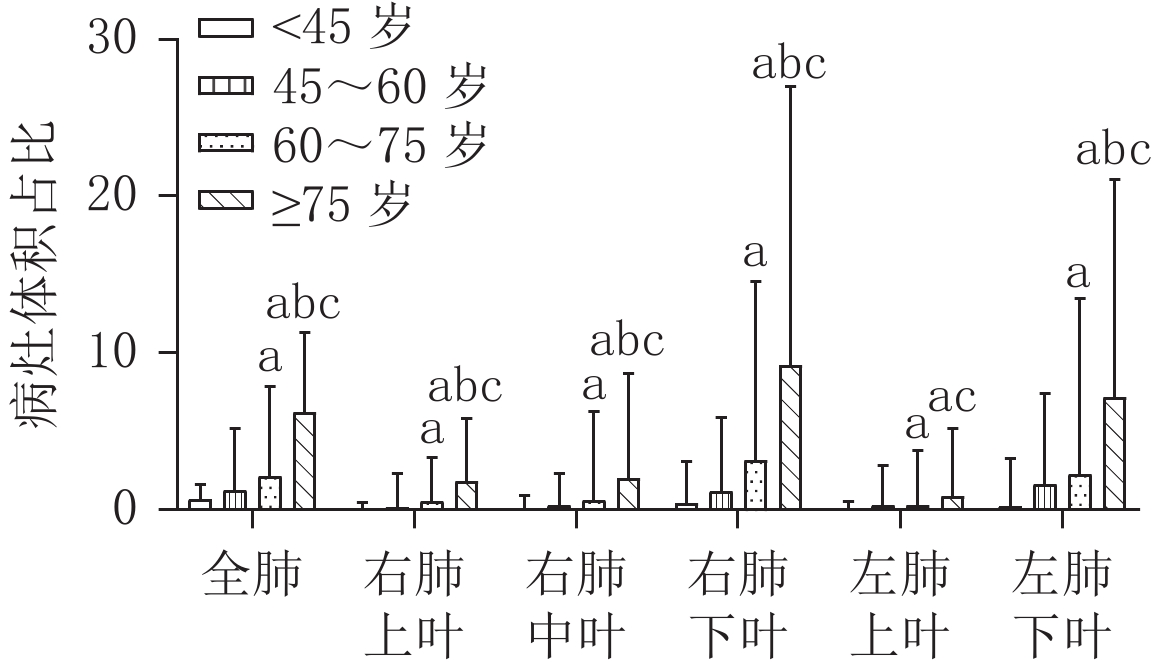
图 1 各组全肺及各肺叶病灶体积占比比较
Figure 1. Comparison of the proportion of the volume of the whole lung and each lung lobe in each group
![]()
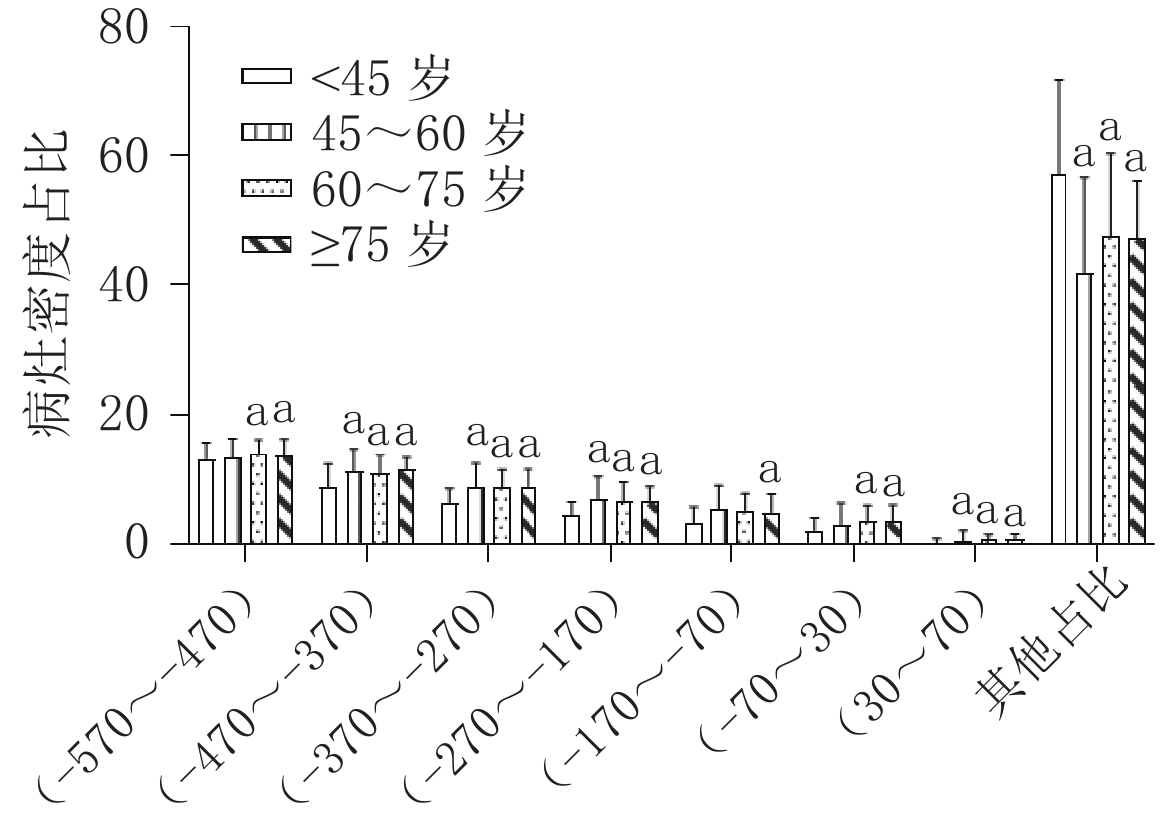
图 2 各组不同CT值病灶密度占比比较
Figure 2. Comparison of focal density ratio with different CT values in each group
![]()
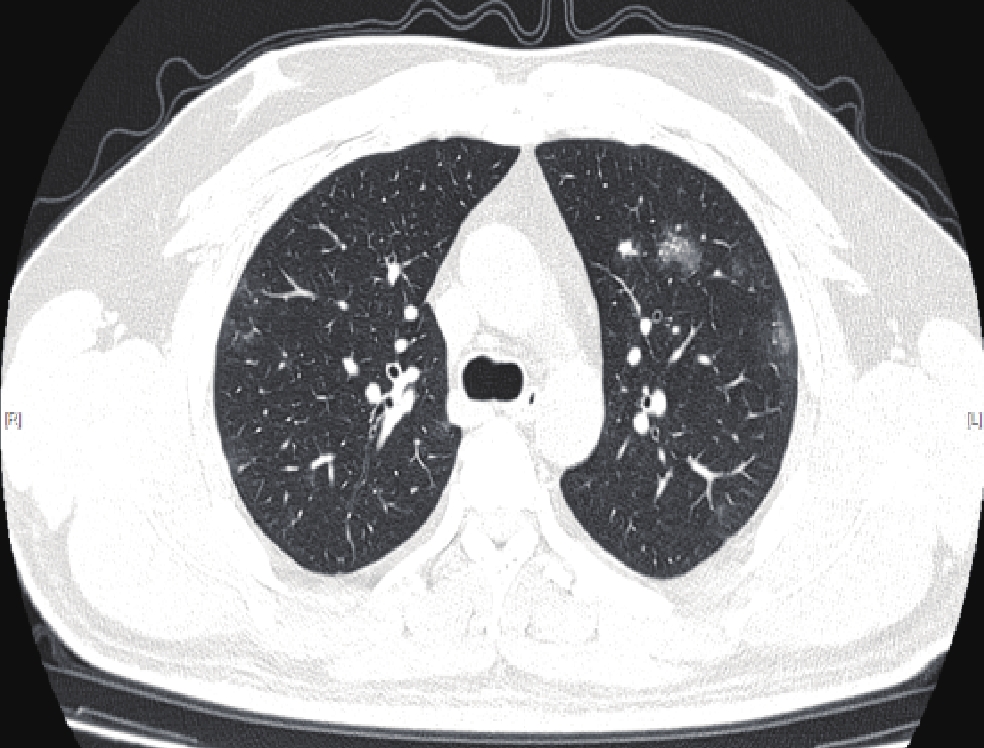
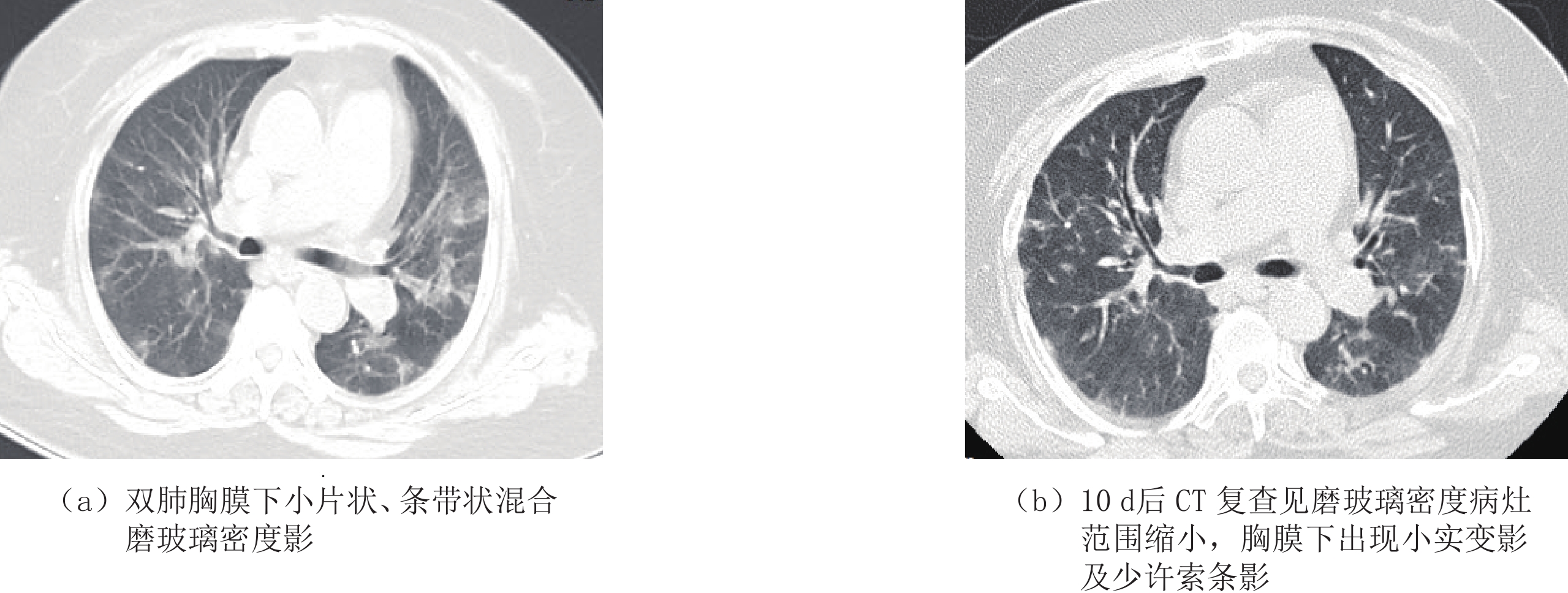
图 3 男,34岁,奥密克戎变异株BF.7感染患者
Figure 3. Male, 34 years old, Patients with Omicron variant BF.7 were infected
![]()
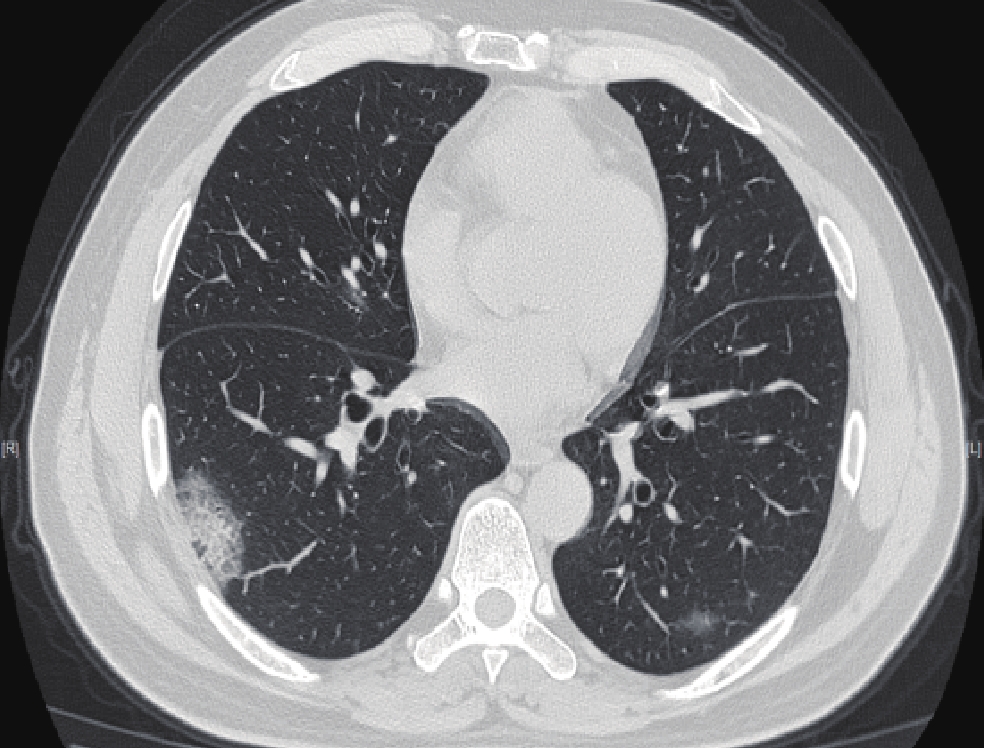
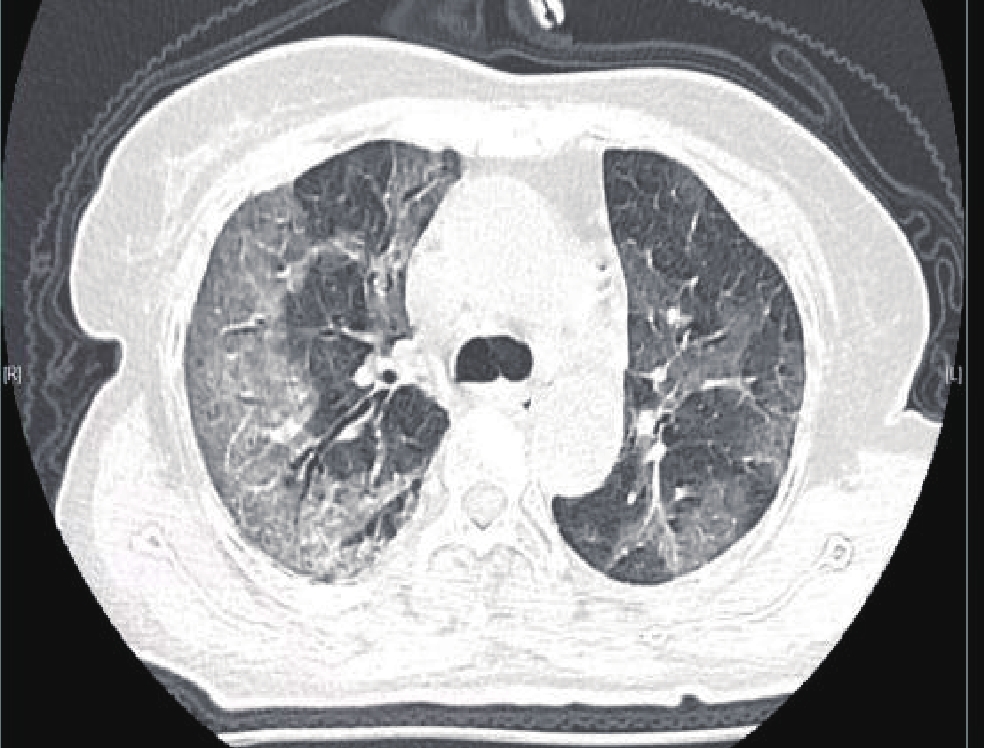
图 4 男,53岁,奥密克戎变异株BF.7感染患者
Figure 4. Male, 53 years old, Patients with Omicron variant BF.7 were infected
![]()
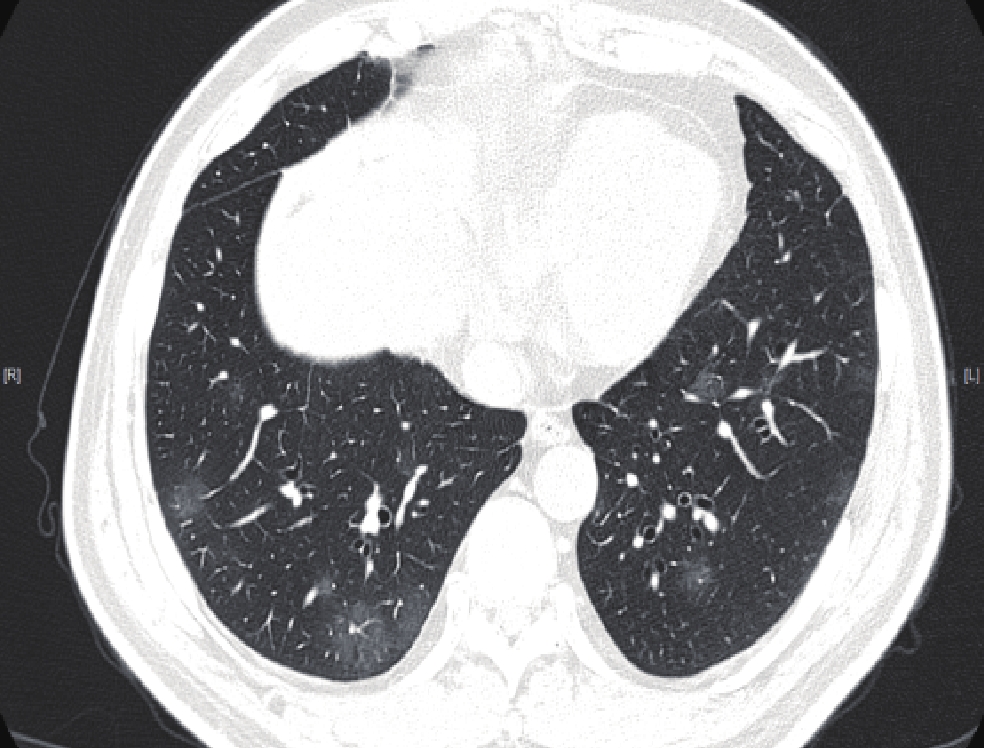
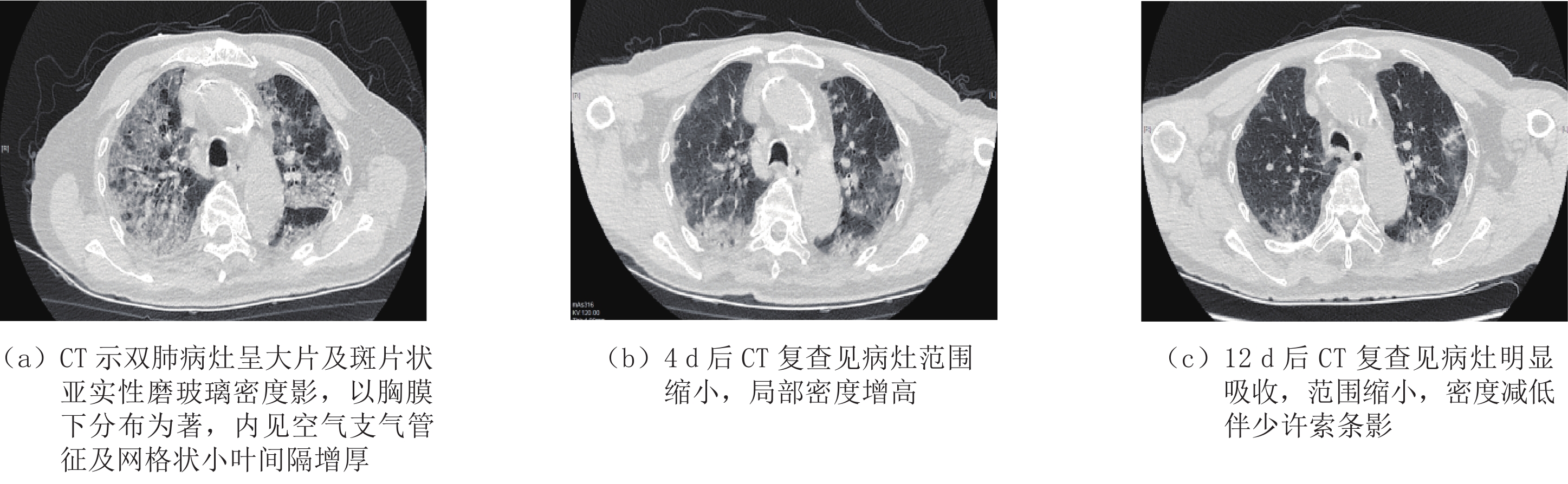
图 5 男,52岁,奥密克戎变异株BF.7感染患者
Figure 5. Male, 52 years old, Patients with Omicron variant BF.7 were infected
![]()
图 6 女,67岁,奥密克戎变异株BF.7感染患者
Figure 6. Female, 56 years old, Patients with Omicron variant BF.7 were infected
![]()
图 7 女,66岁,奥密克戎变异株BF.7感染患者
Figure 7. Female, 66 years old,Patients with Omicron variant BF.7 were infected
![]()
图 8 男,86岁,奥密克戎变异株BF.7感染患者
Figure 8. Male, 86 years old,Patients with Omicron variant BF.7 were infected
表 1 各年龄段全肺及各肺叶感染体积、体积占比比较
Table 1 Comparison of the infected volume and the proportion of infected volume in the whole lung and each lung lobe at different ages
指标 年龄段 统计检验 <45岁
(n=33)45~60岁
(n=72)60~75岁
(n=203)≥75岁
(n=168)H P 全肺病灶体积占比/% 0.63 1.24 2.14a 6.21abc 50.675 <0.001 全肺病灶体积 24.74 49.58 71.40a 189.09abc 49.238 <0.001 右肺上叶病灶体积占比/% 0.00 0.10 0.53a 1.79abc 33.428 <0.001 右肺上叶病灶体积 0.00 0.89 4.90a 14.73abc 35.840 <0.001 右肺中叶病灶体积占比/% 0.00 0.29 0.58a 1.97abc 27.296 <0.001 右肺中叶病灶体积 0.00 1.28 1.925a 5.90abc 25.960 <0.001 右肺下叶病灶体积占比/% 0.42 1.15 3.15a 9.16abc 57.565 <0.001 右肺下叶病灶体积 4.02 8.16 26.39ab 67.02abc 58.197 <0.001 左肺上叶病灶体积占比/% 0.00 0.23 0.23a 0.86ac 21.036 <0.001 左肺上叶病灶体积 0.00 2.20 2.26a 7.33a 20.602 <0.001 左肺下叶病灶体积占比/% 0.21 1.58 2.25a 7.13abc 31.768 <0.001 左肺下叶病灶体积 1.38 11.89 15.51a 45.76abc 27.555 <0.001 注:a与<45岁组比较P<0.05;b与45~60岁组比较P<0.05;c与60~75岁组比较P<0.05。  下载: 导出CSV
下载: 导出CSV
表 2 各组病灶密度及各密度病灶占比比较
Table 2 Comparison of lesion density and cases in each group
指标 组别 统计检验 A(<45岁) B(45~60岁) C(60~75岁) D(≥75岁) H P (-570~-470)体积 2.62 6.09 9.37a 27.46abc 49.529 <0.001 (-570~-470)体积占比/% 13.22 13.44 14.04a 13.77a 2.211 <0.001 (-470~-370)体积 1.97 5.08 8.97a 21.38abc 50.983 <0.001 (-470~-370)体积占比/% 8.64 11.23 a 10.97a 11.57a 9.192 0.027 (-370~-270)体积 1.46 4.46 a 6.74 16.22abc 50.336 <0.001 (-370~-270)体积占比/% 6.39 8.73 a 8.76a 8.88a 14.231 0.003 (-270~-170)体积 0.83 3.65 a 4.84a 11.60abc 48.063 <0.001 (-270~-170)体积占比/% 4.40 6.87 a 6.53a 6.50a 13.823 0.003 (-170~-70)体积 0.53 2.45 a 3.77a 8.13 abc 44.968 <0.001 (-170~-70)体积占比/% 3.28 5.32 5.22 4.91a 8.044 0.045 (-70~30)体积 0.25 1.37 2.68a 6.58abc 43.384 <0.001 (-70~30)体积占比/% 2.15 2.86 3.52a 3.40a 10.103 0.018 (30~70)体积 0.02 0.31 a 0.47a 1.39abc 41.819 <0.001 (30~70)体积占比/% 0.19 0.55 a 0.67a 0.74a 12.169 0.007 其他 12.34 17.99 31.49 88.00abc 46.874 <0.001 其他占比/% 56.94 41.72 a 47.58a 47.11a 16.631 0.001 注:a与<45岁组比较P<0.05;b与45~60岁组比较P<0.05;c与60~75岁组比较P<0.05。
下载: 导出CSV
-
[1] 中华医学会放射学分会. 新型冠状病毒肺炎的放射学诊断: 中华医学会放射学分会专家推荐意见(第一版)[J]. 中华放射学杂志, 2020,54(4): 279−285. DOI: 10.3760/cma.j.cn112149-20200205-00094. Chinese Society of Radiology. Radiological diagnosis of new coronavirus infected pneumonitis: Expert recommendation from the Chinese Society of Radiology (First edition)[J]. Chinese Journal of Radiology, 2020, 54(4): 279−285. DOI: 10.3760/cma.j.cn112149-20200205-00094. (in Chinese).
[2] CHUNG M, BERNHEIM A, MEI X Y, et al. CT imaging features of 2019 novel coronavirus (2019-nCoV)[J]. Radiology, 2020, 295(1): 202−207. DOI: 10.1148/radiol.2020200230.
[3] AI T, YANG Z L, ZHAN H Y, et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases[J]. Radiology, 2020, 296(2): E32−E40. DOI: 10.1148/radiol.2020200642.
[4] LI Q, GUAN X, WU P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus infected pneumonia[J]. The New England Journal of Medicine, 2020, 382(13): 1199−1207. DOI: 10.1056/NEJMoa2001316.
[5] MUNSTER V J, KOOPMANS M, VAN D N, et al. A novel coronavirus emerging in china-key questions for impact assessment[J]. The New England Journal of Medicine, 2020, 382(8): 692−694. DOI: 10.1056/NEJMp2000929.
[6] 中华人民共和国国家卫生健康委员会. 新型冠状病毒感染诊疗方案(试行第十版)[EB/OL]. (2023-01-06) [2023-01-20]. http://www.nhc.gov.cn/ylyjs/pqt/202301/32de5b2ff9bf4eaa88e75bdf7223a65a.shtml. [7] CHEN D D, JIANG X Q, HONG Y, et al. Can chest CT features distinguish patients with negative from those with positive initial RT-PCR results for coronavirus disease (COVID-19)?[J]. American Journal of Roentgenology, 2021, 216(1): 66−70. DOI: 10.2214/AJR.20.23012.
[8] 靳英辉, 蔡林, 程真顺, 等. 新型冠状病毒(2019-nCoV)感染的肺炎诊疗快速建议指南(标准版)[J]. 解放军医学杂志, 2020,45(1): 1−20. DOI: 10.11855/j.issn.0577-7402.2020.01.01. JIN Y H, CAI L, CHENG Z S, et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (Standard version)[J]. Medical Journal of Chinese People's Liberation Army, 2020, 45(1): 1−20. DOI: 10.11855/j.issn.0577-7402.2020.01.01. (in Chinese).
[9] 赵建华, 张晓琴, 柴军, 等. 无症状感染转确诊新型冠状病毒肺炎胸部CT分析[J]. 生物医学工程与临床, 2020,24(6): 672−677. DOI: 10.13339/j.cnki.sglc.20201023.021. ZHAO J H, ZHANG X Q, CHAI J, et al. Analysis of COVID-19 chest CT in asymptomatic infection transferred to diagnosis patients[J]. Biomedical Engineering and Clinical Medicine, 2020, 24(6): 672−677. DOI: 10.13339/j.cnki.sglc.20201023.021. (in Chinese).
[10] 吴杰, 肖安岭, 顾金凤. 多层螺旋CT对新型冠状病毒肺炎的临床诊断价值[J]. 实用放射学杂志, 2021,37(5): 746−748. doi: 10.3969/j.issn.1002-1671.2021.05.013 WU J, XIA0 A L, GU J F. Clinical value of MSCT in the diagnosis of COVID-19[J]. Journal of Practical Radiology, 2021, 37(5): 746−748. (in Chinese). doi: 10.3969/j.issn.1002-1671.2021.05.013
[11] 余成成, 杨彦鸿, 胡天丽, 等. 新型冠状病毒B.1.617.2变异株感染者高分辨率CT与临床特点[J]. 中华放射学杂志, 2021,55(10): 1054−1058. DOI: 10.3760/cma.j.cn112149-20210618-00574. YU C C, YANG Y H, HU T L, et al. High resolution CT findings and clinical features of the novel corona-virus B.1.617.2 variant[J]. Journal of Practical Radiology, 2021, 55(10): 1054−1058. DOI: 10.3760/cma.j.cn112149-20210618-00574. (in Chinese).
[12] 李声鸿, 曾献军, 鄢海蓝, 等. 新型冠状病毒肺炎薄层CT评价[J]. 实用放射学杂志, 2021,37(7): 1074−1076, 1130. DOI: 10.3969/j.issn.1002-1671.2021.07.007. LI S H, ZENG X J, YAN H L, et al. Evaluation of COVID-19 with thin-sclice CT[J]. Journal of Practical Radiology, 2021, 37(7): 1074−1076, 1130. DOI: 10.3969/j.issn.1002-1671.2021.07.007. (in Chinese).
[13] LIGUORO I, PILOTTO C, BONANNI M, et al. SARS-CoV-2 infection in children and newborns: A systematic review[J]. European Journal of Pediatrics, 2020, 179(7): 1029−1046. DOI: 10.1007/s00431-020-03684-7.
[14] 耿梦杰, 任翔, 余建兴, 等. 不同年龄组新型冠状病毒肺炎患者临床特征分析[J]. 疾病监测, 2021,36(6): 573−580. DOI: 10.3784/jbjc.202101220035. GENG M J, REN X, YU J X, et al. Clinical characteristics of coronavirus disease 2019 cases in different age groups[J]. Disease Surveillance, 2021, 36(6): 573−580. DOI: 10.3784/jbjc.202101220035. (in Chinese).
[15] HENRY B M, LIPPI G, PLEBANI M. Laboratory abnormalities in children with novel coronavirus disease 2019[J]. Clinical Chemistry and Laboratory Medicine, 2020, 58(7): 1135−1138. DOI: 10.1515/cclm-2020-0272.
[16] 孙莹, 李玲, 刘晓燕, 等. 早期新型冠状病毒肺炎的胸部薄层平扫CT表现特征[J]. CT理论与应用研究, 2023,32(1): 131−138. DOI: 10.15953/j.ctta.2023.006. SUN Y, LI L, LIU X Y, et al. Imaging features of early COVID-19 on chest thin-slice non-enhanced CT[J]. CT Theory and Applications, 2023, 32(1): 131−138. DOI: 10.15953/j.ctta.2023.006. (in Chinese).
[17] 吴宝亮, 李婷, 侯勤明, 等. 不同年龄组新型冠状病毒肺炎患者首次胸部CT表现[J]. 医学影像学杂志, 2020,30(11): 2034−2037. WU B L, LI T, HOU Q M, et al. Chest CT manifestation of patients with corona virus disease 2019 in different age groups[J]. Journal of Medical Imaging, 2020, 30(11): 2034−2037. (in Chinese).
[18] 李勃, 孙钢. 基础医学视角的新型冠状病毒肺炎CT表现及鉴别诊断[J]. 中国医学影像学杂志, 2020,28(10): 738−740. DOI: 10.3969/j.issn.1005-5185.2020.10.005. LI B, SUN G. CT findings and differential diagnosis of novel coronavirus pneumonia from the perspective of basic medicine[J]. Chinese Journal of Medical Imaging, 2020, 28(10): 738−740. DOI: 10.3969/j.issn.1005-5185.2020.10.005. (in Chinese).
[19] 田斌, 余晖, 任基刚, 等. 基于机器学习的多种分类模型在新型冠状病毒肺炎与社区获得性肺炎鉴别诊断中的效能[J]. 放射学实践, 2021,36(5): 590−595. DOI: 10.13609/j.cnki.1000-0313.2021.05.004. TIAN B, YU H, REN J G, et al. Effectiveness of multiple classification models based on machine learning in the differential diagnosis of COVID-19 and community-acquired pneumonia[J]. Radiologic Practice, 2021, 36(5): 590−595. DOI: 10.13609/j.cnki.1000-0313.2021.05.004. (in Chinese).
[20] 侯阳, 郭启勇. 从SARS、MERS到COVID-19: 以史为鉴−浅谈影像学在冠状病毒肺炎中的应用价值[J]. 中国临床医学影像杂志, 2020,31(2): 77−82. DOI: 10.12117/jccmi.2020.02.001. HOU Y, GUO Q Y. From SARS, MERS to COVID-19: Learning from history: A brief introduction to imaging of coronavirus pneumonia[J]. Journal of China Clinic Medical Imaging, 2020, 31(2): 77−82. DOI: 10.12117/jccmi.2020.02.001. (in Chinese).
[21] CORMAN V M, LANDT O, KAISER M, et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR[J]. Eurosurveillance, 2020, 25(3): 2000045. DOI: 10.2807/1560-7917.ES.2020.25.3.2000045.
[22] LEE N, HUI D, WU A, et al. A major outbreak of severe acute respiratory syndrome in Hongkong[J]. The New England Journal of Medicine, 2003, 348(20): 1986−1994. DOI: 10.1056/NEJMoa030685.
[23] WONG K T, ANTONIO G E, HUI D S, et al. Severe acute respiratory syndrome: Radiographic appearances and pattern of progression in 138 patients[J]. Radiology, 2003, 228(2): 401−406. DOI: 10.1148/radiol.2282030593.
[24] HOSSEINY M, KOORAKI S, GHOLAMREZANEZHAD A, et al. Radiology perspective of coronavirus disease 2019 (COVID-19): Lessonsfrom severe acute respiratory syndrome and middle east respiratory syndrome[J]. American Journal of Roentgenology, 2020, 215(5): 1−5. DOI: 10.2214/AJR.20.22969.
[25] 李蕾. 重症甲型H1N1流感肺部的影像学表现[J]. 中国临床医学影像杂志, 2011,22(2): 118−120. LI L. Pulmonary imaging findings in severe influenza Alpha H1N1[J]. Journal of China Clinic Medical Imaging, 2011, 22(2): 118−120. (in Chinese).
[26] 王青乐, 施裕新, 张志勇, 等. 新型重组禽流感病毒(H7N9)性肺炎的影像学初步观察[J]. 中华放射学杂志, 2013,47(6): 505−508. DOI: 10.3760/cma.j.issn.1005-1201.2013.06.005. WANG Q L, SHI Y X, ZHANG Z Y, et al. Preliminary imaging findings of novel reassortant avian-origin influenza A(H7N9) pneumonia[J]. Chinese Journal of Radiology, 2013, 47(6): 505−508. DOI: 10.3760/cma.j.issn.1005-1201.2013.06.005. (in Chinese).
[27] 陈钊, 王荣福. CT在新型冠状病毒肺炎诊断与鉴别诊断中的应用价值[J]. CT理论与应用研究, 2020,29(3): 273−279. DOI: 10.15953/j.1004-4140.2020.29.03.02. CHEN Z, WANG R F. Application of CT in the diagnosis and differential diagnosis of novel coronavirus pneumonia[J]. CT Theory and Applications, 2020, 29(3): 273−279. DOI: 10.15953/j.1004-4140.2020.29.03.02. (in Chinese).
-
期刊类型引用(1)
1. 吴传洋. 填方土体压实效果多道瞬态瑞雷波快速检测方法. CT理论与应用研究. 2023(06): 703-712 .  本站查看
本站查看
其他类型引用(2)
计量
- 文章访问数: 230
- HTML全文浏览量: 95
- PDF下载量: 20
- 被引次数: 3


