
The Value of Radiomics Based on Spectral CT Iodine Map for Diagnosing Cervical Lymph Node Metastasis in Papillary Thyroid Carcinoma
-
摘要:
目的:探讨基于能谱CT碘图的影像组学特征对甲状腺乳头状癌患者颈部转移性淋巴结的诊断价值。方法:收集术前两周行颈部能谱CT检查的甲状腺乳头状癌患者,共纳入117枚转移性和176枚非转移性淋巴结,按照3︰1的比例随机分为训练集和验证集。从静脉期碘图中提取并筛选淋巴结的影像组学特征。采用Logistic回归分别建立影像组学模型、常规CT图像特征模型及联合模型,并绘制列线图将联合模型可视化。各模型的诊断效能、校准能力及临床实用性分别通过ROC曲线、校准曲线及决策曲线分析评估。结果:联合模型在训练集和验证集中均表现出最佳的诊断效能,其次是影像组学模型,且两者显著优于常规CT图像特征模型。所有模型均显示出良好的校准能力,决策曲线分析表明列线图的临床实用性优于其余两种模型。结论:能谱CT的影像组学特征在诊断甲状腺乳头状癌淋巴结转移方面表现出良好的性能,联合常规CT图像特征后诊断效能进一步提高。
Abstract:Objective: To investigate the value of radiomics features based on spectral CT iodine map for diagnosing metastatic cervical lymph nodes in patients with papillary thyroid carcinoma. Methods: Seventy-eight patients with papillary thyroid carcinoma who underwent cervical energy spectrum CT within two weeks before surgery were retrospectively analyzed. We included 117 metastatic, 176 non-metastatic lymph nodes, which were then randomly divided into a training set and a validation set in a 3:1 ratio. Radiomics features were extracted and screened from venous phase iodine maps. Logistic regression model was used to construct diagnostic models based on CT image features, radiomics signature, and a combination of the two, respectively; a nomogram was then drawn to visualize the combined model. The diagnostic performance, calibration ability and clinical practicability of each model were evaluated by ROC curve, calibration curve and decision curve analysis, respectively. Results: The combined model showed optimal diagnostic performance in both the training and validation sets, followed by radiomics model. These two models outperformed the CT image features model in both the training and validation sets. All models showed good calibration, and decision curve analysis demonstrated the superiority of the nomogram over the other two models in terms of clinical usefulness. Conclusion: The radiomics signature of spectral CT showed good performance in diagnosing lymph node metastasis of papillary thyroid carcinoma. The diagnostic performance was further improved when combined with CT image features, which can be a useful tool to assist in clinical decision-making.
-
Keywords:
- spectral CT /
- radiomics /
- thyroid neoplasms /
- papillary carcinoma /
- lymphatic metastasis
-
-
![]()
图 2 甲状腺乳头状癌患者伴颈部转移性淋巴结(红色箭头)
Figure 2. A papillary thyroid cancer patient with metastatic cervical lymph nodes (red arrow)
![]()
图 3 联合常规CT图像特征(形状、强化程度、强化方式及钙化)和Radscore绘制的列线图,用于判断转移性淋巴结的风险
Figure 3. Nomogram combined with conventional CT image features (shape, degree of enhancement, enhancement pattern, and calcification) and Radscore was used to determine the risk of metastatic lymph nodes
![]()
图 4 CT图像特征模型、影像组学模型、列线图诊断甲状腺乳头状癌颈部转移淋巴结的ROC曲线
注:(a)为训练集,(b)为验证集。可见列线图的曲线下面积大于另外两种模型。
Figure 4. ROC curve of the CT image feature model, radiomics model and nomogram in diagnosing cervical lymph node metastasis of papillary thyroid carcinoma
![]()
图 5 训练集(a)~(c)和验证集(d)~(f)中CT图像特征模型、影像组学模型和列线图的校准曲线,曲线越接近对角灰色虚线表示模型的预测能力越好
Figure 5. The calibration curves of the CT image feature model, radiomics model, and nomogram in the training set ((a)~(c)) and validation set ((d)~(f)). The closer the curve is to the diagonal gray dotted line, the better the predictive ability of the model
![]()
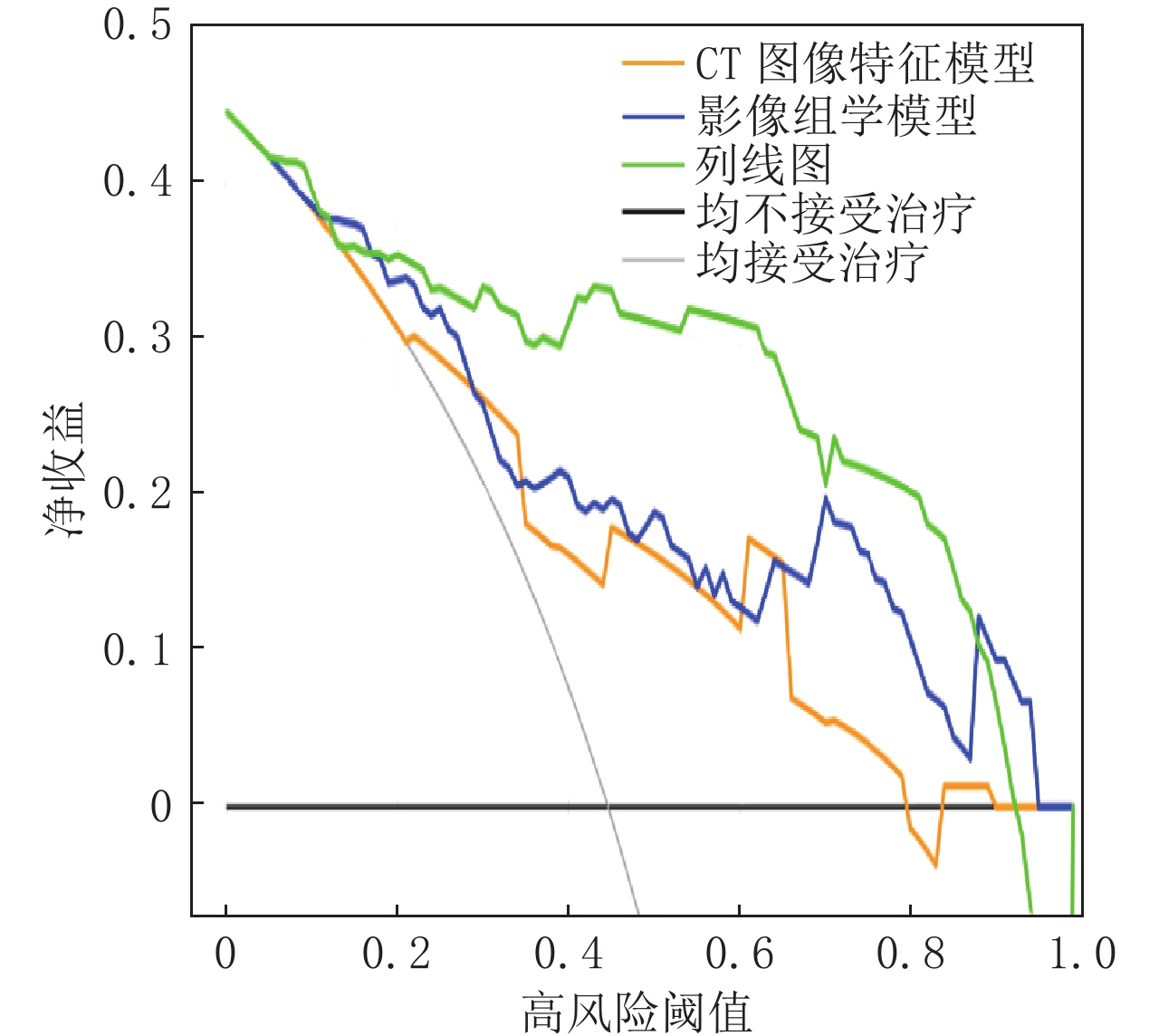
图 6 CT图像特征模型、影像组学模型和列线图的决策曲线
注:曲线显示预测淋巴结转移的阈值概率在19%~88% 时,列线图比CT图像特征模型和影像组学模型获得更多的净收益。
Figure 6. Decision curve analysis of the CT image feature model, radiomics model and nomogram
表 1 甲状腺乳头状癌患者颈部转移组与非转移组淋巴结的CT图像特征比较
Table 1 Comparison of CT image features of neck lymph nodes between metastatic and non-metastatic groups of patients with papillary thyroid carcinoma
组别 数量/枚 最大短径d/mm 形状 边缘 强化程度 5≤d<10 10≤d<35 规则 不规则 清楚 模糊 轻中度 明显 转移组 117 85 32 69 48 80 37 41 76 非转移组 176 134 42 144 32 142 34 115 61 统计检验 $\chi^2 $ 0.453 18.477 5.797 25.915 P 0.501 <0.001 <0.050 <0.001 组别 数量/枚 强化方式 钙化 囊变/坏死 结外侵犯 均匀 不均匀 有 无 有 无 有 无 转移组 117 54 63 14 103 16 101 8 109 非转移组 176 139 37 3 173 1 175 0 176 统计检验 $\chi^2 $ 33.680 13.540 22.091 Fisher P <0.001 <0.001 <0.001 <0.001 注:本研究中所测得淋巴结最大短径范围为5~35 mm。  下载: 导出CSV
下载: 导出CSV
表 2 三种模型诊断甲状腺乳头状癌颈部淋巴结转移纳入的logistic回归因素
Table 2 Logistic regression factors included in the diagnosis of cervical lymph node metastasis of papillary thyroid carcinoma by three models
模型 变量 P 回归系数 标准差 Wald值 OR值 95% CI CT图像特征模型 形状 0.013 0.746 0.302 6.113 2.108 1.167~3.806 强化程度 0.000 1.007 0.270 13.938 2.737 1.613~4.643 强化方式 <0.001 1.148 0.280 16.834 3.153 1.821~5.456 钙化 0.035 1.480 0.700 4.469 4.394 1.113~17.335 影像组学模型 firstorder_90 Percentile
_wavelet_HLH0.000 -0.994 0.273 13.281 0.370 0.216~0.631 glcm_Correlation_wavelet_LHL <0.001 -1.143 0.280 16.695 0.319 0.184~0.551 glcm_Idm_wavelet_HLH 0.518 -0.155 0.239 0.418 0.857 0.535~1.369 glcm_Imc1_wavelet_LHL 0.036 -0.638 0.305 4.388 0.528 0.290~0.959 gldm_DependenceVariance
_log_sigma_3_0_mm_3D0.094 0.335 0.200 2.812 1.398 0.945~2.068 gldm_Dependence
Variance_wavelet_HHH0.055 0.404 0.211 3.673 1.497 0.990~2.262 glrlm_GrayLevelNon
UniformityNormalized_square0.118 -0.623 0.399 2.441 0.537 0.245~1.171 glrlm_LowGrayLevel
RunEmphasis_square0.689 -0.146 0.364 0.161 0.864 0.423~1.763 shape_Elongation_original 0.005 0.525 0.187 7.889 1.690 1.171~2.436 联合模型 形状 0.000 1.408 0.384 13.465 4.086 1.926~8.666 强化程度 0.012 0.817 0.326 6.303 2.265 1.196~4.286 强化方式 0.016 0.820 0.341 5.788 2.270 1.164~4.426 钙化 0.061 1.434 0.765 3.509 4.195 0.935~18.805 Radscore <0.001 5.486 0.731 56.269 241.193 57.528~1011.227
下载: 导出CSV
表 3 训练集和验证集中CT图像特征模型、影像组学模型和列线图的诊断效能比较
Table 3 Comparison of diagnostic performance of the CT image feature model, radiomics model, and nomogram in training and validation sets
数据集 模型 AUC 95%CI P 灵敏度 特异度 PPV NPV 训练集 CT图像特征模型 0.746 0.682~0.802 <0.001 0.595 0.815 0.667 0.764 影像组学模型 0.832 0.776~0.879 0.061 0.857 0.689 0.632 0.886 列线图 0.870 0.818~0.912 ref 0.679 0.926 0.851 0.822 验证集 CT图像特征模型 0.751 0.637~0.844 0.005 0.576 0.902 0.826 0.725 影像组学模型 0.816 0.709~0.897 0.051 0.909 0.561 0.625 0.885 列线图 0.899 0.807~0.957 ref 0.788 0.927 0.900 0.864
下载: 导出CSV
-
[1] MCLEOD D S, SAWKA A M, COOPER D S. Controversies in primary treatment of low-risk papillary thyroid cancer[J]. Lancet, 2013, 381(9871): 1046−1057. DOI: 10.1016/S0140-6736(12)62205-3.
[2] PARK J H, YOON J H. Lobectomy in patients with differentiated thyroid cancer: Indications and follow-up[J]. Endocrine-Related Cancer, 2019, 26(7): R381−R393. DOI: 10.1530/ERC-19-0085.
[3] CHOI J S, KIM J, KWAK J Y, et al. Preoperative staging of papillary thyroid carcinoma: Comparison of ultrasound imaging and CT[J]. American Journal of Roentgenology, 2009, 193(3): 871−878. DOI: 10.2214/AJR.09.2386.
[4] ROH J L, PARK J Y, KIM J M, et al. Use of preoperative ultrasonography as guidance for neck dissection in patients with papillary thyroid carcinoma[J]. Journal of Surgical Oncology, 2009, 99(1): 28−31. DOI: 10.1002/jso.21164.
[5] KIM E, PARK J S, SON K R, et al. Preoperative diagnosis of cervical metastatic lymph nodes in papillary thyroid carcinoma: Comparison of ultrasound, computed tomography, and combined ultrasound with computed tomography[J]. Thyroid, 2008, 18(4): 411−418. DOI: 10.1089/thy.2007.0269.
[6] LAMBIN P, LEIJENAAR R T, DEIST T M, et al. Radiomics: The bridge between medical imaging and personalized medicine[J]. Nature Reviews Clinical Oncology, 2017, 14(12): 749−762. DOI: 10.1038/nrclinonc.2017.141.
[7] GILLIES R J, KINAHAN P E, HRICAK H. Radiomics: Images are more than pictures, they are data[J]. Radiology, 2016, 278(2): 563−577. DOI: 10.1148/radiol.2015151169.
[8] ZHOU Y, SU G Y, HU H, et al. Radiomics analysis of dual-energy CT-derived iodine maps for diagnosing metastatic cervical lymph nodes in patients with papillary thyroid cancer[J]. European Radiology, 2020, 30(11): 6251−6262. DOI: 10.1007/s00330-020-06866-x.
[9] SCOTT G C, MEIER D A, DICKINSON C Z. Cervical lymph node metastasis of thyroid papillary carcinoma imaged with fluorine-18-FDG, technetium-99m-pertechnetate and iodine-131-sodium iodide[J]. Journal of Nuclear Medicine, 1995, 36(10): 1843−1845.
[10] CHOI B, KIM D H, SON S H, et al. Usefulness of SPECT/CT for equivocal findings on I-131 whole-body scan in a patient with differentiated papillary thyroid cancer[J]. Clinical Nuclear Medicine, 2014, 39(2): E160−E2. DOI: 10.1097/RLU.0b013e318286b9bb.
[11] 中国医师协会外科医师分会甲状腺外科医师委员会, 中国研究型医院学会甲状腺疾病专业委员会. 分化型甲状腺癌颈侧区淋巴结清扫专家共识(2017版)[J]. 中国实用外科杂志, 2017, 37(9): 985−991. DOI: 10.19538/j.cjps.issn1005-2208.2017.09.13. [12] PARK J E, LEE J H, RYU K H, et al. Improved diagnostic accuracy using arterial phase CT for lateral cervical lymph node metastasis from papillary thyroid cancer[J]. American Journal of Neuroradiology, 2017, 38(4): 782−788. DOI: 10.3174/ajnr.A5054.
[13] 许晓泉, 周燕, 苏国义, 等. 联合CT图像特征和双能CT定量参数对甲状腺乳头状癌颈部淋巴结转移的诊断价值[J]. 中华放射学杂志, 2021, 55(2): 137−142. DOI: 10.3760/cma.j.cn112149-20200222-00226. XU X Q, ZHOU Y, SU G Y, et al. Integrating CT image features and quantitative dual-energy CT parameters for diagnosing metastatic lymph nodes from papillary thyroid carcinoma[J]. Chinese Journal of Radiology, 2021, 55(2): 137−142. DOI: 10.3760/cma.j.cn112149-20200222-00226. (in Chinese).
[14] 中华医学会放射学分会头颈学组. 甲状腺结节影像检查流程专家共识[J]. 中华放射学杂志, 2016, 50(12): 911−915. DOI: 10.3760/cma.j.issn.1005-1201.2016.12.003. [15] 魏培英, 蒋念东, 韩志江, 等. CT强化程度对甲状腺乳头状癌颈部淋巴结转移的诊断价值[J]. 中华内分泌外科杂志, 2020, 14(2): 144−148. WEI P Y, JIANG N D, HAN Z J, et al. Value of CT enhancement degree in diagnosing cervical lymph node metastasis of papillary thyroid carcinoma[J]. Chinese Journal of Endocrine Surgery, 2020, 14(2): 144−148. (in Chinese).
[16] KING A D, TSE G M, YUEN E H. et al. Comparison of CT and MR imaging for the detection of extranodal neoplastic spread in metastatic neck nodes[J]. European Journal of Radiology, 2004, 52(3): 264−270. DOI: 10.1016/j.ejrad.2004.03.004.
[17] CHAI R L, RATH T J, JOHNSON J T, et al. Accuracy of computed tomography in the prediction of extracapsular spread of lymph node metastases in squamous cell carcinoma of the head and neck[J]. Jama Otolaryngology-Head & Neck Surgery, 2013, 139(11): 1187−1194.
[18] HUGHES D T, HAYMART M R, MILLER B S, et al. The most commonly occurring papillary thyroid cancer in the united states is now a microcarcinoma in a patient older than 45 years[J]. Thyroid, 2011, 21(3): 231−236. DOI: 10.1089/thy.2010.0137.
[19] WANG T S, DUBNER S, SZNYTER L A, et al. Incidence of metastatic well-differentiated thyroid cancer in cervical lymph nodes[J]. Archives of Otolaryngology-Head & Neck Surgery, 2004, 130(1): 110−113.
[20] 陈雨桐, 王燕. 超声诊断甲状腺乳头状癌颈部转移淋巴结的研究进展[J]. 肿瘤影像学, 2022, 31(2): 203−207. CHEN Y T, WANG Y. Advances in ultrasonographic diagnosis of cervical lymph node metastasis in papillary carcinoma of the thyroid[J]. Oncoradiology, 2022, 31(2): 203−207. (in Chinese).
[21] HAUGEN B R, ALEXANDER E K, BIBLE K C, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer[J]. Thyroid, 2016, 26(1): 1−133. DOI: 10.1089/thy.2015.0020.
[22] LIU Z M, XUN X Q, WANG Y Z, et al. MRI and ultrasonography detection of cervical lymph node metastases in differentiated thyroid carcinoma before reoperation[J]. American Journal of Translational Research, 2014, 6(2): 147−154.
[23] 周燕, 许晓泉, 苏国义, 等. 双能CT动静脉期加权融合图像影像组学对甲状腺乳头状癌颈部淋巴结转移的诊断价值[J]. 中华放射学杂志, 2021, 55(7): 703−709. ZHOU Y, XU X Q, SU G Y, et al. Radiomics based on arterial-venous mixed images derived from dual-energy CT data in diagnosis of lymph nodes metastasis of papillary thyroid cancer[J]. Chinese Journal of Radiology, 2021, 55(7): 703−709. (in Chinese).
-
期刊类型引用(3)
1. 席杭闽. 上海市某医院CT机房屏蔽防护改造及评价. 价值工程. 2022(25): 51-53 .  百度学术
百度学术
2. 黄贤海,李桂明,劳婉仪. 平疫结合的CT机房建设实践. 现代仪器与医疗. 2022(04): 91-96 . 百度学术
3. 周大琼,谢震中,何李. 智慧医疗系列产品在新冠肺炎疫情中的应用. 人工智能. 2021(03): 92-100 . 百度学术
其他类型引用(0)





计量
- 文章访问数: 152
- HTML全文浏览量: 24
- PDF下载量: 30
- 被引次数: 3


