
Advances in Research on Low-dose CT Imaging Algorithm Based on Deep Learning
-
摘要:
计算机断层扫描成像(CT)技术具有成像速度快分辨率高的优点,广泛应用于医学临床诊断中。然而,提高剂量辐射会引发人体组织器官受损,降低剂量又会造成成像质量严重下降。为解决上述矛盾,在确保成像质量满足临床诊断需求的条件下,研究如何最大程度地降低X射线辐射对人体造成的伤害,已成为低剂量CT成像技术的研究热点。近年来,在人工智能领域深度学习方法快速发展,已广泛应用于图像处理、模式识别、信号处理等领域。与此同时,大数据驱动下的深度学习方法在LDCT成像领域的应用也有了长足的发展。本文从CT成像的过程、低剂量CT噪声建模以及成像算法的设计3方面,介绍近年来国内外低剂量CT成像算法的发展,尤其对深度学习领域的成像算法进行阐述与分析,并对LDCT图像成像领域未来的发展进行展望。
Abstract:Computed tomography (CT) is widely used in clinical diagnosis because of its fast imaging speed and high resolution. However, higher doses of radiation will cause damages to human tissues and organs, while lower doses will lead to serious deterioration of imaging quality. In order to solve the above contradiction, researchers have focused on the low-dose CT imaging technology to study how to reduce the harm caused by radiation to the human body to the greatest extent under the condition of ensuring the imaging quality to meet the needs of clinical diagnosis. In recent years, deep learning has developed rapidly in the field of artificial intelligence, and has been widely used in image processing, pattern recognition, signal processing fields. Driven by big data, LDCT imaging algorithms based on deep learning have made great progress. This paper studies the development of low-dose CT imaging algorithms in recent years in terms of three aspects: the process of CT imaging, the noise modeling of low-dose CT, and the design of imaging algorithms. In particular, the imaging algorithms in the field of deep learning are systematically elaborated and analyzed. Finally, future developments in the field of LDCT image artifact suppression are also prospected.
-
Keywords:
- deep learning /
- low dose CT /
- artifact suppression /
- noise modeling
-
计算机断层扫描成像(computed tomography,CT)是一种广泛应用于生物医学、图像引导介入、安检、工农业生产、地球物理与石油勘测[1]等领域的无损检测技术。作为医学诊疗的重要辅助手段,CT成像速度快、精度高,可以完整呈现被检查部位的三维信息,且在骨伤、肿瘤与节点、血管病变与肺部积水、细胞癌变等的检测中发挥着不可替代的作用[2]。
目前,常规体检、特定医学诊疗等均需按照要求对被检者进行不同程度的CT检查。有资料表明,在美国,CT检查占所有放射检查的13%,但其导致患者接受的辐射剂量却占患者接受的全部辐射剂量的70%[3]。一般地,人体做一次胸部X射线平片检查所承受的辐射剂量大约为0.1 mSv,而CT检查需要重复使用X射线进行多角度扫描,致使人体承受的辐射剂量比普通平片检查高得多。例如,人体在一次常规胸部CT检查中所受辐射剂量大约是一次胸部平片检查的100倍,乳腺钼靶检查的10倍,而对于癌症患者接受多排CT或CT增强扫描所承受的辐射剂量则更大。伴随着X射线辐射而来的潜在危害包括白内障、新陈代谢异常、生育功能退化、染色体变异导致的胎儿畸变以及癌症等[4]。由于体质弱于成年人,儿童遭受辐射伤害后引发疾病的比例更高,一份来自英国的调查结果表明,在被调查的15周岁以下儿童中,有约1/500死于腹部CT扫描引发的癌症,约1/1500死于脑部CT扫描引发的癌症[5]。相对较高的辐射剂量已成为制约CT成像技术在医学诊疗领域进一步发展的一个重要因素。因此,降低CT扫描的辐射剂量已刻不容缓。然而,辐射剂量降低会引起“光子饥饿”现象,导致重建图像中产生条纹伪影与斑点噪声,进而影响医学诊断的准确性,尤其易导致对面积小、形态细微的早期病变的误诊和漏诊。在此背景下,衍生出了CT成像领域的一个重要研究方向——低剂量CT(low-dose CT,LDCT)技术。
自LDCT出现以来,针对如何提高低剂量条件下CT成像质量这一问题,学者们从降低扫描剂量[6-7]、提升硬件性能[8]与改善成像算法3个角度出发,做了大量研究尝试[9]。首先,由于管电流与辐射剂量之间呈正相关且操作简单,降低管电流是目前临床应用中最常用的降低X射线剂量的方式之一。然而此方法的最大弊端在于获取的LDCT图像密度分辨率较低、出现明显斑点噪声和条状伪影[6];其次,降低管电压也是降低X射线辐射的一种选择,然而管电压降低的同时X射线的穿透能力也将随之下降,进而导致成像质量严重退化。此外,减少X射线数目也是降低辐射剂量的主要方式,这类方法(如内部扫描、少视角、有限角度)获取的投影数据不完备,对重建算法性能有更高的要求[7]。如图1所示,LDCT成像算法主要分为投影域方法、重建方法、后处理方法三方面,在下文中我们分小节进行了详细阐述。
1. 投影域方法与重建方法
1.1 投影域方法
投影数据采集是LDCT成像的前提条件和关键步骤,然而,由于受硬件设备、外部环境等客观因素制约,实际CT扫描系统采集到的投影数据常被大量光子噪声与电子噪声污染,这也是重建图像中出现复杂条状伪影与斑点噪声的主要原因。近年,许多学者致力于研究投影数据的预处理方法,该类方法以投影数据为分析对象,研究如何改善采用滤波反投影(filtered back projection,FBP)方法重建出的LDCT图像的质量,其焦点在于投影数据的统计建模及噪声抑制。
一方面,学者们通过构造正态泊松混合投影数据统计观测模型[10]、研究相邻探测器获取的投影数据之间的相关性[11]、对散射噪声进行估计和校正[12]等方法来解决由数据采集过程中多种客观因素(如X射线多能谱特性、探测器响应不一致、随机噪声等)影响而造成的投影数据原有统计特性被破坏的问题。另一方面,大量研究文献则关注投影数据中噪声的抑制,它们主要可以分为两类:①改善各种线性或非线性滤波器,如Hsieh等[13]提出的能够自适应参数调整的中值滤波方法、Kachelrieß 等[14]提出的基于三维非线性滤波器的噪声抑制方法、基于小波分解的投影滤波法[15]以及基于维纳滤波器[16]或双边滤波器[17]的方法等。这类方法直接对原始投影数据进行处理,将噪声抑制和图像重建看作两个相互独立的过程,便于系统集成,算法复杂度和计算时间远小于迭代重建方法。虽然,该类方法能够充分利用原始数据信息,但是在进行数据修正的过程中不可避免地会出现数据不一致、过校正、欠校正等现象,这些因素往往限制投影数据的精确重建,进而造成重建图像失真、出现伪影或噪声等。②对投影数据的统计建模,如Wang等[18]提出的投影域二次函数惩罚加权最小二乘方法、Zhang等[19]提出的基于各向异性加权先验的低剂量CT正弦图最大后验概率平滑算法和Rudin等[20]提出的针对泊松噪声的全变分滤波方法等。这类方法将投影数据降噪过程视为以投影数据为自变量的目标函数的构建和优化问题,通过考虑含噪声投影数据的分布特性,来构建更加符合投影数据统计特征的统计迭代滤波模型。其优点在于考虑了噪声投影数据的统计特性,缺点在于算法迭代时间较长。
总之,上述两类需人工设计特征提取器的传统算法的主要缺点是人工成本高、特征提取能力差和可移植性弱。此外,也有学者尝试使用深度学习的方法来解决投影数据不完备引起的重建图像质量退化问题,如梁宁宁等[21]提出采用基于切片的生成对抗网络(generative adversarial networks,GAN)来学习投影数据的统计分布规律。这类方法虽然能够在一定程度上克服传统算法的不足,但也存在模型训练效率受限于数据集大小、模型可解释性差等问题。
1.2 传统重建方法
CT成像技术的核心是重建算法,典型的重建算法包括解析法和迭代法[22]。由于具备算法简单、计算速度快等的优点,解析法中的FBP与FDK(feldkamp-daivs-kress)分别成为了二维和三维CT系统的主流选择。然而,解析法对投影数据的完备性要求较高,且对噪声非常敏感,在稀疏角度或有限角度扫描条件下的重建结果往往会受到严重的伪影和噪声污染。迭代法将待重建图像作为未知量,在图像域建立目标函数,并通过迭代求解来获取待重建图像。根据目标函数建立的方式不同,迭代算法可分为代数迭代法和统计迭代重建算法(statistical iterative reconstruction,SIR)。代数迭代法能够节省内存且重建速度快,然而重建后的图像质量并不理想。与传统的解析法和代数迭代法相比,SIR的重建效果更好。
在实际重建过程中,常常通过在目标函数中引入能够反映待重建图像先验信息的正则项来提高重建图像的质量,一般地,SIR的目标函数如下:
$${\varPhi(\boldsymbol{\mu})} = {\Vert \boldsymbol{A \mu - P} \Vert_2^2 + \beta R(\boldsymbol{\mu})}\,, $$ (1) 其中,A表示N×M维的系统矩阵,A中的元素ai,j表示第j个像素对第i个投影的贡献,
$\boldsymbol{\mu} $ 表示待重建图像,P表示投影数据,R$(\boldsymbol{\mu} )$ 表示正则化项,β表示正则化参数。SIR中正则项R$(\boldsymbol{\mu}) $ 的设计一直是这个领域的研究热点[23]。近年发表的文献中,正则项R$(\boldsymbol{\mu}) $ 的典型代表主要包括高斯先验[24]、中值先验[25]、稀疏先验[26]、基于字典学习的先验[27]、以及基于全变分及其变型如TGV[28]、stokeTV先验[29]等。基于正则项约束的统计迭代重建算法考虑了成像系统的物理模型和含噪投影数据的统计特性,能够获取高质量的重建图像;然而,算法复杂度较大、运行过程耗内存等缺点也限制了此类方法的广泛应用。1.3 基于深度学习的重建方法
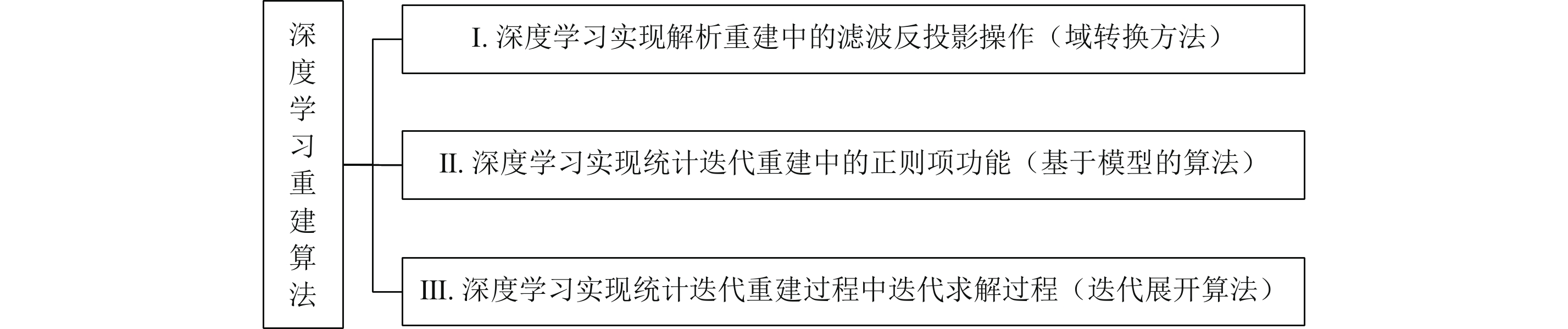
近年,伴随着深度学习在各个领域的成功应用,很多学者尝试通过研究基于深度学习的CT重建方法来克服传统重建算法的局限性。根据深度学习在重建算法中所起的作用,本文将此类重建方法分为如图2所示的3类:深度学习用于实现解析重建中的滤波反投影操作(域转换类方法)、深度学习用于实现统计迭代重建中的正则项功能(基于模型的算法)、深度学习用于实现统计迭代重建过程中的迭代求解过程(迭代展开类算法)。
![]() 图 2 基于深度学习的CT重建算法分类Figure 2. Classification of Deep Learning-based CT Reconstruction Algorithms
图 2 基于深度学习的CT重建算法分类Figure 2. Classification of Deep Learning-based CT Reconstruction Algorithms第Ⅰ类方法将深度学习用于实现解析重建中的滤波反投影操作,主要研究如何采用卷积神经网络(convolutional neural network,CNN)实现投影域与图像域的直接映射。此类方法一般采用网络训练的方式实现解析重建中的滤波与反投影操作,它们可以分为投影域网络+BP和投影域网络+BP+图像域网络两类[30]。
(1)投影域网络+BP是指首先在投影域上对欠完备的投影数据进行修正或者对带噪声的投影数据进行滤波,再利用反投影算法对处理后的投影数据进行重构。一部分研究者致力于滤波器的学习,例如,Pelt等[31]提出在每次迭代过程中通过数据驱动来训练投影域滤波器,采用重建图像的投影数据与实测投影数据的均方误差作为网络约束;Wang等[32]提出的FBP-Net在频域上对滤波器进行改进,网络反投影层中的参数保持不变;另一部分研究者则致力于学习投影域与图像域之间的域转换函数。早期,学者们的研究焦点是全连接层的使用,例如,Zhang等[33]通过对全连接层的权重参数进行分析和可视化,发现全连接层在重建算法中所起的作用与反投影操作相同,可以将其直接应用于反投影过程。Zhu等[34]提出的AUTOMAP网络通过使用全连接层实现了传感器数据与图像域数据的直接映射。由于使用了多个全连接层,这类方法在实现数据转换时增加了网络的计算复杂度,提高了用于网络运行的硬件配置要求。随后,学者们提出了一些采用替代方法来解决全连接层参数问题的算法,Fu等[35]提出采用稀疏连接的方式来减少全连接层的网络参数,其中稀疏连接是通过将全连接层的部分权重值置零来实现的;Ye等[36]对每个角度的投影数据进行单独反投影,并利用CNN来学习反投影数据与图像之间的映射关系。在此基础上,Tao等[37]构造了一种能够反映在不同投影角度上获取的反投影数据信息的三维反投影张量(VVBP-Tensor),并依据像素值大小对每个投影角度上获取的数据进行了排序,指出VVBP-Tensor具备结构自相似性、张量稀疏性与噪声高斯分布的统计特性等特点。此后,该课题组采用CNN实现FBP重建,构建了一种能够学习VVBP-Tensor与重建结果之间映射关系的CT重建网络[38]。
这3种算法的相同点在于其研究对象均是在每个角度上获取的反投影数据。尽管投影域网络+BP类算法能够改善传统FBP的重建结果,但是网络性能受限于投影的数据源,即训练好的网络只适用于解决某一特定成像系统的CT重建问题,并不能有效解决从其他成像系统或不同扫描协议获取的投影数据重建问题,算法鲁棒性较差。
(2)投影域网络+BP+图像域网络是指同时在投影域和图像域设计能够进行噪声抑制的网络。早期,研究者们通常采用将投影域网络、域转换函数与图像域网络按照先后次序进行连接的研究思路来设计双域网络。典型的代表包括:intelligent CT network(iCT-Net)[39],iRadonMAP[40],Dual-domain Residual-based Optimization NEtwork (DRONE)[41],ADAPTIVE-NET[42],hdNet[43],Dual Domain Network(DuDoNet)[44]和Dual-Domain Adaptive-Scaling Non-local Network(DAN-Net)[45]等,其中,DRONE网络采用3阶段训练策略完成重构,在投影域与图像域均采用了残差思想。在第1阶段,该网络采用投影域U-Net来对稀疏投影数据进行扩展;采用图像域(wasserstein GAN,WGAN)来初步重建图像;在第2阶段,采用投影残差网络与图像残差网络来对投影和图像进行细化处理,以输出能够作为先验的投影残差与图像残差;在第3阶段,通过正则化处理,来进一步保障重建图像的质量。DuDoNet网络是双域网络在CT金属伪影抑制任务中的成功尝试。该网络主要包括3部分:正弦域增强网络、Radon逆变换层和图像域增强网络。正弦域增强网络采用了掩码金字塔结构,图像域增强网络采用了U-Net结构。特别地,该方法设计了Radon一致性损失来抑制投影数据中的噪声,通过特定的顺序来处理投影域数据和图像域数据,尽管它们在投影域和图像域均进行了降噪设计,然而由于并未考虑两个域中数据之间的潜在信息交互,常导致重建结果中出现新的伪影。
由此,许多学者尝试通过交互训练来建立投影域与图像域之间的联系。Wang等[46]提出了一种用来解决CT金属伪影抑制问题的交互式双域并行网络(interactive dual-domain parallel network,IDOL-Net)。该网络由分解模块与细化模块组成,其中,分解模块输出的正弦先验与图像先验是细化模块的初始输入;细化模块包括两个分支,分别为用以处理投影数据的FBP分支和用以处理图像的BP分支,两者之间可进行信息交互。Ran等[47]将这种并行交互式策略应用在MRI重建任务中,来探索k-space和空间域数据之间的相互关系。
第Ⅱ类方法将深度学习用于实现SIR中的正则项功能。与传统SIR算法需要人工设计正则化项不同,此类方法中能够反映CT图像先验信息的正则项是可学习的。根据网络模型是否需要预先训练,可将这类方法分为model-based类重建方法和plug-and-play类重建方法。
(1)model-based重建方法在重建过程中直接学习先验信息,例如,Chen等[48]研究了基于“fields of experts”的正则项与卷积神经网络的卷积层之间的关系,用CNN网络来实现重建算法的每次迭代过程。特别地,由于CNN每一层网络的权重值不同,随着迭代过程的推进,网络会不断修正正则化项及超参数。Wu等[49]提出利用k-sparse自动编码器来学习CT图像的非线性稀疏先验,该算法采用了无监督训练模式,对数据集规模要求较小,且网络较为灵活,能对图像特征进行充分提取。Kang等[50]在CNN网络中融入了小波紧框架的思想,构造了一种收敛性较好的降噪网络,该网络在图像纹理细节保留方面表现良好。Gao等[51]充分利用了人体组织结构所具备的自相似性,将训练NDCT数据库所得的特征图作为先验信息来约束重建算法。
(2)plug-and-play重建算法将预训练好的模型作为先验信息,一般地,这类方法常采用交替方向乘子法、原始对偶法等将待求解问题分解为若干个子问题,并通过预训练网络的方式来解决其中的部分子问题。plug-and-play类重建算法是近年学术界的研究热点,该模型由Venkatakrishnan等[52]在2013年首次提出,旨在实现基于成像系统的前向模型与基于图像的先验模型(或降噪模型)之间的相互匹配。此后,2015年,Sreehari等[53]提出了一种基于双随机梯度非局部均值降噪先验(doubly stochastic gradient NLM,DSG-NLM)的重建算法;2021年,Cascarano等[54]将基于数据驱动的DnCNN降噪先验与基于模型驱动的全变差先验进行结合,提出了混合plug-and-play重建算法。第Ⅱ类重建方法的优点是从较小规模的训练数据集重建出的图像质量可观,缺点是其网络结构通常不是前馈神经网络,计算速度较慢。
第 Ⅲ 类方法是基于CNN的迭代展开类算法,主要研究如何采用深度学习网络模块通过网络训练的方式实现SIR中的迭代求解过程。①一部分研究者致力于研究采用端到端的训练方式实现迭代求解过程可学习。例如,Adler等[55]利用CNN网络来学习对偶算子的解,这种操作能够降低采用原始对偶法求解CT重建问题的复杂度;Xia等[56]采用CNN学习最速梯度下降法中的正则化项,提出一种能够同时捕获图像像素级特征与拓扑特征的先验信息;Chen等[57]同时结合了解析重建、统计迭代重建与深度学习算法三者的优点,利用Proximal Forward Backward Splitting算法将目标函数的求解问题转化为保真项与正则化项的迭代求解过程,其中正则化项是通过稠密网络进行学习的。②另一部分研究者则致力于研究采用CNN实现部分超参数可学习。例如,为了解决重建结果与原始测量数据不一致问题,Gupta等[58]将投影梯度下降算法中的投影算子用残差网络进行了代替,设计了1种可学习的松弛投影梯度下降算法,该算法具有较好的收敛性;Zhang等[59]提出了1种具有自学习特性网络MetaInv-Net,通过CNN来学习共轭梯度下降算法的初值。尽管迭代展开策略能为CT重建任务提供一种新的网络结构设计思路,但它造成的网络计算负荷通常较大。
2. 后处理方法
在图像域,以抑制图像中噪声和伪影为研究目标,直接对重建图像进行处理的方法称为后处理方法。由于其在图像域进行操作,不依赖于原始投影数据,可移植性较强,便于推广,后处理方法已经成为LDCT成像领域的热点研究方向。后处理算法主要分为两类:传统后处理算法与基于深度学习的后处理方法。
2.1 传统后处理算法
在深度学习被广泛应用之前,LDCT图像伪影抑制主要通过传统后处理方法来实现。经典算法中,由于能够有效利用图像像素之间的结构相似性,基于非局部均值(non-local means,NLM)[60]及其改进形式[61]的方法取得了较好的降噪效果。
Chen等[62]提出的基于大尺度邻域非局部均值滤波的LDCT伪影抑制方法,考虑了大尺度窗口内像素结构的相似性,伪影抑制效果较好。此外,也有许多在变换域进行LDCT图像降噪的探索,如基于多尺度奇异点检测的LDCT图像小波去噪算法[63]、在小波域对NLM方法进行改进的三维块匹配滤波[64]算法和基于稀疏表示和字典学习[65]的方法也是LDCT图像降噪领域近年的研究热点。传统方法还包括自适应多尺度全变分LDCT图像降噪方法[66]、基于Curvelet双线性插值的LDCT图像降噪方法[67]等。这些传统算法主要运用数学分析、现代信号处理与数字图像处理等理论来解决CT图像降噪问题,算法原理过于依赖人工设计难以灵活调整,其性能有较大的局限性。
2.2 基于深度学习的LDCT图像后处理方法
深度学习技术通过对样本特征的自动学习,将低维浅层特征映射到高维深层特征,学习数据本质特征的能力非常优异。伴随着卷积层、池化层、激活函数、批量归一化等基础层的构建,网络训练能力大大提升,深度学习已成功应用于超分辨率重构、图像翻译、图像降噪等自然图像处理领域。
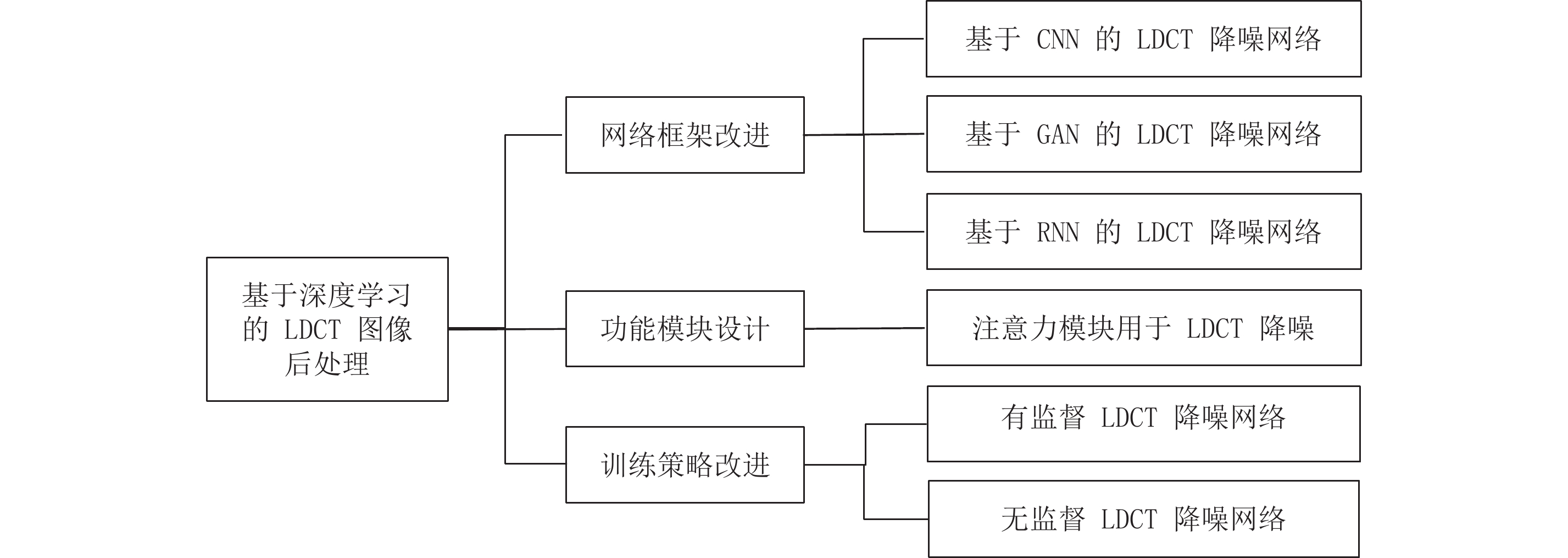
近年,研究者们尝试采用深度学习解决LDCT图像伪影噪声抑制问题。学者们的研究热点主要集中在网络框架改进、训练策略改进及功能模块设计等方面(图3)。
![]() 图 3 基于深度学习的LDCT图像后处理算法分类Figure 3. Classification of deep learning-based LDCT image post-processing algorithms
图 3 基于深度学习的LDCT图像后处理算法分类Figure 3. Classification of deep learning-based LDCT image post-processing algorithms2.2.1 网络框架改进
一般地,网络降噪性能受算法框架与功能模块类型的影响,选择不同的算法框架(例如2D CNN[68],3D CNN[69],Wasserstein GAN[70],CycleGAN[71]或长短期记忆网络(long short term memory network,LSTM)[72]等)会使降噪网络的复杂度不尽相同,不同的功能模块如增加注意力模块、特征补充模块与图像分解模块等,也会使网络的性能表现不尽相同。近年,用于LDCT降噪领域的主流深度学习网络架构主要分为3类:基于CNN的LDCT降噪网络、基于GAN的LDCT降噪网络和基于循环神经网络(recurrent neural networks,RNN)的LDCT降噪网络,其中,CNN具有优异的特征提取能力,GAN具有强大的图像生成能力,RNN具有独特的时空特性。这些网络已广泛应用于机器视觉的各个领域,在LDCT图像伪影抑制方面也有不错表现。
CNN是一种模拟人脑功能、包含卷积运算且基于多层监督学习的人工神经网络。得益于CNN强大的特征学习与映射能力,与传统算法相比,CNN在处理LDCT图像降噪问题时表现更加优越。在近年涌现出来的诸多研究成果中,一部分学者致力于通过增加网络层数和改进网络结构来提高网络的降噪性能。
2012年,Burger等[73]利用多层感知机网络来学习噪声图像与干净图像之间的函数映射关系,实现了深度学习在自然图像降噪领域的首次成功尝试。在此基础上,研究者们在寻找能够高度拟合这一函数映射关系的网络方面做了许多尝试,其典型代表包括包含三层卷积层的LDCT降噪网络[68]、基于残差编解码结构的CNN网络[74]、基于U-Net的LDCT降噪网络[75]等。也有一部分学者尝试级联多个网络,通过分阶段处理来改善降噪图像的质量。例如,Wu等[76]提出了一种渐进式级联CNN;Shan等[77]提出了一种由结构相同的多个传输链路导向的编解码模块(conveying-link-oriented network encoder-decoders,CLONEs)组成的自适应处理神经网络模型,该网络中每个CLONE对降噪结果进行逐层改善,这样做不仅可以保障基本降噪任务的实现,而且可以通过上层模块对下层模块的指导实现降噪图像质量的进一步提升。此外,CNN强大的特征提取能力的实现是建立在成对数据集比较充足的前提之上,而实际临床应用中成对的CT数据往往并不容易取得,这也就限制了CNN在LDCT降噪领域的进一步发展。综上,改善基于CNN的LDCT降噪网络既需要兼顾特征提取的有效性和网络复杂度,又需要考虑数据集的大小。未来,改善基于CNN的LDCT降噪网络的性能可从完善特征提取的方式、寻找高效的卷积操作以及在网络中嵌入功能子网络等角度入手。
GAN是一种基于博弈对抗思想的无监督生成式网络模型,主要由生成器G(Generator)与判别器D(Discriminator)两部分构成。在基于GAN的LDCT降噪任务中,G的任务是生成一幅能够以假乱真的“假NDCT图像”,D的任务是对真实NDCT和生成的“假NDCT”的真伪做出尽可能接近事实的判断,通过G和D的博弈对抗和交替训练,最终完成LDCT图像降噪任务。
近年,学者们主要从两个角度来提高GAN网络的降噪性能:①通过改进G、D、引入功能子网络或者改变网络的连接方式来改善GAN的特征提取能力。在这类方法中,多数研究成果均集中在对生成器与判别器的改进方面。其中的典型代表包括含7层卷积层的生成器[78]、包含对称编解码结构U-Net256的生成器[79]、基于PatchGAN分切片进行真伪判别的判别器[80]和基于Inception结构多尺度进行真伪判别的判别器[81]。在功能子网络的引入或者网络的连接方式改进方面,Yi等[79]在GAN中引入了一种清晰度检测网络,该功能网络的加入能够抑制边缘模糊现象,且对被噪声污染的图像低对比度区域的细节进行修复;You等[82]利用点卷积能够实现特征降维这一优点,在GAN中调整了卷积方式,在降低网络复杂度的同时提高了伪影抑制效果。基于网络结构的改进方法能够在一定程度上提高GAN生成图像的质量,然而当输入样本分布复杂且G和D初始化不恰当时,极易产生模型崩塌、训练不稳定等问题。②通过改进损失函数的形式或者运用多损失函数进行约束来提高GAN训练的稳定性。以往常采用KL散度或者JS散度来评价GAN中两个不同分布之间的差异性,然而当真实数据与生成数据分布一致时,采用上述两种损失函数约束GAN常会致使反向传播过程中出现梯度消失现象。为了克服这一难题,Arjovsky等[83]提出了用Wassertein距离来衡量真实数据与生成数据分布的Wassertein GAN(WGAN)网络,Wassertein距离的引入使得GAN的训练更加稳定。然而,由于WGAN采用权重裁剪策略来使梯度强行满足Lipschitz条件,最终导致GAN在训练过程中产生不可控的结果,生成图像的质量并不总令人满意。Li等[84]改进了WGAN中的梯度裁剪策略,增加了梯度惩罚这一正则项,该方法取得了比WGAN更稳定的效果。Yang等[70]通过将Wassertein Distance与感知损失同时应用于普通的GAN中来提高GAN网络训练的稳定性。此外,最小二乘损失(LSGAN)[85]、频谱归一化损失(SNGAN)[86]、嵌入保真度的损失(f-GAN)[87]等也是目前常用的损失函数。
综上,在训练数据有限的情况下,采用GAN网络可以生成清晰度良好的降噪结果,然而训练不稳定、模型崩溃等问题一直是限制基于GAN的降噪网络性能提升的重要因素。
RNN可以看成一个在时间上传递的神经网络,不仅将当前的输入样本作为网络输入,还将它们之前感知到的信息一并作为输入,有助于上下文信息的获取。考虑到CT图像在获取过程中通常具有连续性,前一帧CT图像与后一帧CT图像之间具有紧密的联系,因此将RNN用来解决基于CT序列的LDCT图像降噪问题也是一种可行方案。例如,Du等[88]提出利用长短期记忆网络来学习LDCT图像的注意力图,Rajeev等[89]提出了一种基于批量归一化和长短期记忆网络来去除白噪声与椒盐噪声的有效系统。
2.2.2 训练策略改进
在LDCT伪影噪声抑制领域,训练方式也是决定CT图像质量的关键因素。根据训练数据集是否成对出现,可以将训练分为有监督训练与无监督训练。有监督训练是指利用一组已知类型的成对训练数据来对网络进行训练。有监督训练有助于人们从具有大量特征的图像中快速提炼有价值的信息,避免了不必要的训练。由于其是一种目的明确的训练方式,因此可以产生符合预期、质量较高的图像,且输出图像的质量可以进行衡量。由于有大量成对数据集作为依托且训练准确度较高,因此主流的LDCT降噪算法均采用有监督训练机制,如Chen等[74]采用成对的NBIA(the National Biomedical Imaging Archive)数据集来训练残差编解码CNN、Wu等[76]采用成对的mayo数据集来训练级联CNN,均产生了一定的降噪效果。然而,由于仅在像素级上对网络的输出结果进行了约束,这两种算法的降噪效果并不十分理想。由此可见,决定有监督训练方式有效性的一个重要因素是目标函数的设置。
为了解决上述问题,研究者们试图在目标函数上进行改进,以提高降噪精度。Yang等[90]利用预训练的VGG网络分别提取降噪结果与NDCT的特征,在特征空间上对降噪结果加以约束;Yi等[79]提出了一种用来约束CT图像边缘特征的损失函数;You等[91]将像素级L1损失与基于图像质量评价指标——多尺度结构相似性的损失函数相结合,来共同约束网络训练过程。虽然,有监督训练在LDCT图像降噪任务上表现优异,但是,有监督训练对CT数据集有严格的要求,即训练数据集必须包括LDCT以及与之对应的NDCT,由于重复扫描会对人体带来极大危害,临床应用中成对的LDCT与NDCT图像较少,有监督训练的有效性难以得到保障。
无监督训练本质上是一个统计方法,在没有标签的数据里,通过数据自身存在的规律,来发现潜在的一些结构特征。由于对数据集没有严格的要求,无监督训练近年逐渐成为CT成像领域的研究热点。Zhu等[71]首次提出了采用无监督训练方式对网络进行训练的CycleGAN:在没有配对数据的情况下,首先学习一个函数映射G:X→Y,将图像从源域X转换到目标域Y,使得来自G(X)的图像分布与Y分布不会因对抗损失而产生模糊现象,之后再进行逆映射F:Y→X并引入循环一致性损失,使得
$F\Big(G\big(X\big)\Big)$ ≈X。CycleGAN在无监督训练领域的表现优越,其网络训练的策略被研究者们广泛应用。如Gu等[92]对CycleGAN的网络结构进行了微调,通过在生成器中引入自适应实例归一化层,仅采用单个生成器完成了在LDCT图像域与NDCT图像域之间的相互转换过程;Kwon等[93]则将可逆的生成器应用在CycleGAN网络中,利用一个生成器与一个判别器实现无监督循环;Liao等[94]首次将CycleGAN应用于金属伪影抑制问题中,通过对CT图像噪声伪影特征与结构特征进行分解并分开训练,不仅实现了LDCT降噪任务,而且能够合成与真实LDCT接近的新LDCT图像。上述方法均采用循环对抗思想与多损失函数约束来实现CT图像降噪网络的无监督训练,并取得了良好的降噪效果。在无监督训练中采用多损失函数进行约束面临的问题在于:如何在众多损失函数中合理地选取损失函数组合,以及如何准确地调整超参数来改变不同损失函数在训练过程中所起的作用大小。
2.2.3 功能子模块设计
实际临床应用中,LDCT图像中伪影分布极其不规律且与组织位置息息相关,伪影和噪声等干扰信息往往与人体正常组织和低密度病变等有用信息具有相似的分布规律,这使得如何将两类信息有效分离成为后处理类方法的研究重点和难点。为了能够准确地提取LDCT图像中不同尺度、密度和位置的伪影特征,研究者们试图将具有某一特定功能的子网络引入到LDCT降噪网络的设计中来。例如,为了抑制LDCT图像中存在的运动伪影,Ko等[95]在残差网络中引入了自注意力模块,该模块通过调整伪影特征的权重来加强或削弱所提取伪影特征的重要性;考虑到LDCT成像过程中的统计不确定性,Du等[88]将视觉注意力网络分别引入生成器与判别器中,使得网络对伪影与其周围的结构信息更加敏感。考虑到CT图像本身在人体组织结构上具有强大的相关性,同时在连续拍摄CT过程中相邻帧图像之间具有依赖性,Li等[96]提出同时结合空间注意力与帧间注意力的CNN网络,该论文最大的亮点在于将视频处理的思路巧妙地运用在图像处理中,同时利用切片内与切片间的相关性,使得网络在特征提取过程中有了更多的先验信息作为指导。该算法要求获取连续扫描的CT图像序列作为输入,由于对数据集有很高的要求,该网络性能的最大化受到了限制。
因此,不管是自注意力网络,还是双注意力网络,注意力网络均是一种功能子网络,能够实现图像特定特征的有效提取。类似的功能子网络包括提取密度特征[97]、深度特征[98]、噪声水平特征[99]、伪影位置特征[100]与梯度信息[101]等的功能模块。
3. 数据集
3.1 投影域CT数据集
LDCT-and-Projection-data数据集是由Mccolloigh等[102]研究人员在国家生物医学成像和生物工程研究所的资助下,以DICOM-CT-PD格式(包含CT投影数据和采集几何)建立的CT患者投影数据库。该数据集提供了包括各种检查类型扫描(如急性认知或运动障碍的99次非对比头部CT扫描、用于筛查高风险患者肺部结节的100次低剂量非对比胸部扫描以及为寻找转移性肝脏病变而获得的100次腹部增强CT扫描)重建后的CT图像、患者年龄和性别以及病理注释等信息。每种扫描类型的50个病例来自SomATOM定义的Flash CT扫描仪(西门子医疗保健公司,Forchheim,德国),49例头部病例、50例胸部病例、50例腹部病例来自光速VCT CT扫描仪(GE Healthcare,Waukesha,WI)。对于每一位患者的CT扫描,该数据还提供包括全剂量和模拟的低剂量水平的3种类型的CT投影数据:DICOM-CT-PD投影数据、DICOM图像数据和Excel临床数据报告。此外,还针对性地对商业CT提供了相应的重建后的CT图像(所有CT图像均采用滤波反投影方法重建)。这些数据将极大地促进新的CT重建与去噪算法的研究,包括那些与深度学习相关的算法。
3.2 图像域CT数据集
3.2.1 模拟数据集
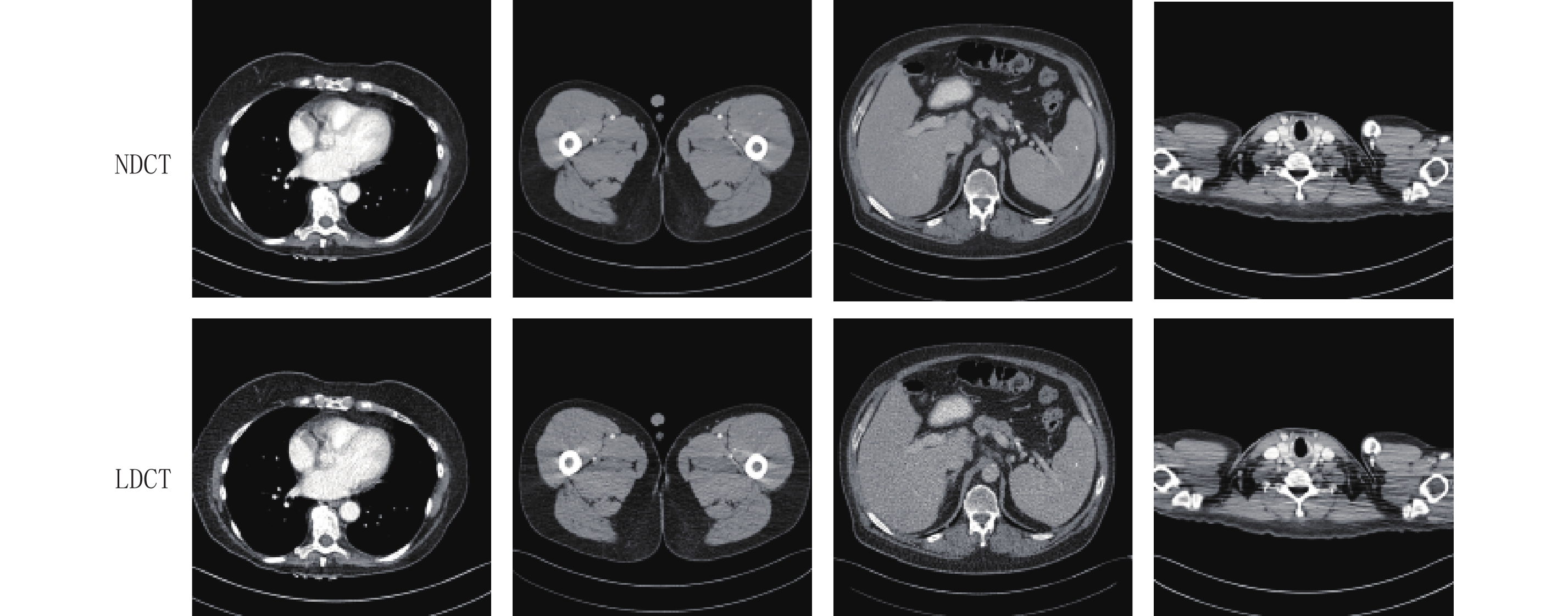
自从被Mayo Clinics首次授权应用于“the 2016 NIH-AAPM-Mayo Clinic Low Dose CT Grand Challenge”以后,Mayo数据集[103]成为了LDCT研究领域广泛应用的数据集。该数据集共包含来自10名匿名患者的2378幅3 mm厚度的腹部CT图像,其中包括NDCT图像与其对应的四分之一剂量CT图像,图像大小均为512×512,NDCT数据是在管电流与管电压分别为200 mAs与120 kV情况下得到的,而LDCT则是插入了泊松噪声低剂量CT图像。
图4展示了从Mayo数据集中提取的人体不同部位CT示意图,其中第1行表示NDCT图像,第2行表示与之对应的LDCT图像。通过对比可以发现,LDCT图像中包含大量的噪声与伪影,破坏了人体组织结构与病理信息,不利于后期医生的诊断。而在NDCT中却可以清晰地看出软组织结构、组织细微边缘等信息。由此可见,LDCT图像噪声伪影抑制是一个很有意义的研究课题。
除此之外,不同的模拟数据集纷纷被构建。国家生物医学影像档案(the national biomedical imaging archive,NBIA)CT数据集[104]包括165名患者的NDCT数据集共7015张,每张图像大小为256×256。考虑到假设使用单色源,CT扫描的投影测量遵循泊松分布这一基本规律,研究者们在正常剂量扫描情况下获取的正弦图中加入泊松噪声,形成了相应的LDCT图像。NBIA数据集具有多样性,包括了人体不同组织结构,能够更加真实地反映临床成像。TCIA(the cancer imaging archive)数据集[105]是一个包含常见肿瘤医学图像及相应临床信息的大规模公用数据库,运用相同的模拟LDCT图像原理,首先对原始图像做投影变换,并在投影域中加入泊松噪声,再通过FBP算法重建出CT图像。运用同样方式模拟的数据集包括TCGA-COAD[106]临床CT数据集。不像临床数据集中噪声的分布不可控制,模拟数据集可以人为调整噪声水平的大小,以获得不同剂量的LDCT图像,能够进一步证明不同算法的鲁棒性。
表 1 典型的CT成像算法在现有数据集上性能比较Table 1. Performance comparison of typical CT imaging algorithms on existing data sets方法 主要特点 优点 缺点 传统 CT 重建算法 FBP 解析类且最基础的重建算法 成像速度快,鲁棒性好 对稀疏角度 CT 重建质量不佳 TV-POCS 迭代重建类算法,使用了 TV 正则化项进行约束 研究对象为原始数据,不容易丢失信息,降噪效果优于 FBP 算法 降噪结果容易产生块状伪影,且部分重要的细微结构被平滑 传统 CT 后处理算法 BM3D 基于块匹配的后处理 细节保留能力优于 TV- POCS 降噪结果出现了模糊与失真 K-SVD 基于字典学习的后处理 算法运算时间较长,降噪结果中仍然存在部分伪影 基于深度学习的 CT 重建算法 iCT-Net 用 CNN 学习 FBP:投影数据扩展;滤波;反投影;求和 对稀疏角度、短扫描内部扫描 CT 重建效果良好 并未解决锥束 CT 重建问题,网络参数较多 LEARN 迭代展开类算法,对“fields of experts”进行展开,并用 CNN 进行学习 重建结果保留了更多的边缘与细节,比传统迭代算法更高效 鲁棒性较差,对正则化函数具有一定的限制 DRONE 双域残差优化网络 重建精度高 需要更多数据集进行训练 基于深度学习的 CT 后处理算法 RED-CNN CNN 网络,包括 5 层编码与 5 层解码,其中初始输入、第 2、4 层编码端特征通过残差连接并入相应解码端 降噪效果优于传统后处理算法,降噪结果中伪影残留量较少 降噪结果容易产生图像过平滑现象,丢失了一些细微信息,如血管等 WGAN-VGG GAN 网络,G:8 层 conv,D:6 层 conv,2 层 FC,损失函数:WGAN+VGG 训练稳定性较好,能够有效缓解图像过平滑问题 在抑制伪影的过程中易破坏图像原有结构,引入新的噪声 SACNN CNN 网络,同时采用自注意力与自编码模块 在伪影抑制与结构保留方面实现了较好的平衡 降噪结果中仍然存在部分噪声,细微结构产生了失真 3.2.2 真实数据集
piglet数据集[107]中的LDCT图像运用GE扫描仪(Discovery CT750 HD)(原电压设为100 kVp,切片厚度设为0.625 mm)在仔猪身上进行实验,通过调整扫描过程中的管电流大小进而获取不同剂量的LDCT图像,管电流调整范围从300 mAs到15 mAs。图5给出了不同剂量piglet数据集CT示意图,其中300 mAs管电流获得的图像为NDCT(图5(a)),管电流分别降至原电流的50%、25%、10% 与5% 从而获得不同剂量的LDCT图像(图5(b)~图5(e))。该数据集可以通过调整管电流来获取不同剂量的CT图像,操作灵活,适用性强。然而,由于人体组织结构与仔猪存在一定的差异,形成的LDCT也并不准确。
4. 总结
CT技术具有成像速度快、质量高、硬件成本低的优点,已成为医学诊疗领域一种不可或缺的成像手段广泛应用于临床诊断中。与此同时,由X射线辐射所引发的一系列人体损伤也逐渐被人们所重视。LDCT成像技术在降低X射线剂量的同时研究如何提高CT成像的质量,已成为CT成像领域的研究热点。近年来,学者们针对这一课题已经进行了大量的研究,尤其是基于深度学习的LDCT成像技术取得了长足的发展。本文总结基于深度学习的LDCT成像技术的最新发展。①本文从投影域方法、重建方法与后处理方法这3个角度对目前LDCT成像技术进行了阐述并分析每类方法的优缺点,重点分析基于深度学习的LDCT成像技术的发展;②总结LDCT成像领域广泛使用的数据集;③对目前LDCT成像领域的研究现状以及未来的发展方向进行展望。
深度学习已成为LDCT成像领域新的热点研究方向。目前,深度学习应用于LDCT成像领域仍然面临3个主要问题:①网络对分布规律复杂的伪影与噪声的特征提取能力不足;②数据集不足制约了深度学习网络的训练;③复杂的网络结构对GPU性能提出了更高的要求。未来,将传统CT重建算法与深度学习相结合,投影域方法、变换域(如小波域)与图像域方法相结合、CT成像硬件设备与软件算法相结合,将会进一步提升LDCT的成像质量。
-
![]()
图 2 基于深度学习的CT重建算法分类
Figure 2. Classification of Deep Learning-based CT Reconstruction Algorithms
![]()
图 3 基于深度学习的LDCT图像后处理算法分类
Figure 3. Classification of deep learning-based LDCT image post-processing algorithms
1 典型的CT成像算法在现有数据集上性能比较
方法 主要特点 优点 缺点 传统 CT 重建算法 FBP 解析类且最基础的重建算法 成像速度快,鲁棒性好 对稀疏角度 CT 重建质量不佳 TV-POCS 迭代重建类算法,使用了 TV 正则化项进行约束 研究对象为原始数据,不容易丢失信息,降噪效果优于 FBP 算法 降噪结果容易产生块状伪影,且部分重要的细微结构被平滑 传统 CT 后处理算法 BM3D 基于块匹配的后处理 细节保留能力优于 TV- POCS 降噪结果出现了模糊与失真 K-SVD 基于字典学习的后处理 算法运算时间较长,降噪结果中仍然存在部分伪影 基于深度学习的 CT 重建算法 iCT-Net 用 CNN 学习 FBP:投影数据扩展;滤波;反投影;求和 对稀疏角度、短扫描内部扫描 CT 重建效果良好 并未解决锥束 CT 重建问题,网络参数较多 LEARN 迭代展开类算法,对“fields of experts”进行展开,并用 CNN 进行学习 重建结果保留了更多的边缘与细节,比传统迭代算法更高效 鲁棒性较差,对正则化函数具有一定的限制 DRONE 双域残差优化网络 重建精度高 需要更多数据集进行训练 基于深度学习的 CT 后处理算法 RED-CNN CNN 网络,包括 5 层编码与 5 层解码,其中初始输入、第 2、4 层编码端特征通过残差连接并入相应解码端 降噪效果优于传统后处理算法,降噪结果中伪影残留量较少 降噪结果容易产生图像过平滑现象,丢失了一些细微信息,如血管等 WGAN-VGG GAN 网络,G:8 层 conv,D:6 层 conv,2 层 FC,损失函数:WGAN+VGG 训练稳定性较好,能够有效缓解图像过平滑问题 在抑制伪影的过程中易破坏图像原有结构,引入新的噪声 SACNN CNN 网络,同时采用自注意力与自编码模块 在伪影抑制与结构保留方面实现了较好的平衡 降噪结果中仍然存在部分噪声,细微结构产生了失真  下载: 导出CSV
下载: 导出CSV
表 1 典型的CT成像算法在现有数据集上性能比较
Table 1 Performance comparison of typical CT imaging algorithms on existing data sets
方法 主要特点 优点 缺点 传统 CT 重建算法 FBP 解析类且最基础的重建算法 成像速度快,鲁棒性好 对稀疏角度 CT 重建质量不佳 TV-POCS 迭代重建类算法,使用了 TV 正则化项进行约束 研究对象为原始数据,不容易丢失信息,降噪效果优于 FBP 算法 降噪结果容易产生块状伪影,且部分重要的细微结构被平滑 传统 CT 后处理算法 BM3D 基于块匹配的后处理 细节保留能力优于 TV- POCS 降噪结果出现了模糊与失真 K-SVD 基于字典学习的后处理 算法运算时间较长,降噪结果中仍然存在部分伪影 基于深度学习的 CT 重建算法 iCT-Net 用 CNN 学习 FBP:投影数据扩展;滤波;反投影;求和 对稀疏角度、短扫描内部扫描 CT 重建效果良好 并未解决锥束 CT 重建问题,网络参数较多 LEARN 迭代展开类算法,对“fields of experts”进行展开,并用 CNN 进行学习 重建结果保留了更多的边缘与细节,比传统迭代算法更高效 鲁棒性较差,对正则化函数具有一定的限制 DRONE 双域残差优化网络 重建精度高 需要更多数据集进行训练 基于深度学习的 CT 后处理算法 RED-CNN CNN 网络,包括 5 层编码与 5 层解码,其中初始输入、第 2、4 层编码端特征通过残差连接并入相应解码端 降噪效果优于传统后处理算法,降噪结果中伪影残留量较少 降噪结果容易产生图像过平滑现象,丢失了一些细微信息,如血管等 WGAN-VGG GAN 网络,G:8 层 conv,D:6 层 conv,2 层 FC,损失函数:WGAN+VGG 训练稳定性较好,能够有效缓解图像过平滑问题 在抑制伪影的过程中易破坏图像原有结构,引入新的噪声 SACNN CNN 网络,同时采用自注意力与自编码模块 在伪影抑制与结构保留方面实现了较好的平衡 降噪结果中仍然存在部分噪声,细微结构产生了失真
下载: 导出CSV
-
[1] BRENNER D J, HALL E J. Computed tomography: An increasing source of radiation exposure[J]. New England Journal of Medicine, 2007, 357(22): 2277−2284.
[2] SMITH-BINDMAN R, LIPSON J, MARCUS R, et al. Radiation dose associated with common computed tomography examinations and the associated lifetime attributable risk of cancer[J]. Archives of Internal Medicine, 2009, 169(22): 2078−2086. doi: 10.1001/archinternmed.2009.427
[3] HART D, WALL B F. UK population dose from medical X-ray examinations[J]. European Journal of Radiology, 2004, 50(3): 285−291. doi: 10.1016/S0720-048X(03)00178-5
[4] HSIEH J. Computed tomography: Principles, design, artifacts, and recent advances[M]. SPIE Press, 2003.
[5] SHRIMPTON P C, HILLIER M C, LEWIS M A, et al. Doses from computed tomography (CT) examinations in the UK-2003 review[M]. National Radiological Protection Board, 2005.
[6] SIGAL-CINQUALBRE A B, HENNEQUIN R, ABADA H T, et al. Low-kilovoltage multi-detector row chest CT in adults: Feasibility and effect on image quality and iodine dose[J]. Radiology, 2004, 231(1): 169−174. doi: 10.1148/radiol.2311030191
[7] YEDDER H B, CARDOEN B, HAMARNEH G. Deep learning for biomedical image reconstruction: A survey[J]. Artificial Intelligence Review, 2021, 54(1): 215−251.
[8] 柳澄, 秦维昌. 多层螺旋CT(一)[J]. 医学影像学杂志, 2000,10(3): 194−195. [9] SHANGGUAN H. Study on statistical iterative reconstruction methods for low-dose X-ray CT[D]. Taiyuan: North University of China, 2016.
[10] MA J, LIANG Z, FAN Y, et al. Variance analysis of X-ray CT sinograms in the presence of electronic noise background[J]. Medical Physics, 2012, 39(7): 4051−4065.
[11] ZHANG H, OUYANG L, MA J, et al. Noise correlation in CBCT projection data and its appli-cation for noise reduction in low-dose CBCT[J]. Medical Physics, 2014, 41(3): 031906. doi: 10.1118/1.4865782
[12] XIE S P, LUO L M, YANG L F, et al. Scatter correction method for cone beam CT using beam attenuation grid[C]//Key Engineering Materials. Trans Tech Publications Ltd, 2011, 480: 341-346.
[13] HSIEH J. Adaptive streak artifact reduction in computed tomography resulting from excessive X-ray photon noise[J]. Medical Physics, 1998, 25(11): 2139−2147.
[14] KACHELRIEβ M, WATZKE O, KALENDER W A. Generalized multi-dimensional adaptive filtering for conventional and spiral single-slice, multi-slice, and cone-beam CT[J]. Medical Physics, 2001, 28(4): 475−490.
[15] SAHINER B, YAGLE A E. Image reconstruction from projections under wavelet constraints[J]. IEEE Transactions on Signal Processing, 1993, 41(12): 3579−3584. doi: 10.1109/78.258101
[16] YAZDI M, BEAULIEU L. Artifacts in spiral X-ray CT scanners: Problems and solutions[J]. International Journal of Biological and Medical Sciences, 2008, 4(3): 135−139.
[17] DEMIRKAYA O. REDUCTION of noise and image artifacts in computed tomography by nonlinear filtration of projection images[C]//Medical Imaging 2001. International Society for Optics and Photonics, 2001: 917-923.
[18] WANG J, LL T, LU H, et al. Penalized weighted least-squares approach for low-dose X-ray computed tomography[C]//Medical Imaging 2006: Physics of Medical Imaging. International Society for Optics and Photonics, 2006, 6142: 614247.
[19] ZHANG Q, GUI Z, CHEN Y, et al. Bayesian sinogram smoothing with an anisotropic diffusion weighted prior for low-dose X-ray computed tomography[J]. Optik-International Journal for Light and Electron Optics, 2013, 124(17): 2811−2816. doi: 10.1016/j.ijleo.2012.08.045
[20] RUDIN L I, OSHER S, FATEMI E. Nonlinear total variation based noise removal algorithms[J]. Physica D: Nonlinear Phenomena, 1992, 60(1): 259−268.
[21] 梁宁宁, 李子恒, 王林元, 等. 一种基于GAN网络投影补全的有限角度CT重建算法[J]. 中国体视学与图像分析, 2019,24(1): 1−8. LIANG N, LI Z, WANG L, et al. A limited-angle computed tomography reconstruction algorithm based on projection completion via generative adversarial networks[J]. Chinese Journal of Stereology and Image Analysis, 2019, 24(1): 1−8. (in Chinese).
[22] GORDON R, BENDER R, HERMAN G T. Algebraic reconstruction techniques (ART) for three- dimensional electron microscopy and X-ray photography[J]. Journal of Theoretical Biology, 1970, 29(3): 471−481. doi: 10.1016/0022-5193(70)90109-8
[23] ZHANG H, WANG J, MA J, et al. Statistical models and regularization strategies in statistical image reconstruction of low-dose X-ray CT: A survey[J]. arXiv preprint arXiv: 1412.1732, 2014.
[24] LEVITAN E, HERMAN G T. A maximum a posteriori probability expectation maximization algorithm for image reconstruction in emission tomography[J]. IEEE Transactions on Medical Imaging, 1987, 6(3): 185−192. doi: 10.1109/TMI.1987.4307826
[25] HSIAO T, RANGARAJAN A, GINDI G. A new convex edge-preserving median prior with applications to tomography[J]. IEEE Transactions on Medical Imaging, 2003, 22(5): 580−585. doi: 10.1109/TMI.2003.812249
[26] LU Y, ZHAO J, WANG G. Few-view image reconstruction with dual dictionaries[J]. Physics in Medicine & Biology, 2011, 57(1): 173.
[27] BAI T, MOU X, XU Q, et al. Low-dose CT reconstruction based on multiscale dictionary[C]//International Society for Optics and Photonics. Medical Imaging 2013: Physics of Medical Imaging, 2013, 8668: 86683L.
[28] NIU S, GAO Y, BIAN Z, et al. Sparse-view X-ray CT reconstruction via total generalized variation regularization[J]. Physics in Medicine and Biology, 2014, 59(12): 2997. doi: 10.1088/0031-9155/59/12/2997
[29] LIU Y, LIANG Z, MA J, et al. Total variation-stokes strategy for sparse-view X-ray CT image reconstruction[J]. IEEE Transactions on Medical Imaging, 2013, 33(3): 749−763.
[30] LIANG K, YANG H, XING Y. Comparison of projection domain, image domain, and comprehensive deep learning for sparse-view X-ray CT image reconstruction[J]. arXiv preprint arXiv: 1804.04289, 2018.
[31] PELT D M, BATENBURG K J. Improving filtered backprojection reconstruction by data-dependent filtering[J]. IEEE Transactions on Image Processing, 2014, 23(11): 4750−4762. doi: 10.1109/TIP.2014.2341971
[32] WANG B, LIU H. FBP-Net for direct reconstruction of dynamic PET images[J]. Physics in Medicine & Biology, 2020, 65(23): 235008.
[33] ZHANG Q, LIANG D. Visualization of fully connected layer weights in deep learning CT reconstruction[J]. arXiv preprint arXiv: 2002.06788, 2020.
[34] ZHU B, LIU J Z, CAULEY S F, et al. Image reconstruction by domain-transform manifold learning[J]. Nature, 2018, 555(7697): 487−492. doi: 10.1038/nature25988
[35] FU L, DE MAN B. A hierarchical approach to deep learning and its application to tomographic reconstruction[C]//International Society for Optics and Photonics. 15th International Meeting on Fully Three-Dimensional Image Reconst- ruction in Radiology and Nuclear Medicine, 2019, 11072: 1107202.
[36] YE D H, BUZZARD G T, RUBY M, et al. Deep back projection for sparse-view CT reconstruction[C]//2018 IEEE Global Conference on Signal and Information Processing (GlobalSIP). IEEE, 2018: 1-5.
[37] TAO X, ZHANG H, WANG Y, et al. VVBP-tensor in the FBP algorithm: Its properties and application in low-dose CT reconstruction[J]. IEEE transactions on medical imaging, 2019, 39(3): 764−776.
[38] TAO X, WANG Y, LIN L, et al. Learning to reconstruct CT images from the VVBP-tensor[J]. IEEE Transactions on Medical Imaging, 2021.
[39] LI Y, LI K, ZHANG C, et al. Learning to reconstruct computed tomography images directly from sinogram data under a variety of data acquisition conditions[J]. IEEE Transactions on Medical Imaging, 2019, 38(10): 2469−2481. doi: 10.1109/TMI.2019.2910760
[40] HE J, WANG Y, MA J. Radon inversion via deep learning[J]. IEEE Transactions on Medical Imaging, 2020, 39(6): 2076−2087. doi: 10.1109/TMI.2020.2964266
[41] WU W, HU D, NIU C, et al. DRONE: Dual-domain residual-based optimization network for sparse-view CT reconstruction[J]. IEEE Transactions on Medical Imaging, 2021.
[42] GE Y, SU T, ZHU J, et al. ADAPTIVE-NET: Deep computed tomography reconstruction network with analytical domain transformation knowledge[J]. Quantitative Imaging in Medicine and Surgery, 2020, 10(2): 415. doi: 10.21037/qims.2019.12.12
[43] ZHANG Q, HU Z, JIANG C, et al. Artifact removal using a hybrid-domain convolutional neural network for limited-angle computed tomography imaging[J]. Physics in Medicine & Biology, 2020, 65(15): 155010.
[44] LIN W A, LIAO H, PENG C, et al. Dudonet: Dual domain network for CT metal artifact reduction[C]//Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, 2019: 10512-10521.
[45] WANG T, XIA W, HUANG Y, et al. DAN-Net: Dual-domain adaptive-scaling non-local network for CT metal artifact reduction[J]. arXiv Preprint arXiv: 2102.08003, 2021.
[46] WANG T, XIA W, LU Z, et al. IDOL-Net: An interactive dual-domain parallel network for CT metal artifact reduction[J]. arXiv Preprint arXiv: 2104.01405, 2021.
[47] RAN M, XIA W, HUANG Y, et al. Md-recon-net: A parallel dual-domain convolutional neural network for compressed sensing MRI[J]. IEEE Transactions on Radiation and Plasma Medical Sciences, 2020, 5(1): 120−135.
[48] CHEN H, ZHANG Y, CHEN Y, et al. LEARN: Learned experts'assessment-based reconstruction network for sparse-data CT[J]. IEEE Transactions on Medical Imaging, 2018, 37(6): 1333−1347. doi: 10.1109/TMI.2018.2805692
[49] WU D, KIM K, El Fakhri G, et al. Iterative low-dose CT reconstruction with priors trained by artificial neural network[J]. IEEE Transactions on Medical Imaging, 2017, 36(12): 2479−2486. doi: 10.1109/TMI.2017.2753138
[50] KANG E, CHANG W, YOO J, et al. Deep convolutional framelet denosing for low-dose CT via wavelet residual network[J]. IEEE Transactions on Medical Imaging, 2018, 37(6): 1358−1369. doi: 10.1109/TMI.2018.2823756
[51] GAO Y, LIANG Z, MOORE W, et al. A feasibility study of extracting tissue textures from a previous full-dose CT database as prior knowledge for Bayesian reconstruction of current low-dose CT images[J]. IEEE Transactions on Medical Imaging, 2019, 38(8): 1981−1992. doi: 10.1109/TMI.2018.2890788
[52] VENKATAKRISHNAN S V, BOUMAN C A, WOHLBERG B. Plug-and-play priors for model based reconstruction[C]//2013 IEEE Global Conference on Signal and Information Processing. IEEE, 2013: 945-948.
[53] SREEHARI S, VENKATAKRISHNAN S V, WOHLBERG B, et al. Plug-and-play priors for bright field electron tomography and sparse interpolation[J]. IEEE Transactions on Computational Imaging, 2016, 2(4): 408−423.
[54] CASCARANO P, PICCOLOMINI E L, MOROTTI E, et al. Plug-and-play external and internal priors for image restoration[J]. arXiv e-prints, 2021, arXiv: 2102.07510.
[55] ADLER J, OKTEM O. Learned Primal-dual reconstruction[J]. IEEE Transactions on Medical Imaging, 2017: 1322−1332.
[56] XIA W, LU Z, HUANG Y, et al. MAGIC: Manifold and graph integrative convolutional network for low-dose CT reconstruction[J]. IEEE Transactions on Medical Imaging, 2021.
[57] CHEN G, HONG X, DING Q, et al. AirNet: Fused analytical and iterative reconstruction with deep neural network regularization for sparse-data CT[J]. Medical Physics, 2020, 47(7): 2916−2930. doi: 10.1002/mp.14170
[58] GUPTA H, JIN K H, NGUYEN H Q, et al. CNN-based projected gradient descent for consistent CT image reconstruction[J]. IEEE Transactions on Medical Imaging, 2018, 37(6): 1440−1453. doi: 10.1109/TMI.2018.2832656
[59] ZHANG H, LIU B, YU H, et al. MetaInv-net: Meta inversion network for sparse view CT image reconstruction[J]. IEEE Transactions on Medical Imaging, 2020, 40(2): 621−634.
[60] BUADES A, COLL B, MOREL J M. A non-local algorithm for image denoising[C]//2005 IEEE Computer Society Conference on Computer Vision and Pattern Recognition (CVPR'05). IEEE, 2005, 2: 60-65.
[61] CHEN Y, YANG Z, HU Y, et al. Thoracic low-dose CT image processing using an artifact suppressed large-scale nonlocal means[J]. Physics in Medicine & Biology, 2012, 57(9): 2667.
[62] CHEN Y, CHEN W, YIN X, et al. Improving low-dose abdominal CT images by weighted intensity averaging over large-scale neighborhoods[J]. European Journal of Radiology, 2011, 80(2): e42−e49. doi: 10.1016/j.ejrad.2010.07.003
[63] ZHONG J, NING R, CONOVER D. Image denoising based on multiscale singularity detection for cone beam CT breast imaging[J]. IEEE Transactions on Medical Imaging, 2004, 23(6): 696−703. doi: 10.1109/TMI.2004.826944
[64] FERUGLIO P F, VINEGONI C, GROS J, et al. Block matching 3D random noise filtering for absorption optical projection tomography[J]. Physics in Medicine & Biology, 2010, 55(18): 5401.
[65] CHEN Y, SHI L, FENG Q, et al. Artifact suppressed dictionary learning for low-dose CT image processing[J]. IEEE Transactions on Medical Imaging, 2014, 33(12): 2271−2292. doi: 10.1109/TMI.2014.2336860
[66] ZAMYATIN A, KATSEVICH G, KRYLOV R, et al. Adaptive multi-scale total variation minimization filter for low dose CT imaging[C]//SPIE Medical Imaging. International Society for Optics and Photonics, 2014: 903426-903426-7.
[67] MENG B, JIANG H, LIU Z, et al. Curvelet-based bilinear interpolation method for low-dose CT[C]//International Society for Optics and Photonics. Fifth International Conference on Digital Image Processing, 2013: 88783X-88783X-5.
[68] CHEN H, ZHANG Y, ZHANG W H. Low dose CT via convolutional neural network[J]. Biomedical Optics Express, 2017, 8(2): 679−694. DOI: 10.1364/BOE.8.000679.
[69] SHAN H M, ZHANG Y, YANG Q S, et al. 3-D convolutional encoder-decoder network for low-dose CT via transfer learning from a 2-D trained network[J]. IEEE Transactions on Medical Imaging, 2018, 37(6): 1522−1534. DOI: 10.1109/TMI.2018.2832217.
[70] YANG Q S, YAN P K, ZHANG Y B, et al. Low-dose CT image denoising using a generative adversarial network with wasserstein distance and perceptual loss[J]. IEEE Transactions on Medical Imaging, 2018, 36(7): 1348−1357. DOI: 10.1109/TMI.2018.2827462.
[71] ZHU J Y, PARK T, ISOLA P, et al. Unpaired image-to-image translation using cycle-consistent adversarial networks[C]//Proceedings of the IEEE international conference on computer vision. 2017: 2223-2232.
[72] CHEN Y. CT-LSTM: Detection & estimation duplexed system for robust object tracking[C]//Proceedings of the 2nd International Conference on Computer Science and Application Engineering, 2018: 1-7.
[73] BURGER H C, SCHULER C J, HARMELING S. Image denoising: Can plain neural networks compete with BM3D?[C]//2012 IEEE conference on computer vision and pattern recognition. IEEE, 2012: 2392-2399.
[74] CHEN H, ZHANG Y, KALRA M, et al. Low-dose CT with a residual encoder-decoder convolutional neural network[J]. IEEE Transactions on Medical Imaging, 2017, 2(3): 2524−2535. DOI: 10.1109/TMI.2017.2715284.
[75] HEINRICH M P, STILLE M, BUZUG T M. Residual U-net convolutional neural network architecture for low-dose CT denoising[J]. Current Directions in Biomedical Engineering, 2018, 4(1): 297−300. doi: 10.1515/cdbme-2018-0072
[76] WU D F, KIM K, FAKHRI G E, et al. A cascaded convolutional neural network for X-ray low-dose CT image denoising[OL]. https://arxiv.org/abs/1705.04267, 2017.5.
[77] SHAN H, PADOLE A, HOMAYOUNIEH F, et al. Competitive performance of a modularized deep neural network compared to commercial algorithms for low-dose CT image reconstruction[J]. Nature Machine Intelligence, 2019, 1(6): 269−276. doi: 10.1038/s42256-019-0057-9
[78] WOLTERINK J M, LEINER T, VIERGEVER M A, et al. Generative adversarial networks for noise reduction in low-dose CT[J]. IEEE Transactions on Medical Imaging, 2017, 36(12): 2536−2545. DOI: 10.1109/TMI.2017.2708987.
[79] YI X, BABYN P. Sharpness-aware low-dose CT denoising using conditional generative adversarial network[J]. Journal of Digital Imaging, 2018, 31(5): 655−669. doi: 10.1007/s10278-018-0056-0
[80] ISOLA P, ZHU J Y, ZHOU T, et al. Image-to-image translation with conditional adversarial networks[C]//Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition. 2017: 1125-1134.
[81] YANG L, SHANGGUAN H, ZHANG X, et al. High-frequency sensitive generative adversarial network for low-dose CT image denoising[J]. IEEE Access, 2019, 8: 930−943.
[82] YOU C, YANG L, ZHANG Y, et al. Low-dose CT via deep CNN with skip connection and network-in- network[C]//Developments in X-ray Tomography XII. International Society for Optics and Photonics, 2019, 11113: 111131W.
[83] ARJOVSKY M, CHINTALA S, BOTTOU L. Wasserstein gan[J]. arXiv Preprint arXiv: 1701.07875, 2017.
[84] LI X, YE C, YAN Y, et al. Low-dose CT image denoising based on improved WGAN-gp[J]. Journal of New Media, 2019, 1(2): 75. doi: 10.32604/jnm.2019.06259
[85] MAO X, LI Q, XIE H, et al. Least squares generative adversarial networks[C]//Proceedings of the IEEE International Conference on Computer Vision, 2017: 2794-2802.
[86] MIYATO T, KATAOKA T, KOYAMA M, et al. Spectral normalization for generative adversarial networks[J]. arXiv Preprint arXiv: 1802.05957, 2018.
[87] PARK H S, BAEK J, YOU S K, et al. Unpaired image denoising using a generative adversarial network in X-ray CT[J]. IEEE Access, 2019, 7: 110414−110425. doi: 10.1109/ACCESS.2019.2934178
[88] DU W, CHEN H, LIAO P, et al. Visual attention network for low-dose CT[J]. IEEE Signal Processing Letters, 2019, 26(8): 1152−1156. doi: 10.1109/LSP.2019.2922851
[89] RAJEEV R, SAMATH J A, KARTHIKEYAN N K. An intelligent recurrent neural network with long short-term memory (LSTM) BASED batch normalization for medical image denoising[J]. Journal of Medical Systems, 2019, 43(8): 234. doi: 10.1007/s10916-019-1371-9
[90] YANG Q, YAN P, KALRA M K, et al. CT image denoising with perceptive deep neural networks[J]. arXiv Preprint arXiv: 1702.07019, 2017.
[91] YOU C, YANG Q, SHAN H, et al. Structurally-sensitive multi-scale deep neural network for low-dose CT denoising[J]. IEEE Access, 2018, 6: 41839−41855. doi: 10.1109/ACCESS.2018.2858196
[92] GU J, YE J C. AdaIN-based tunable cycleGAN for efficient unsupervised low-dose CT denoising[J]. IEEE Transactions on Computational Imaging, 2021, 7: 73−85. doi: 10.1109/TCI.2021.3050266
[93] KWON T, YE J C. Cycle-free cycleGAN using invertible generator for unsupervised low-dose CT denoising[J]. arXiv Preprint arXiv: 2104.08538, 2021.
[94] LIAO H, LIN W A, ZHOU S K, et al. Adn: Artifact disentanglement network for unsupervised metal artifact reduction[J]. IEEE Transactions on Medical Imaging, 2019, 39(3): 634−643.
[95] KO Y, MOON S, BAEK J, et al. Rigid and non-rigid motion artifact reduction in X-ray CT using attention module[J]. Medical Image Analysis, 2021, 67: 101883. doi: 10.1016/j.media.2020.101883
[96] LI M, HSU W, XIE X, et al. SACNN: Self-attention convolutional neural network for low-dose CT denoising with self-supervised perceptual loss network[J]. IEEE Transactions on Medical Imaging, 2020, 39(7): 2289−2301. doi: 10.1109/TMI.2020.2968472
[97] ZHANG H, PATEL V M. Density-aware single image de-raining using a multi-stream dense network[C]//Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, 2018: 695-704.
[98] HU X, FU C W, ZHU L, et al. Depth-attentional features for single-image rain removal[C]// Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, 2019: 8022-8031.
[99] GUO S, YAN Z, ZHANG K, et al. Toward convolutional blind denoising of real photographs[C]//Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, 2019: 1712-1722.
[100] WANG Y, GONG D, YANG J, et al. An effective two-branch model-based deep network for single image deraining[J]. arXiv Preprint arXiv: 1905.05404, 2019.
[101] WANG Y, ZHANG H, LIU Y, et al. Gradient information guided deraining with a novel network and adversarial training[J]. arXiv Preprint arXiv: 1910.03839, 2019.
[102] MCCOLLOUGH C L, CHEN B, HOLMES D, et al. Low dose CT image and projection data (LDCT-and-Projection-data)[DB/OL]. The Cancer Imaging Archive, 2020. (2020-00-00) [2021-05-20]. https://doi.org/10.7937/9npb-2637.
[103] The American Association of Physicists in Medicine (AAPM). Low dose CT grand challenge[DB/OL]. (2017-00-00) [2021-05-20]. http://www.aapm.org/GrandChallenge/LowDoseCT/.
[104] National biomedical imaging archive[DB/OL]. (2021-00-00) [2021-05-20]. NCIP/national-biomedical-image-archive.
[105] CLARK K, VENDT B, SMITH K, et al. The cancer imaging archive (TCIA) maintaining and operating a public information repository[J]. Journal of Digital Imaging, 2013, 26(6): 1045-1057.
[106] LINGLE W, ERICKSON B, ZULEY M, et al. Radiology data from the cancer genome atlas breast invasive carcinoma [TCGA-BRCA] collection[DB/OL]. The Cancer Imaging Archive, (2016-00-00) [2021-05-20]. http://wiki.cancerimagingarchive.net/.
[107] YI X. Piglet Dataset[DB/OL]. (2019-00-00)[2021-05-20] http://homepage.usask.ca/~xiy525/.
-
期刊类型引用(5)
1. 上官宏,任慧莹,张雄,韩兴隆,桂志国,王燕玲. 基于双编码器双解码器GAN的低剂量CT降噪模型. 计算机应用. 2025(02): 624-632 .  百度学术
百度学术
2. 陈辉艳,王映飞,梁莎,许大幸. 孕妇儿童肺部疾病多模态磁共振扫描应用研究进展. 实用医学影像杂志. 2023(05): 373-375 . 百度学术
3. 朱元正,吕启闻,官瑜,刘且根. 基于深度能量模型的低剂量CT重建. CT理论与应用研究. 2022(06): 709-720 . 本站查看
4. 栗乔新,金科,庞志峰. 一种去除CT图像中同心椭圆伪影的变分模型. CT理论与应用研究. 2022(06): 773-781 . 本站查看
5. 吴凡,刘进,张意,陈阳,陆志凯. 面向CT成像的深度重建算法研究进展. 中国体视学与图像分析. 2022(04): 387-404 . 百度学术
其他类型引用(12)








计量
- 文章访问数: 3116
- HTML全文浏览量: 730
- PDF下载量: 523
- 被引次数: 17


