
Risk-Prediction Model Construction of Visceral Pleural Invasion in Early Lung Adenocarcinoma Based on Computed Tomography Imaging Features
-
摘要:
目的:构建基于CT影像特征早期肺腺癌脏层胸膜侵犯风险预测模型。方法:回顾性纳入2016年1月至2022年12月行手术治疗并确诊为IA期肺腺癌患者170例,根据有无脏层胸膜侵犯分为侵犯组(84例)和未侵犯组(86例);采用单因素和多因素法评价早期胸膜下肺腺癌脏层胸膜侵犯CT影像学特征相关独立危险因素,早期胸膜下肺腺癌脏层胸膜侵犯CT影像学特征预测模型效能分析。结果:单因素分析结果显示,实性成分占比、实性成分最大径、桥征、血管集束征及病灶与胸膜毗邻关系均可能与早期胸膜下肺腺癌患者脏层胸膜侵犯有关。多因素分析结果显示,桥征、血管集束征及病灶与胸膜毗邻关系Ⅱ型/Ⅲ 型均是早期胸膜下肺腺癌脏层胸膜侵犯独立危险因素。利用桥征、血管集束征、病灶与胸膜毗邻关系、Logistic模型预测概率对早期胸膜下肺腺癌脏层胸膜侵犯情况预测,最佳截断值分别为0.50、0.50、0.50和56.25%,约登指数分别为24.00%、23.95%、48.70% 和55.04%。结论:基于桥征、血管集束征及病灶与胸膜毗邻关系构建CT影像学特征模型可用于早期胸膜下肺腺癌脏层胸膜侵犯高危人群识别。
Abstract:Objective: To construct a structural risk prediction model for visceral pleural invasion in early lung adenocarcinoma based on computed tomography (CT) features. Methods: 170 patients with early lung adenocarcinoma treated surgically in our hospital were retrospectively selected between January 2016 and December 2022 and grouped according into invasion (84 cases) and non-invasion (86 cases) groups. Independent risk factors related to CT imaging features of visceral pleural invasion in early lung adenocarcinoma were evaluated using univariate and multivariate factor methods. The effectiveness of the CT imaging feature prediction model for visceral pleural invasion in early subpleural lung adenocarcinoma was analyzed. Results: Univariate analysis showed that the proportion and maximum diameter of solid components, bridging sign, vascular bundle sign, and relationship between the lesion and pleura may be related to visceral pleural invasion in patients with early subpleural lung adenocarcinoma. Multivariate analysis showed that the bridging sign, vascular bundle sign, and type II/III relationship between the lesion and pleura were independent risk factors for visceral pleural invasion in early subpleural lung adenocarcinoma. The best cutoff values for predicting visceral pleural invasion in early subpleural lung adenocarcinoma using the bridge sign, vascular bundle sign, adjacent relationship between the lesion and pleura, and logistic model prediction probability were 0.50, 0.50, 0.50, and 56.25%, respectively. The Jordan index for each of these was 24.00%, 23.95%, 48.70%, and 55.04%, respectively. Conclusion: Based on the bridge sign, vascular cluster sign, and the relationship between tumor and pleural adjacency, the CT imaging feature model can be used to identify high-risk groups for visceral pleural invasion in early lung adenocarcinoma.
-
Keywords:
- CT imaging features /
- lung adenocarcinoma /
- visceral pleural invasion /
- prediction
-
常规CT图像实际上是在混合能量X线束的基础上成像,低能X线束易被人体组织吸收,而透过的高能X线束容易产生射线束硬化伪影,现在通常的做法是采用特定的算法对射线束硬化伪影进行校正。但是由于常规CT本身的缺陷,这种校正常常不能充分对其进行抵消,随之产生的非线性伪影会造成疾病的误诊和漏诊[1-2]。同时,由于光电效应和康普顿散射的存在,拥有不同原子序数的物质会呈现出相似的表现,使得CT的密度分辨率不佳[3]。此外,如果采用低电压扫描图像噪声会增加,但图像的对比度分辨率更好。而采用高电压方案则图像的噪声得到抑制,但对比度分辨率进一步下降,且同等情况下的辐射剂量增加。
双能CT利用高低两种能量进行成像,在此基础上通过物质分离算法,重建的虚拟单能图像可以进一步模拟各级能量下不同物质的衰减[4-5]。既往研究表明,双能CT虚拟单能成像相比传统CT可以降低图像噪声,提升图像质量[6-10]。但是,相关研究大多都是临床研究,受限于辐射剂量,不能做到同一个研究对象的自身对照,患者差异会是影响研究结果的潜在重要影响因素。
因此,本研究旨在运用体模,对比双源双能CT低、中、高3档虚拟单能能级图像和两种常规CT图像的图像质量,探讨虚拟单能图像的临床可行性。
1. 资料与方法
1.1 体模
采用CT图像质量控制体模Catphan 500中的高对比度分辨率CTP 528和低对比度分辨率CTP 515两个组间。CTP 528(图1(a))由21组高密度线对(呈放射状分布)的结构,分辨率为1~21 lp/cm。CTP 515(图1(b))由内外两层低密度孔阵(呈放射状分布)的结构构成,内层孔阵的对比度分别为0.3%、0.5%和1.0%,直径分别为3、5、7和9 mm;外层孔阵的对比度分别为0.3%、0.5%和1.0%,直径分别为2、3、4、5、6、7、8、9和15 mm。
1.2 仪器与方法
通过西门子SOMATOM Force双源双能CT分别扫描Catphan 500的CTP 528和CTP 515组件(图1),分别采用双球管双能模式扫描与单球管单能模式扫描。所有扫描方案固定剂量20 mGy,螺距1.0,机架旋转速度为1 s/r。其中双能模式扫描参数为双球管电压对100/150 Sn kVp,电流294 mAs/147 mAs;单能扫描方案采用120 kVp,电流分别为299 mAs和205 mAs。
所有图像重建层厚5 mm,标准滤波函数Qr40(双能模式)或Br40(单能模式)和中等迭代重建算法ADMIRE 2。双能扫描重建3档虚拟单能图像:A组40 keV,B组70 keV,C组100 keV;单能混合能量扫描图像为:D组120 kVp。
1.3 图像质量评估
评估CT图像质量的几个主要参数分别为:高对比度分辨率、低对比度分辨率、图像噪声、信噪比(signal-to-noise ratio,SNR)和对比噪声比(contrast-to-noise ratio,CNR)。
所有图像由两名具有5年以上阅片经验的放射科医生采用独立盲法测量并分别进行主观与客观评价。主观评价记录包含高对比度分辨率组件CTP 528的最佳线对(1~2 lp/cm)以及低对比度分辨率组件CTP 515所能分辨的外层1% 浓度下的最小孔径(直径2~15 mm,要求分辨80% 以上有效面积),比较两名医生的主观评价结果,如有分歧则由另一名高年资医生做最终评判。
客观测量选取两个面积均为100 mm2的圆形感兴趣区域(region of interest,ROI)分别测量CTP 515组件中1% 浓度中直径最大(15 mm)孔径和邻近固态水背景的CT值(CTm和CTw,单位HU),将15 mm孔径ROI标准差(SD)定义为噪声(单位HU),随后计算各组图像SNR=CTm/SD和CNR=(CTm- CTw)/SD。所有主观及客观评价指标均在各组件中心的连续3个层面上进行测量;主观指标取3个层面的最佳值。
1.4 统计学分析
运用SPSS 23.0统计分析软件进行分析。连续性变量数据以
$\bar{x}\pm s $ 表示。两名医生的主观一致性评价采用统计分析Cohen's Kappa检验,客观一致性评价采用Spearman相关性分析。5组图像的高对比度分辨率和低对比度分辨率采用秩和检验;5组图像的SD、SNR及CNR的比较采用单因素方差分析。双能模式虚拟能级图像的组内比较采用Bonferroni矫正,以P<0.05认为差异具有统计学意义。
2. 结果
2.1 一致性评价
两名医生对各组图像的高对比度分辨率和低对比度分辨率的主观及客观一致性评价良好,Kappa系数为0.667,Spearman相关系数r=0.920,差异均具有统计学意义。
2.2 四组图像对比度分辨率比较
D组图像具有最佳的高对比度分辨率(线对6 lp/cm),A组~C组图像的最佳线对数均为5 lp/cm。对于低对比度分辨率,A组和B组图像表现最佳(均为4 mm孔径),其余两组图像的最小孔径为5 mm(表1)。3档虚拟单能图像对比见图2。
表 1 四组图像高对比度分辨率和低对比度分辨率比较Table 1. Comparison of high-contrast resolution and low-contrast resolution of four groups of images对比度分辨率 A组
(40 keV)B组
(70 keV)C组
(100 keV)D组
(120 kVp)高对比对分辨率(线对/(lp/cm)) 5 5 5 6 低对比度分辨率(孔径直径/mm) 4 4 5 5 ![]() 图 2 三档虚拟单能图像的示例图(a)~(c)分别代表40、70和100 keV图像;(a1)、(b1)和(c1)分别代表相同窗宽窗位下(400,0)40、70和100 keV的图像对比;(a2)和(a3)、(b2)和(b3)、(c2)和(c3)分别代表相应虚拟单能图像的CTP 515低对比度分辨率和CTP 528高对比度分辨率模块图像。Figure 2. Schematic diagram for the three series of virtual monochromatic images
图 2 三档虚拟单能图像的示例图(a)~(c)分别代表40、70和100 keV图像;(a1)、(b1)和(c1)分别代表相同窗宽窗位下(400,0)40、70和100 keV的图像对比;(a2)和(a3)、(b2)和(b3)、(c2)和(c3)分别代表相应虚拟单能图像的CTP 515低对比度分辨率和CTP 528高对比度分辨率模块图像。Figure 2. Schematic diagram for the three series of virtual monochromatic images2.3 四组图像噪声、SNR和CNR比较
各组图像间噪声差异有统计学意义,其中A组图像噪声最大(4.167±0.289),C组图像噪声最小(2.333±0.289);噪声在虚拟单能组内(A组~C组)差异有统计学意义。各组图像间SNR差异有统计学意义,C组图像SNR最高(37.944±3.949);SNR随着虚拟单能能级的升高而增加,SNR在虚拟单能组内(A组~C组)间差异有统计学意义。B组图像的CNR最高(3.361±0.875),但各组图像CNR差异无统计学意义;组内比较方面,虚拟单能组(A组~C组)的CNR差异也无统计学意义(表2)。
表 2 四组图像图噪声参数评价结果比较Table 2. Comparison of the evaluation results of the noise parameters of the five groups of images组别 SD/HU SNR CNR A组(40 keV) 4.167±0.289 10.942±0.465 2.383±0.336 B组(70 keV) 2.500±0.500 24.028±5.000 3.361±0.875 C组(100 keV) 2.333±0.289 37.944±3.949 3.139±0.337 D组(120 kVp) 2.500±0.000 30.806±1.398 2.778±0.241 $P $ <0.001 <0.001 0.179 3. 讨论
CT在临床诊疗中扮演着重要的作用,但常规CT在选择最优管电压方面具有一定的妥协性。选择低电压代表更低的辐射剂量,虽然其具有更高的图像对比度,在常规低剂量肺筛的作用显著,但是也在一定程度上牺牲了图像质量,增加了图像噪声,因此在其他领域的作用受限;而选择高电压方案则与此相反,虽能获得更佳的图像质量,但其图像对比度下降且会增加病人的受照辐射剂量。
由于常规CT扫描采用的是混合能量X射线谱,以120 kVp为例,低能的X射线被组织吸收,导致其平均能量大约在90 keV左右,在这种能量下,钙与碘具有相似的衰减系数,因此两种物质在常规CT上具有相似的高密度,这不利于钙化斑块的检出[11]。双能CT在不增加患者辐射剂量的基础上,可以重建不同虚拟单能能级的图像,利用不同物质/组织在不同X线束下的衰减系数不同,以此获得不同对比度的CT图像,并且可以通过“动态”观察不同物质随着能级变化的特点,实现常规CT上不能实现的微小病灶的检出和病灶成分的鉴别。目前有研究证明其在心血管疾病、肿瘤检出、颅内出血、炎症性肠病等领域的效果显著[12-16]。
本研究分别研究低、中、高3档虚拟单能能级图像的图像质量,3档能级图像具有相似的高/低对比度分辨率,100 keV低对比度分辨率稍有下降。既往研究表明,低keV下图像的低对比度分辨率(即密度分辨率)较高,图像对不同软组织的分辨较好,但是同时伴随着一定的伪影,而高keV下图像的伪影得到抑制,但图像的密度分辨率下降。因此,低keV虚拟单能图像有助于CT静脉造影及软组织肿块等的检出,而高keV则有助于抑制如心脏支架、人工髋关节伪影等对图像质量的影响[4,11]。
图像噪声方面,随着能级的增加,图像平均噪声降低,而70 keV的CNR更高,100 keV的SNR最高。总体来看,本体模研究表明,70 keV是比较均衡的虚拟单能能级;不同研究也表明,70 keV有助于冠状动脉、肺血管、胰腺癌、小肠梗阻等的显示或检出[17-20]。目前最常用的3档双能成像模式(双源双能量、快速kVp切换以及双层探测器模式),与常规120 kVp图像等效的虚拟单能图像的能级均在70 keV左右。同等条件下,70 keV图像往往具有更低的辐射剂量,更佳的图像质量。本研究中,70 keV图像的平均噪声比常规120 kVp图像更低,而CNR更高,两者的高/低对比度分辨率相近,提示70 keV图像具有更高的图像质量,这与前人的研究结果相一致[21-22]。
本研究也存在一定的局限性。①本研究只对比了低、中、高3档虚拟单能能级,在全面对比虚拟单能图像之间的差异方面还显不足;②本研究用的体模为研究对象,且只选取了其中两个模块进行评价,对图像质量的全面评价略显不足,例如对比虚拟单能图像和常规CT图像的CT值准确性等方面还有待进一步研究;③本模型研究在临床方面的指导作用还有待进一步阐明。
总之,能谱CT虚拟单能图像相比传统混合能量CT图像可以降低图像噪声并提升图像质量。
-
![]()
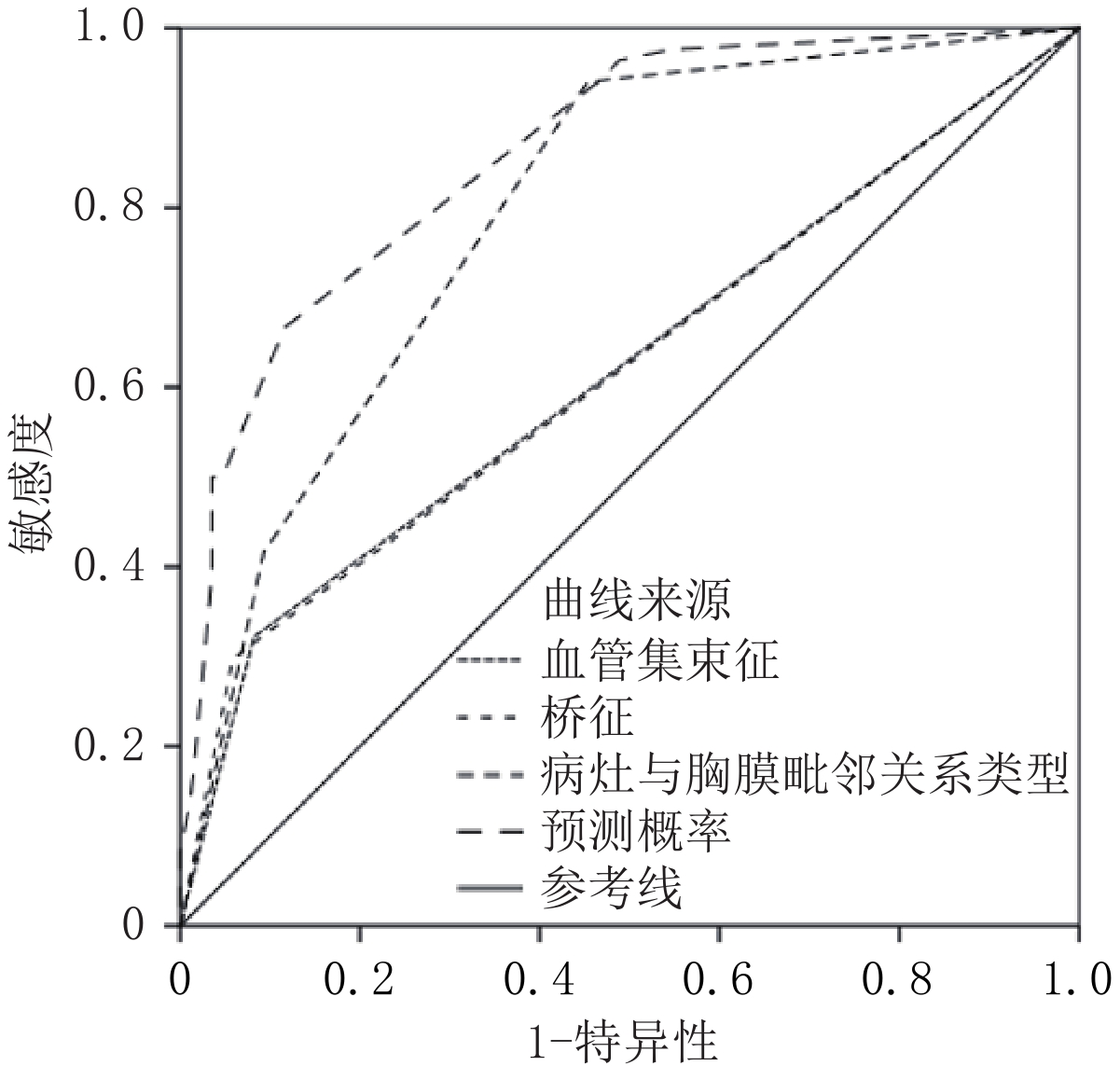
图 1 早期胸膜下肺腺癌脏层胸膜侵犯CT影像学特征预测ROC曲线
Figure 1. ROC curve predicted by CT imaging features of visceral pleural invasion in early subpleural lung adenocarcinoma
![]()
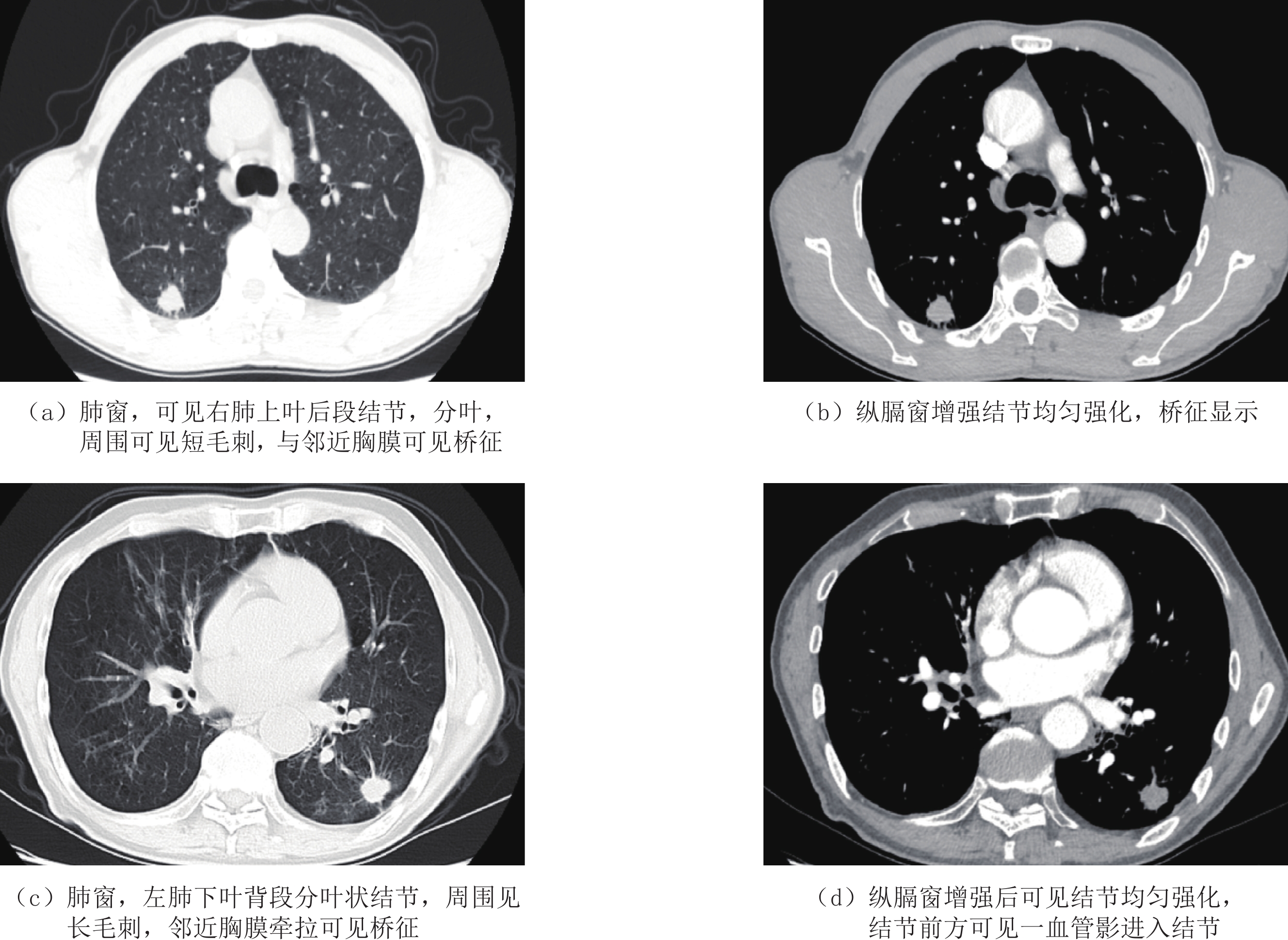
图 2 早期肺腺癌脏层胸膜侵犯典型图像
Figure 2. Typical images of visceral pleural invasion in early-stage lung adenocarcinoma
表 1 早期胸膜下肺腺癌脏层胸膜侵犯CT影像学特征相关危险因素单因素分析
Table 1 Univariate analysis of risk factors associated with CT imaging features of visceral pleural invasion in early subpleural lung adenocarcinoma
指标 组别 统计检验 未侵犯组(n=86) 侵犯组(n=84) $t/\chi^2 $ P 年龄/岁 60.54±7.30 61.31±7.86 -0.909 0.365 男/女/例 30/56 33/51 0.353 0.552 病灶位置 0.189 0.664 左肺 26(30.23) 28(33.33) 右肺 60(69.77) 56(66.67) CT影像学指标 病灶最大径/mm 24.54±4.40 25.36±4.63 -1.643 0.102 病灶与胸膜间最短距离/mm 3.01±0.54 2.95±0.50 1.113 0.267 实性成分最大径/mm 12.83±2.40 14.79±3.12 -5.826 0.000 实性成分比例(%) 53.41±4.10 57.01±6.14 -5.438 0.000 病灶密度类型/例 0.538 0.463 亚实性 76(88.37) 71(84.52) 实性 10(11.63) 13(15.48) 病灶形状/例 1.754 0.185 圆/类圆形 68(79.07) 59(70.24) 不规则 18(20.93) 25(29.76) 分叶征/例 85(98.84) 77(91.67) 3.404◆ 0.065 毛刺征/例 13(15.12) 20(23.81) 2.053 0.152 边界模糊/例 2(2.33) 4(4.76) 0.198◆ 0.656 内部结构/例 空泡 24(27.91) 27(32.14) 0.363 0.547 囊腔/空洞 4(4.65) 5(5.95) 0.001◆ 0.971 毗邻结构/例 支气管改变 54(62.79) 46(54.76) 1.131 0.288 血管集束征 7(8.14) 27(32.14) 15.302 0.000 桥征/例 5(5.81) 21(25.00) 12.074 0.001 病灶与胸膜毗邻关系类型/例 53.114 0.000 Ⅰ型 47(54.65) 5(5.95) Ⅱ型 31(36.05) 44(52.38) Ⅲ 型 8(9.30) 35(41.67) 注:◆为连续校正$\chi^2 $检验。  下载: 导出CSV
下载: 导出CSV
表 2 早期胸膜下肺腺癌脏层胸膜侵犯CT影像学特征相关危险因素多因素分析
Table 2 Multivariate analysis of the risk factors related to CT imaging features of visceral pleural invasion in early subpleural lung adenocarcinoma
影响因素 β SE Wald $\chi^2 $ OR值 OR 95% CI P 实性成分最大径 -0.001 0.074 0.000 0.999 0.864~1.154 0.987 实性成分比例 -0.043 0.041 1.100 0.958 0.884~1.038 0.294 血管集束征 2.074 0.653 10.087 7.954 2.212~28.601 0.001 桥征 2.162 0.668 10.469 8.687 2.345~32.184 0.001 病灶与胸膜毗邻关系类型 30.805 <0.001 Ⅱ型 2.987 0.620 23.236 19.832 5.886~66.815 <0.001 Ⅲ 型 3.742 0.696 28.930 42.170 10.786~164.873 <0.001 常量 -0.830 2.343 0.125 0.436 0.723
下载: 导出CSV
表 3 早期胸膜下肺腺癌脏层胸膜侵犯CT影像学特征预测价值
Table 3 Predictive value of CT imaging features of visceral pleural invasion in early subpleural lung adenocarcinoma
项目 最佳截断值 ROC曲线下面积 诊断灵敏度/% 诊断特异度/% 约登指数/% 血管集束征 0.50 0.620 32.14 91.86 24.00 桥征 0.50 0.620 29.76 94.19 23.95 病灶与胸膜毗邻关系类型 0.50 0.794 94.05 54.65 48.70 Logistic模型预测概率 56.25% 0.861 66.67 88.37 55.04
下载: 导出CSV
表 4 ROC曲线下的成对样本区域差异
Table 4 Regional differences in paired samples under the ROC curve
检验结果对 统计检验 Z P 血管集束征-桥征 0.007 0.995 血管集束征-病灶与胸膜毗邻关系类型 -4.189 0.000 血管集束征-Logistic模型预测概率 -7.194 0.000 桥征-病灶与胸膜毗邻关系类型 -4.155 0.000 桥征-Logistic模型预测概率 -7.694 0.000 病灶与胸膜毗邻关系类型-Logistic模型预测概率 -3.649 0.000
下载: 导出CSV
-
[1] SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA: A Cancer Journal for Clinicians, 2021, 71(3): 209−249. DOI: 10.3322/caac.21660.
[2] CHOI H, KIM H, HONG W, et al. Prediction of visceral pleural invasion in lung cancer on CT: Deep learning model achieves a radiologist-level performance with adaptive sensitivity and specificity to clinical needs[J]. European Journal of Radiology, 2021, 31(5): 2866−2876. DOI: 10.1007/s00330-020-07431-2.
[3] ZHANG T, ZHANG J T, LI W F, et al. Visceral pleural invasion in T1 tumors (≤3 cm), particularly T1a, in the eighth tumor-node-metastasis classification system for non-small cell lung cancer: A population-based study[J]. Journal of Thoracic Disease, 2019, 11(7): 2754−2762. DOI: 10.21037/jtd.2019.06.32.
[4] WO Y, ZHAO Y, QIU T, et al. Impact of visceral pleural invasion on the association of extent of lymphadenectomy and survival in stage I non-small cell lung cance[J]. Cancer Medicine, 2019, 8(2): 669−678. DOI: 10.1002/cam4.1990.
[5] ZUO Z, LI Y, PENG K, et al. CT texture analysis-based nomogram for the preoperative prediction of visceral pleural invasion in cT1N0M0 lung adenocarcinoma: An external validation cohort study[J]. Clinical Radiology, 2022, 77(3): e215−e221. DOI: 10.1016/j.crad.2021.11.008.
[6] YUAN M, LIU J Y, ZHANG T, et al. Prognostic impact of the findings on thinsection computed tomography in stage I lung adenocarcinoma with visceral pleural invasion[J]. Scientific Reports, 2018, 8(1): 1−9.
[7] ONODA H, HIGASHI M, MURAKAMI T, et al. Correlation between pleural tags on CT and visceral pleural invasion of peripheral lung cancer that does not appear touching the pleural surface[J]. European Journal of Radiology, 2021, 31(12): 9022−9029. DOI: 10.1007/s00330-021-07869-y.
[8] WEI S H, ZHANG J M, SHI B, et al. The value of CT radiomics features to predict visceral pleural invasion in ≤3 cm peripheral type early non-small cell lung cancer[J]. Journal of X-ray Science and Technology, 2022, 30(6): 1115−1126. DOI: 10.3233/XST-221220.
[9] ZHANG Y, KWON W, LEE H Y, et al. Imaging assessment of visceral pleural surface invasion by lung cancer: Comparison of CT and contrast-enhanced radial T1-weighted gradient echo 3-Tesla MRI[J]. Korean Journal of Radiology, 2021, 22(5): 829−839. DOI: 10.3348/kjr.2020.0955.
[10] SHI J, LI F, YANG F, et al. The combination of computed tomography features and circulating tumor cells increases the surgical prediction of visceral pleural invasion in clinical T1N0M0 lung adenocarcinoma[J]. Translational Lung Cancer Research, 2021, 10(11): 4266−4280. DOI: 10.21037/tlcr-21-896.
[11] TU Z, LI C, TIAN T, et al. A risk classification system predicting the cancer-specific survival for postoperative stage IB non-small-cell lung cancer patients without lymphovascular and visceral pleural invasion[J]. Lung Cancer, 2021, 161(11): 114−121.
[12] YANG X, SUN F, CHEN L, et al. Prognostic value of visceral pleural invasion in non-small cell lung cancer: A propensity score matching study based on the SEER registry[J]. Journal Surgery Oncology, 2017, 116(3): 398−406. DOI: 10.1002/jso.24677.
[13] YU Y, HUANG R, WANG P, et al. Sublobectomy versus lobectomy for long-term survival outcomes of early-stage non-small cell lung cancer with a tumor size ≤2 cm accompanied by visceral pleural invasion: A SEER population-based study[J]. Journal of Thoracic Disease, 2020, 12(3): 592−604. DOI: 10.21037/jtd.2019.12.121.
[14] NAM J G, PARK S, PARK C M, et al. Histopathologic basis for a chest CT deep learning survival prediction model in patients with lung adenocarcinoma[J]. Radiology, 2022, 305(2): 441−451. DOI: 10.1148/radiol.213262.
[15] 汤敏, 孙丹丹, 尹柯, 等. 胸膜下肺腺癌脏层胸膜侵犯CT及临床风险因素[J]. 放射学实践, 2020, 35(10): 1243−1248. TANG M, SUN D D, YIN K, et al. CT and clinical risk factors of visceral pleural invasion in subpleural lung adenocarcinoma[J]. Radiology Practice, 2020, 35(10): 1243−1248. (in Chinese).
[16] YANG S, YANG L, TENG L, et al. Visceral pleural invasion by pulmonary adenocarcinoma ≤3 cm: The pathological correlation with pleural signs on computed tomography[J]. Journal of Thoracic Disease, 2018, 10(7): 3992−3999. DOI: 10.21037/jtd.2018.06.125.
[17] WANG F, LI P, LI F. Nomogram for predicting the relationship between the extent of visceral pleural invasion and survival in non-small-cell lung cancer[J]. Canadian Respiratory Journal, 2021, 20(7): 8816860.
[18] WANG Y, LYU D, ZHOU T, et al. Multivariate analysis based on the maximum standard unit value of 18F-fluorodeoxyglucose positron emission tomography/computed tomography and computed tomography features for preoperative predicting of visceral pleural invasion in patients with subpleural clinical stage IA peripheral lung adenocarcinoma[J]. Diagnostic and Interventional Radiology, 2023, 29(2): 379−389. DOI: 10.4274/dir.2023.222006.
[19] KIM H J, CHO J Y, LEE Y J, et al. Clinical significance of pleural attachment and indentation of subsolid nodule lung cancer[J]. Cancer Research and Treatment, 2019, 51(4): 1540−1548. DOI: 10.4143/crt.2019.057.
[20] HEIDINGER B H, SCHWARZ-NEMEC U, ANDERSON K R, et al. Visceral pleural invasion in pulmonary adenocarcinoma: Differences in CT patterns between solid and subsolid cancers[J]. Radiology-Cardiothoracic Imaging, 2019, 1(3): e190071. DOI: 10.1148/ryct.2019190071.
-
期刊类型引用(3)
1. 刘海燕,邱晓晖,章辉庆,锁咏梅,王超,王亚丽. 能谱CT单能量成像对结直肠癌供血动脉图像质量及辐射剂量的影响. 中国CT和MRI杂志. 2025(01): 159-161 .  百度学术
百度学术
2. 叶雄鑫,刘元芬,汤博荣,陈依林,郑莞怡,薛莉薇,张孝勇. 深度学习图像重建和能谱成像在低对比剂流速胸主动脉CTA中的价值. CT理论与应用研究. 2024(06): 683-691 . 本站查看
3. 何亮,唐彩银,张继,田为中,朱鹏飞. 能谱CT金属伪影抑制算法在胸部穿刺活检中的应用价值. 中国CT和MRI杂志. 2023(11): 50-52 . 百度学术
其他类型引用(2)



计量
- 文章访问数: 149
- HTML全文浏览量: 33
- PDF下载量: 24
- 被引次数: 5
