
Study on the Staging of Primary Lower Extremity Lymphedema Based on Calf Soft-tissue Thickness Measurement by MRI
-
摘要: 目的:探讨基于MRI测量小腿软组织厚度对评估原发性下肢淋巴水肿(PLEL)分期的价值。方法:回顾性收集确诊为PLEL患者90例的临床及MR影像资料,所有患者均行双侧下肢MR检查。采用短时反转恢复序列(STIR)序列测量双侧小腿软组织总厚度(T)、肌骨厚度(M)和皮下软组织厚度(S),分别计算双侧小腿T及S的差值(DT、DS)。参考2020年国际淋巴协会及淋巴外科下肢淋巴水肿的临床分期标准将患者分为Ⅰ、Ⅱ、Ⅲ 期。使用单因素方差分析比较不同临床分期之间的小腿软组织厚度,使用Spearman相关分析小腿软组织厚度与临床分期的相关性,使用ROC曲线确定小腿软组织厚度对临床分期的鉴别效能。结果:3期之间T、S、DT及DS差异均有统计学意义,而M不存在统计学差异;各分期间两两比较,T、S、DT及DS在Ⅰ期与Ⅱ期及Ⅰ期与 Ⅲ 期之间比较均具有统计学差异,而在Ⅱ期与 Ⅲ 期比较无统计学差异。DT(r=0.750)与DS(r=0.772)与临床分期的相关性明显大于T(r=0.669)及S(r=0.734),DS与临床分期相关性最高;M与临床分期无明显相关关系。ROC曲线显示各参数鉴别Ⅰ期与Ⅱ期的AUC值大于鉴别Ⅱ期与 Ⅲ 期的AUC值,所有参数中DS(AUC=0.945)鉴别Ⅰ期与Ⅱ期的曲线下面积(AUC)最高。结论:MRI小腿软组织厚度测量可以作为单侧PLEL临床分期的定量辅助方法,对于单侧PLEL患者,我们推荐DS作为鉴别Ⅰ期与Ⅱ期淋巴水肿的最佳厚度指标。Abstract: Objective: To investigate the value of MRI-based measurement of calf soft-tissue thickness in assessing the clinical staging of primary lower extremity lymphedema (PLEL). Methods: The clinical and MR imaging data of 90 patients diagnosed with PLEL in our hospital were retrospectively collected, and all patients underwent bilateral lower limb MR examinations. Short Time Inversion Recovery (STIR) sequence was used to measure the total soft tissue thickness (T), musculoskeletal thickness (M) and subcutaneous soft tissue thickness (S) of bilateral lower legs, and the difference between T and S of bilateral lower legs (DT, DS) was calculated respectively. Patients were classified into stages Ⅰ, Ⅱ and Ⅲ with reference to the clinical staging criteria of the International Lymphatic Association 2020 and our lymphatic surgery department for lower limb lymphedema, excluding stage 0. One-way ANOVA was used to compare calf soft tissue thickness among different clinical stages, Spearman correlation was used to analyze the correlation between calf soft tissue thickness and clinical stage, and ROC curves were used to evaluate the efficacy of calf soft tissue thickness in discriminating clinical stage. Results: The differences among T, S, DT and DS of the three stages were statistically significant, while there was no statistical difference among M; when comparing two by two in each subperiod, T, S, DT and DS were statistically different between stage Ⅰ and Ⅱ and stage Ⅰ and Ⅲ, while there was no statistical difference between stage II and III. The correlation between DT (r=0.750) and DS (r=0.772) and clinical stage was significantly greater than that between T (r=0.669) and S (r=0.734), with DS showing the highest correlation with clinical stage; there was no significant correlation between M and clinical stage. ROC curves showed that the AUC values for each parameter to identify stage Ⅰ and Ⅱ were greater than those to identify stage Ⅱ and Ⅲ. The AUC value of DS (AUC=0.945) demonstrated the highest area under the curve (AUC) among all parameters to identify stage Ⅰ and stage Ⅱ. Conclusion: MRI soft-tissue thickness measurement of calf can be used as a quantitative adjunct in the clinical staging of unilateral PLEL, and for patients with unilateral PLEL, we recommend DS as the best thickness index to differentiate stage Ⅰ from Ⅱ lymphedema.
-
Keywords:
- MRI /
- lymphedema /
- primary /
- lower extremity /
- stage
-
肺癌是最常见的癌症类型,也是造成癌症相关死亡的主要原因之一[1-2]。肺癌的组织学类型与其成因、进展及临床表现有密切联系[3],非小细胞癌患者占肺癌患者的80%以上,而LUAD和LUSC是最主要的组织学亚型[4]。由于LUAD和LUSC在治疗和预后上存在显著差异,准确鉴别其组织学类型对临床诊疗至关重要[5]。然而,当肺腺癌发生于中央支气管时,其影像学特征与肺鳞癌相似,增加了鉴别难度。目前,病理学检查仍是鉴别NSCLC组织学分型的金标准,但该方法具有侵入性,限制了其广泛应用[6]。
随着深度学习技术的发展,卷积神经网络(CNN)在医学图像分析中展现出巨大潜力,为NSCLC的无创性诊断提供了新思路[7-9]。然而,现有CNN模型在处理LUAD和LUSC影像特征重叠问题时仍存在局限性。因此,本研究提出一种改进的CNN模型ISANET,并基于医院和公共数据集构建计算机辅助诊断模型,旨在为NSCLC的无创性精准预测提供可行性手段。
1. 资料与方法
1.1 一般资料
回顾性分析河北大学附属医院2020年8月至2021年8月的
1000 例肺鳞癌、肺腺癌和正常患者的CT平扫及增强图像及临床信息。纳入标准:①接受胸部CT平扫或增强检查;②病理结果证明肺部原发灶为肺腺癌或肺鳞癌,有且仅有一种原发肿瘤;③胸部CT图像无明显伪影,质量符合实验要求;④≥18岁。排除标准:CT图像质量差,达不到后处理要求。本研究最终纳入90例患者,男64例、女26例,年龄范围40~81岁。根据中华医学会2022年版肺癌临床诊疗指南[2],本组患者包括肺鳞癌29例,肺腺癌31例以及肺部未见明显异常30例,每位患者6~7张CT图像(层厚1.25 mm),共619张图片(肺鳞癌209张、肺腺癌202张和肺部未见明显异常208张)。
图像选取标准:①覆盖肿瘤最大截面;②包含典型影像特征(如分叶、毛刺);③排除伪影严重的层面。
1.2 仪器与方法
为反映图像数据的异构性,采用多台不同的CT扫描仪进行胸部平扫和增强,包括GE New Revolution 256排CT扫描仪、GE DiscoveryTMCT750 HD和联影uCT 520。扫描范围自肺尖至膈底水平,扫描参数如下:管电压120 kVp,管电流150 mA,层厚5 mm,薄层重建1.25 mm,螺距0.984,机架转速0.5 s/周,矩阵512×512,扫描视野50 cm×50 cm。增强扫描时,采用德国Ulrich missouri-XD 2001双管高压注射器经肘静脉注射非离子型碘海醇对比剂(350 mgI/mL,通用电气药业有限公司),剂量为体质量(kg)×0.8 mL/kg,流速3 mL/s,以相同速率跟注生理盐水30 mL。采用对比剂团注跟踪技术自动触发技术,触发阈值150 HU,感兴趣区(region of interest,ROI)放置在升主动脉,延迟5 s扫描动脉期,30 s扫描静脉期。
1.3 图像处理及模型构建
(1)图像预处理。从河北大学附属医院PACS系统获得的619张图片以DICOM格式输出,像素大小为512×512。首先对图像进行预处理,使用3 D slicer对图像进行配准后,使用Python的SimpleIT及Photoshop开源工具包将上述图片像素放缩为256×256,命名为DatasetA。
本研究还使用Kaggle公开数据集中的“Chest CT-Scan Images Dataset”进一步验证ISANET模型的性能,命名为DatasetB。原始数据包含4类(肺鳞癌、肺腺癌、小细胞肺癌、正常)。本研究剔除小细胞肺癌类别,保留肺鳞癌(252张)、肺腺癌(326张)和正常(159张)共737张图像。筛选标准为:①病理确诊;②图像分辨率≥512×512;③无运动伪影。训练集和测试集的比例为6∶4。为使图像识别更准确,本研究使用ImageNet数据集进行预训练[10]。预训练后,ISANET模型能够分辨
1000 种对象类别,学习到大量CT图像的特征。此外,为了防止模型过拟合,本研究对图片做增强处理,将图片按照0.5的概率随机进行水平或垂直翻转,同时随机更改图片亮度、对比度及饱和度(图1)。(2)ISANET模型构建。基于Inception系列CNN模型能够提取丰富图像特征的优势,本研究旨在让该模型聚焦于病理区域,使之能更好的识别出相似度高的非小细胞肺癌CT图像间的差异。因此,本研究基于InceptionV3模型并引入了注意力机制,采用二分类的交叉熵损失函数,提出了一种改进CNN模型,即ISANET模型(相关结构和输入大小详见图2)。
由于InceptionV3最后一个模块的第2个层处经过第1个模块的通道数仅有
1280 ,而此后的两个模块通道数均为2048,会导致重要特性信息被忽略。因此,本研究将通道注意力机制(channel attention mechanism,CAM)的挤压扩张(squeeze and excitation,SE)模块添加于上述位置(图3)。除添加上述通道注意力机制之外,本研究还将空间注意力机制(spatial attention,SA)模块添加于最后一个模块之前,用来降低运算量,加强关键信息的提取,同时增强模型的识别效能,使模型聚焦于特征图中权重更大的区域(图4)。
(3)运行条件与参数。本研究使用1.8.0版本的Pytorch平台进行实验,配备了NVIDIA RTX
3090 GPU,且python的版本为3.8.11。本研究的实验模型基线为Inception的主干部分,即直到卷积层部分结束。本研究在最后一层卷积后添加了通道注意力机制,删除了最后一层池化层,同时在最后一个模块前增加了空间注意力模块。本研究使用Adam优化器,采用Lambda LR作为学习率衰减策略,将学习率设置为1 e-5。在epoch 0-4,学习率保持为1 e-5;在epoch 5-9,学习率变为1 e-5×0.6;在epoch 10-14,学习率变为1 e-5×(0.62)。权重衰减为0.96。单次实验输入图片数为8,迭代次数设置为50。四、统计学分析
本研究使用python 3.8.11软件进行统计学分析。通过记录查准率(precision,PRE),召回率(sensitivity,SEN),并计算出F1分数(F1-score,F1),同时勾画出P-R曲线,评价和比较不同模型的性能。0.5 < P-R曲线下面积(average precision,AP)≤0.7为诊断效能较低,0.7 < AP≤0.9为诊断效能中等,AP > 0.9为诊断效能较高。
$$ \mathrm{A}\mathrm{C}\mathrm{C}=\frac{TP+TN}{TP+FP+TN+FN} \text{,} $$ (1) $$ \mathrm{P}\mathrm{R}\mathrm{E}=\frac{TP}{TP+FP} \text{,} $$ (2) $$ \mathrm{S}\mathrm{E}\mathrm{N}=\frac{TP}{TP+FN} \text{,} $$ (3) $$ \mathrm{F}1=\frac{2TP}{2TP+FP+FN} \text{,} $$ (4) 其中:TP表示正确区分的非小细胞肺癌类别的数量,TN表示错误识别的非小细胞肺癌类别的数量,FP表示正确识别为非目标类别的数量,FN表示错误识别为非目标类别的数量。
2. 结果
本实验通过DatasetA和DatasetB两个数据集,首先探讨ISANET模型的性能,并与包括AlexNet,MobilenetV2,VGG16,InceptionV3和ResNet18在内的5个常用的传统CNN模型进行对比,分析并验证了ISANET模型对于非小细胞肺癌计算机辅助诊断的性能。
2.1 ISANET模型的性能
在DatasetA和DatasetB中,ISANET模型训练集和测试集的准确率和损失曲线如图5所示。结果表明,20 Epoch之后,该模型的准确度趋于稳定。本研究还采用绘制混淆矩阵图的方式,用以评价模型的性能(图6)。如图所示,彩色标记的对角线数值表示模型正确识别为正确目标的图片数,图示结果表明ISANET模型的识别正确率较高。
![]() 图 5 ISANET模型在不同数据集中的准确率和损失曲线Figure 5. Accuracy and loss curves of ISANET on different datasets
图 5 ISANET模型在不同数据集中的准确率和损失曲线Figure 5. Accuracy and loss curves of ISANET on different datasets2.2 ISANET模型与传统CNN模型的性能对比
为了验证ISANET模型的分类器性能,本实验将其与AlexNet,VGG16,InceptionV3,MobilenetV2,ResNet18进行对比实验,并列出上述所有模型DatasetA和DatasetB中D的查准率、召回率、F1值的平均值(表1和表2)。本研究绘制上述所有模型在DatasetA和DatasetB中的P-R曲线(图7)。结果显示,代表ISANET模型的红线位于所有曲线外侧,分别达到了0.996和0.952,这说明ISANET模型准确度最高、模型性能最好。各模型在两数据集中的准确度(即AP值)(表3)。
表 1 不同模型在DatasetA中的查准率、召回率和F1值比较情况Table 1. Comparison of precision, sensitivity, and F1 score of different models in dataset A算法名称 腺癌 鳞癌 未见明显异常 查准率 召回率 F1值 查准率 召回率 F1值 查准率 召回率 F1值 ISANET 0.898 0.925 0.906 0.946 0.914 0.928 0.959 0.985 0.968 AlexNet 0.870 0.852 0.854 0.863 0.895 0.872 0.994 0.999 0.996 VGG16 0.798 0.789 0.761 0.764 0.857 0.771 0.995 0.992 0.994 InceptionV3 0.974 0.807 0.873 0.754 0.941 0.824 0.961 0.954 0.951 MobileNetV2 0.640 0.902 0.733 0.933 0.711 0.799 0.959 0.963 0.953 ResNet18 0.919 0.929 0.919 0.927 0.905 0.911 0.960 0.992 0.969 表 2 不同模型在DatasetB中的查准率、召回率和F1值比较情况Table 2. Comparison of precision, sensitivity, and F1 score of different models in dataset B算法名称 腺癌 鳞癌 未见明显异常 查准率 召回率 F1值 查准率 召回率 F1值 查准率 召回率 F1值 ISANET 0.911 0.824 0.862 0.754 0.882 0.808 0.937 0.942 0.936 AlexNet 0.846 0.740 0.779 0.575 0.816 0.646 0.992 0.895 0.941 VGG16 0.814 0.720 0.717 0.507 0.668 0.531 0.964 0.949 0.952 InceptionV3 0.883 0.835 0.849 0.758 0.824 0.777 0.876 0.938 0.882 MobileNetV2 0.896 0.748 0.805 0.601 0.858 0.670 0.939 0.904 0.910 ResNet18 0.831 0.866 0.842 0.792 0.785 0.788 0.989 0.874 0.926 表 3 各模型在不同数据集中的准确度Table 3. Accuracy of each model in different datasets算法名称 Dataset A Dataset B ISANET 0.996 0.952 AlexNet 0.951 0.854 VGG16 0.939 0.901 InceptionV3 0.980 0.946 MobileNetV2 0.964 0.932 ResNet18 0.992 0.939 2.3 消融实验结果
本研究通过多组消融实验评估ISANET模型的有效性。消融实验中,图片大小均缩放为299×299,两数据集均不进行预训练,其他数据预处理与对比实验均一致,以期实验结果更明显。本研究主要增加了SE模块和SA模块。因此,本研究的3组消融实验包括:①只保留SE模块为A组;②只保留SA模块为B组;③SE模块和SA模块均保留的ISANET模型为C组。此外,将上述3组与D组(未保留SE模块和SA模块的InceptionV3模型)进行对比(表4)。
表 4 消融实验结果Table 4. The results of ablation experiments组别 Dataset A Dataset B A组 0.806 0.745 B组 0.810 0.735 C组 0.854 0.796 D组 0.802 0.721 3. 讨论
非小细胞肺癌的组织学分型目前已显著影响其诊断,并对患者的治疗和预后有着重要的指导意义。尽管组织病理学与分子生物学是分析肿瘤异质性的金标准,但获取组织标本不仅有创、可重复性差,而且由于标本取材的限制,常有不能反映肿瘤组织的整体状况的情况出现,因而开发和研究无创性非小细胞肺癌无创检测工具成为研究热点和难点。本研究采用基于注意力机制的改进CNN模型对肺鳞癌和肺腺癌进行分类,并建立计算机辅助诊断模型,为无创鉴别非小细胞肺癌提供新途径,为这类患者的治疗和预后评估提供了帮助。
目前,深度学习已经在肺癌领域开展了广泛的研究,也取得了良好的效果。在肺癌分类和检测中,已有研究者采用CNN模型对肺癌CT图像进行分类识别并预测,准确率达到71.00%~94.78%[11-20]。除了肺癌CT图像辅助诊断外,CNN模型也被应用于乳腺癌、皮肤癌、脑肿瘤和肾癌等疾病的研究[21-25]。由此可见,CNN在肿瘤医学图像研究领域有着巨大的潜力,为无创性诊断非小细胞肺癌提供了可能。但是,当网络深度超过阈值时,传统的CNN模型将出现梯度消失和性能饱和,增加其计算和存储负荷。因此,Google提出了Inception系列模型,采用不同大小的卷积核,提取不同尺度的图像信息,最后在通道完成信息组合,从而优化图像表征[26]。InceptionV3的开发者将二维卷积核直接拆分成非对称卷积核,ImageNet的分类实验证明该模型性能优于前两代模型,尤其针对多层数的网络,可简化计算量并处理更多的空间特征[27-28]。为使特征图转换更简单自然,同时减少训练参数,除最后一层全连接层保留外,InceptionV3其他的全连接层均使用平均池化层(average pooling,AP)代替。此外,InceptionV3采用批归一化(batch normalization,BN)的方式防止梯度消失,不仅节约了计算资源,而且解放了对内存的巨大需求。
本研究通过建立基于InceptionV3卷积神经网络的ISANET模型,最终Dataset A和Dataset B对于非小细胞肺癌预测准确度分别为99.6%和95.2%。相比于传统的基于CNN模型预测非小细胞肺癌组织学分型,本研究使用的ISANET模型获得了更高的准确度,表明ISANET卷积神经网络可以提供较高的分类置信度。同时,本研究增加了多组消融实验,以最大限度验证SE模块和SA模块的作用。对于Dataset A,A组准确度提高了0.40%,B组则提高了0.80%,即增加SE或SA模块使精确度略微提。这可能是因为Dataset A中的图片清晰度和质量优于Dataset B,使得模型能够更容易地识别出存在于相似度高的两种类别图片中的差异性。而C组中ISANET模型的准确度较Inceptionv3提高了5.20%。对于Dataset B,各组精确度相较于D组明显提升,A组提高了2.30%,B组提高了1.40%,两模块结合的C组提高了7.50%。消融实验结果表明,注意力机制使得ISANET模型能够更好的学习图像的特征,同时证明了添加注意力机制可提升肺鳞癌和肺腺癌分类的准确度。
此外,本研究选择肺部CT平扫和增强图像原因在于临床更易收集,图像分辨率较高,图像预处理较少。而肺部CT增强通过注射碘对比剂可以反映更多的肿瘤异质性[29]。传统的影像组学研究需要人工分割,该过程耗时耗力,与减轻影像医师的日常工作负担的目的相悖[30]。而本研究的图像未预先进行人工分割,但与传统的影像组学模型相比,本研究取得的更高的准确度,节约了时间和人工成本。由于深度学习中的图像特征提取性能非常依赖数据量,若要进一步提高模型准确度以用于临床,最有效的办法是增加海量数据[31]。
本研究存在一定的局限性。首先,尽管模型在现有数据集上表现优异,但样本量较小可能限制其泛化能力。未来将通过交叉验证(如5折交叉验证)和外部独立数据集验证进一步评估模型稳定性。其次,本研究仅着眼于CT平扫和增强图像,未选取其他影像学图像,如MRI和PET/CT等。最后,本研究纳入的数据均为成年人,未将未成年人纳入,未来有必要进一步扩大年龄群的构成。在未来的研究中,我们将邀请其他权威机构继续合作开展多中心研究,进一步增大数据量以期获得更好的模型性能,提升其临床适用性,并尝试纳入MRI和PET/CT图像以期进一步提高模型的可靠性。
综上所述,基于卷积神经网络和注意力机制的深度学习非小细胞肺癌计算机辅助诊断模型ISANET可用于肺鳞癌和肺腺癌的无创预测,为不能耐受手术或者无法进行病理活检的患者制定治疗方案提供更多信息,同时帮助影像医师对非小细胞肺癌进行准确分类,为实现肺癌精准诊断和治疗提供新思路和新方法。
-
![]()
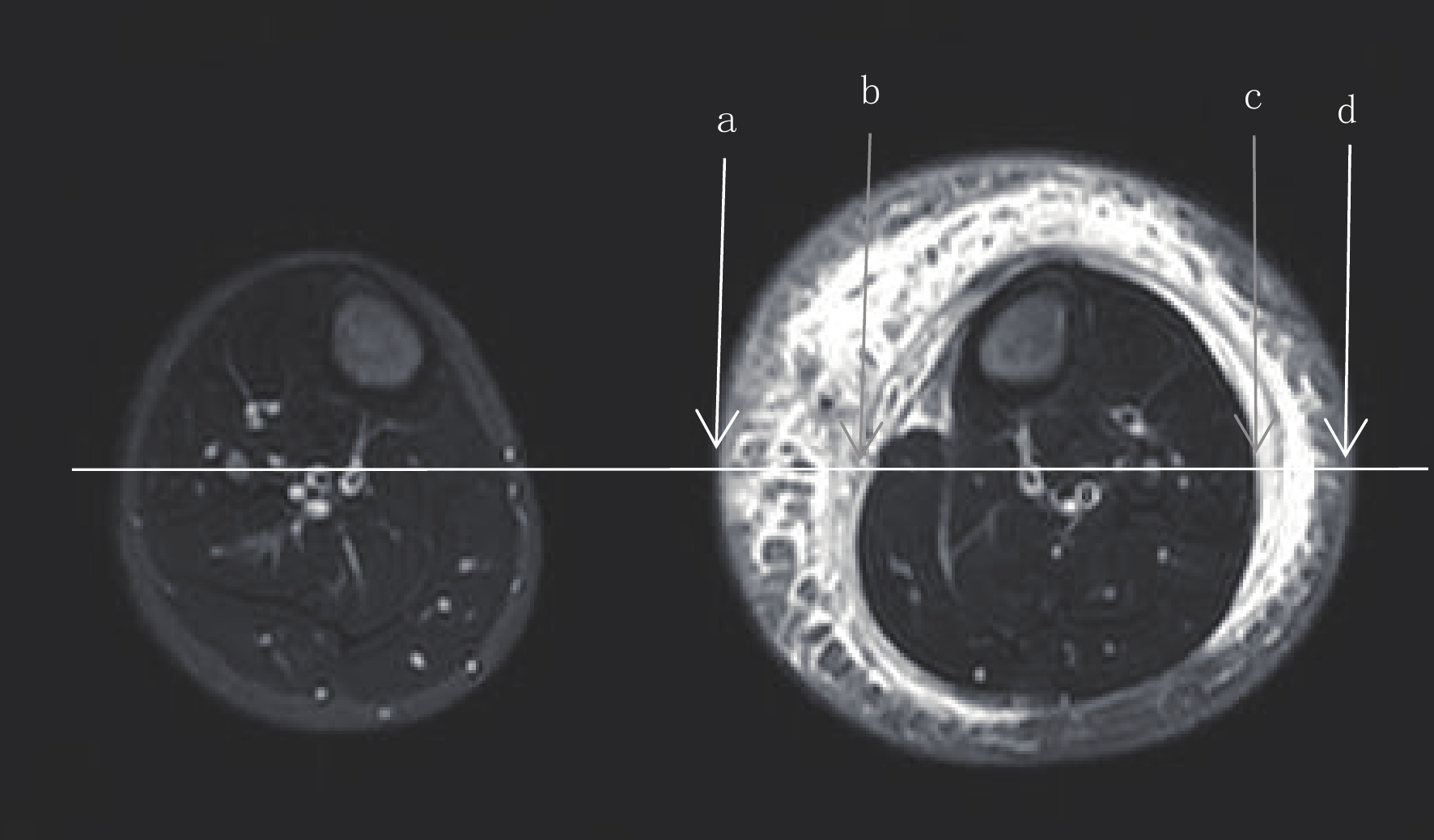
图 1 小腿软组织总厚度(T)、肌肉厚度(M)和皮下组织厚度(S)的测量方法
在小腿轴面STIR图像上,通过小腿上1/3及下1/3层面正中位置(虚线)画一条水平线,测量两层面软组织的厚度。这些线分别与小腿的内侧(a)和外侧(d)皮肤、内侧(b)和外侧(c)浅筋膜相交,(a)与(d)之间的距离表示T的值;(b)与(c)之间的距离表示M的值。S为T减M。健侧小腿的T、M和T的测量方法同患侧小腿。
Figure 1. Total soft tissue thickness (T), muscle thickness (M) and subcutaneous tissue thickness (S) of calf were measured
![]()
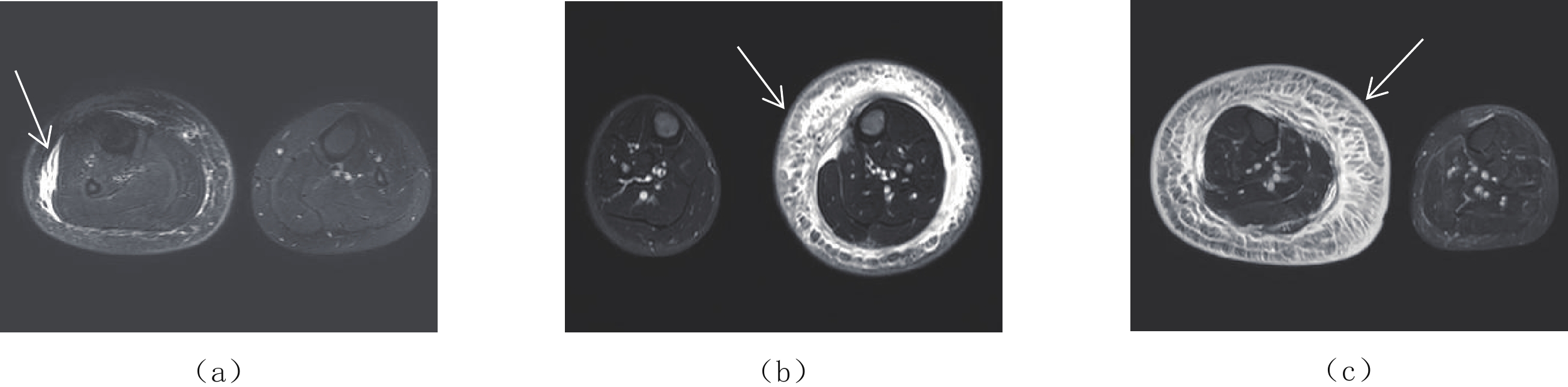
图 2 STIR图像显示不同临床分期皮下软组织厚度的变化
(a)女,14岁,右下肢原发性下肢淋巴水肿1年余(箭头)(Ⅰ期);(b)男,12岁,左下肢原发性下肢淋巴水肿4年(箭头)(Ⅱ期);(c)女,74岁,右下肢原发性下肢淋巴水肿8年(箭头)(Ⅲ 期)。
Figure 2. STIR images show changes in subcutaneous soft tissue thickness at different clinical stages
![]()
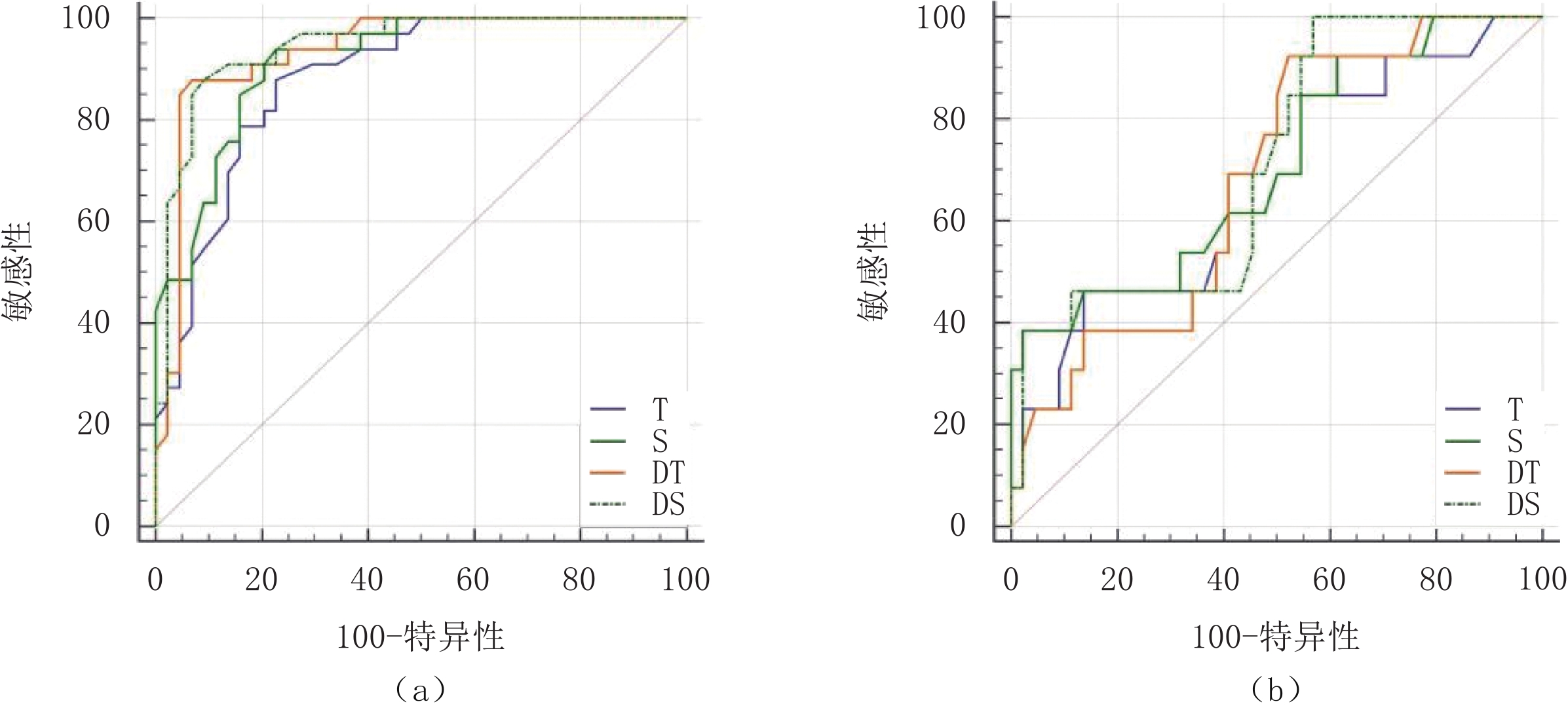
图 3 ROC曲线显示患侧小腿的T、S、DT以及DS进行下肢淋巴水肿分期的效能
(a)Ⅰ期与Ⅱ期比较;(b)Ⅱ期与 Ⅲ期比较。T:总厚度;S:皮下软组织厚度;DT:患侧与健侧总厚度差值;DS:患侧与健侧皮下软组织厚度差值。
Figure 3. ROC curve showed the effectiveness of T, S, DT and DS of the affected leg in staging lymphedema of the lower limb
表 1 2020年国际淋巴协会肢体淋巴水肿临床分期标准
Table 1 Clinical staging criteria for limb lymphedema by the International Lymphatic Society 2020
分期 临床表现 0期 亚临床状态,淋巴系统受损,组织液或成分发生微小变化,但肿胀不明显。可在水肿发生(I~Ⅲ 期)之前存在数月或数年。 Ⅰ期 水肿部位柔软,按压可凹陷,无皮肤纤维化,抬高患肢后肿胀可缓解,又称可逆性水肿。 Ⅱ期 抬高患肢肿胀消退不明显,后期由于皮下脂肪过多和纤维化,水肿可呈非凹陷性。 Ⅲ 期 水肿不可凹陷,病变肢体皮肤改变如脂肪沉积,色素沉着、棘皮病、疣状增生,呈现淋巴象皮肿。  下载: 导出CSV
下载: 导出CSV
表 2 不同分期的原发性下肢淋巴水肿的临床资料
Table 2 Clinical data of patients with primary lymphedema of the lower extremity at different clinical stages
项目 分期临床资料 Ⅰ(n=33) Ⅱ(n=44) Ⅲ(n=13) 年龄/岁* 20.00±19.00 35.50±27.00 29.50±29.00 病程/年* 2.00±9.40 9.00±21.25 9.00±15.00 性别/n(%)a 女 21(63.64) 26(59.09) 7(53.84) 男 12(36.36) 18(40.91) 6(46.16) 注:*-数据采用中位数±四分位间距表示;a-计数资料采用频数(构成比)表示。
下载: 导出CSV
表 3 原发性下肢淋巴水肿患者不同临床分期小腿软组织厚度比较
Table 3 Comparison of calf soft tissue thickness in patients with primary lymphedema of the lower extremity at different clinical stages
参数 分期 统计检验 Ⅰ(n=33) Ⅱ(n=44) Ⅲ(n=13) F/χ P T/cm 10.66±0.91a,b 13.04±1.89a 14.53±2.67b 28.821 <0.001 M/cm 8.08±0.77 8.42±1.30 8.24±0.87 0.944 0.393 S/cm 2.58±0.69a,b 4.62±1.39a 6.29±2.47b 37.970 <0.001 DT/cm 0.95±0.801,a,b 3.50±1.62a 4.94±2.55b 52.2311 <0.001 DS/cm 1.00±0.65a,b 3.18±1.34a 3.40±3.001,b 54.8611 <0.001 注:1-数据采用(中位数±四分位数间距)表示,组间比较采用非参数检验;余数据采用均数±标准差表示,组间
比较采用单因素方差分析。a-Ⅰ期与Ⅱ期比较,P<0.05;b-Ⅰ期与 Ⅲ 期比较,P<0.05。
下载: 导出CSV
表 4 原发性下肢淋巴水肿患者小腿软组织厚度鉴别Ⅰ期及Ⅱ期的ROC曲线分析
Table 4 ROC curve analysis of stage Ⅰ and Ⅱ differentiation of leg soft tissue thickness in patients with primary lower extremity lymphedema
参数 AUC 95% CI P Youden指数 临界值/cm 敏感性/% 特异性/% T 0.882 0.788~0.944 <0.0001 0.6515 11.55 77.27 87.88 S 0.916 0.830~0.967 <0.0001 0.7121 3.55 77.27 93.94 DT 0.935 0.855~0.979 <0.0001 0.8106 1.65 93.18 87.88 DS 0.945 0.869~0.984 <0.0001 0.7879 1.60 90.91 87.88
下载: 导出CSV
表 5 原发性下肢淋巴水肿患者小腿软组织厚度鉴别Ⅱ期及 Ⅲ 期的ROC曲线分析
Table 5 ROC curve analysis of leg soft tissue thickness in stage Ⅱ and Ⅲ differentiation of primary lymphedema of lower extremities
参数 AUC 95% CI P Youden指数 临界值/cm 敏感性/% 特异性/% T 0.667 0.530~0.786 0.063 0.325 14.90 46.15 86.36 S 0.705 0.570~0.819 0.018 0.362 7.35 38.46 97.73 DT 0.685 0.549~0.802 0.020 0.400 2.95 92.31 47.73 DS 0.717 0.582~0.828 0.007 0.432 2.60 100.00 43.18
下载: 导出CSV
-
[1] VIGNES S. Lymphedema: From diagnosis to treatment[J]. La Revue de Medecine Interne, 2017, 38(2): 97−105. doi: 10.1016/j.revmed.2016.07.005
[2] 王鹤玮, 贾杰. 乳腺癌术后上肢淋巴水肿的检查与评估研究进展[J]. 中国康复理论与实践, 2017,23(9): 1001−1006. doi: 10.3969/j.issn.1006-9771.2017.09.003 WANG H W, JIA J. Advance in examination and evaluation of upper limb lymphedema after breast cancer surgery (review)[J]. Chinese Journal of Rehabilitation Theory and Practice, 2017, 23(9): 1001−1006. (in Chinese). doi: 10.3969/j.issn.1006-9771.2017.09.003
[3] TASSENOY A, de STRIJCKER D, ADRIAENSSENS N, et al. The use of noninvasive imaging techniques in the assessment of secondary lymphedema tissue changes as part of staging lymphedema[J]. Lymphatic Research and Biology, 2016, 14(3): 127−133. doi: 10.1089/lrb.2016.0011
[4] LIU N F, YAN Z X, WU X F, et al. Magnetic resonance lymphography demonstrates spontaneous lymphatic disruption and regeneration in obstructive lymphedema[J]. Lymphology, 2013, 46(2): 56−63.
[5] Executive Committee of the International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2020 Consensus Document of the International Society of Lymphology[J]. Lymphology, 2020, 53(1): 3−19.
[6] BRUNELLE C L, TAGHIAN A G. Lymphoedema screening: Setting the standard[J]. British Journal of Cancer, 2020, 123(1): 1−2. doi: 10.1038/s41416-020-0848-0
[7] CELLINA M, MARTINENGHI C, PANZERI M, et al. Noncontrast MR lymphography in secondary lower limb lymphedema[J]. Journal of Magnetic Resonance Imaging, 2021, 53(2): 458−466. doi: 10.1002/jmri.27328
[8] 王丽, 李苏芹, 华小兰, 等. 妇科恶性肿瘤术后下肢淋巴水肿MRI分期研究[J]. 实用放射学杂志, 2017,33(3): 343−348. doi: 10.3969/j.issn.1002-1671.2017.03.006 WANG L, LI S Q, HUA X L, et al. Cross-sectional areas of calf soft tissue measured with MRI as a new method for staging gynecologic oncology-related extremity lymphedema[J]. Journal of Practical Radiology, 2017, 33(3): 343−348. (in Chinese). doi: 10.3969/j.issn.1002-1671.2017.03.006
[9] ARRIVÉ L, DERHY S, DAHAN B, et al. Primary lower limb lymphoedema: Classification with non-contrast MR lymphography[J]. European Radiology, 2018, 28(1): 291−300. doi: 10.1007/s00330-017-4948-z
[10] KIM G, SMITH M P, DONOHOE K J, et al. MRI staging of upper extremity secondary lymphedema: Correlation with clinical measurements[J]. European Radiology, 2020, 30(8): 4686−4694. doi: 10.1007/s00330-020-06790-0
[11] GRADA A A, PHILLIPS T J. Lymphedema: Pathophysiology and clinical manifestations[J]. Journal of the American Academy of Dermatology, 2017, 77(6): 1009−1020. doi: 10.1016/j.jaad.2017.03.022
[12] DAYAN J H, WISER I, VERMA R, et al. Regional patterns of fluid and fat accumulation in patients with lower extremity lymphedema using magnetic resonance angiography[J]. Plastic and Reconstructive Surgery, 2020, 145(2): 555−563. doi: 10.1097/PRS.0000000000006520
[13] ZARRAD M, DUFLOS C, MARIN G, et al. Skin layer thickness and shear wave elastography changes induced by intensive decongestive treatment of lower limb lymphedema[J]. Lymphatic Research and Biology, 2022, 20(1): 17−25.
[14] LU Q, LI Y, CHEN T W, et al. Validity of soft-tissue thickness of calf measured using MRI for assessing unilateral lower extremity lymphoedema secondary to cervical and endometrial cancer treatments[J]. Clinical Radiology, 2014, 69(12): 1287−1294. doi: 10.1016/j.crad.2014.08.011
[15] TASSENOY A, de MEY J, de RIDDER F, et al. Postmastectomy lymphoedema: Different patterns of fluid distribution visualised by ultrasound imaging compared with magnetic resonance imaging[J]. Physiotherapy, 2011, 97: 234−243. doi: 10.1016/j.physio.2010.08.003
-
期刊类型引用(12)
1. 曹翼治,于洪涛,王伟,王锋,陶智慧. 肺动脉栓塞中双源CT大螺距联合低浓度造影剂CTPA的参数设置优化研究. 航空航天医学杂志. 2025(03): 257-259 .  百度学术
百度学术
2. 于洪涛,王锋,王伟,曹翼治,李逸人,杨桂伦. 双源CT Flash扫描模式联合低剂量肺动脉CTA在肺栓塞诊断中的应用价值. 医学影像学杂志. 2025(02): 52-54+59 . 百度学术
3. 王永胜,杨磊清,杨怡帆,裴青霞,王晨思,鲁梦云,何俊林,陈文静,田香宝. 不同触发阈值对肺动脉CTA图像质量影响的研究. CT理论与应用研究. 2024(02): 175-181 . 本站查看
4. 董佳勇,连三平. 64排螺旋CT低剂量造影剂肺动脉CTA成像的应用效果观察. 中国卫生标准管理. 2024(05): 107-110 . 百度学术
5. 王晨思,洪瑶,方慧敏,丁雪璐,杨怡帆,田香宝,陈文静,王永胜. 基于自动管电流调制技术下不同螺距对颈部CTA辐射剂量及图像质量影响的研究. CT理论与应用研究. 2024(03): 309-315 . 本站查看
6. 裴锦奎,刘豪,张进慧,朱柳红,周建军. 肺动脉CTA联合腹盆部增强CT的一站式能谱扫描在妇科肿瘤患者术前评估中的价值. 中国临床医学. 2024(05): 795-803 . 百度学术
7. 薛莉薇,许念洁,刘元芬. 三期双流法在CT肺动脉造影的可行性和安全性评价. 福建医科大学学报. 2024(04): 256-262 . 百度学术
8. 熊赛赛,李树要,吉明山,冶冰洁,于娜,赵伟伟. 老年放化疗患者胸部增强CT造影效果与低对比剂注射流速相关研究. 影像研究与医学应用. 2024(21): 50-53 . 百度学术
9. 王永胜,张鹏宇,李方中,王正华,鲁梦云,陈蕾,何俊林,陈文静. 不同管电压对头颈部CTA图像质量影响的研究. CT理论与应用研究. 2022(05): 631-638 . 本站查看
10. 问进. 低浓度对比剂依据体表面积个性化注射模式在单心动周期成像冠脉CTA中的作用. 影像研究与医学应用. 2022(19): 152-154 . 百度学术
11. 胡灯元,杜文杰. 低剂量对比剂肺动脉CTA成像检查肺动脉栓塞的临床价值分析. 医学影像学杂志. 2022(11): 2007-2009 . 百度学术
12. 黄嘉成,杨凌乔,车铭,邹晓凤. 64层螺旋CT对使用正常剂量与低剂量造影剂肺动脉CTA的效果分析. 影像研究与医学应用. 2022(21): 82-84 . 百度学术
其他类型引用(0)











计量
- 文章访问数: 321
- HTML全文浏览量: 140
- PDF下载量: 20
- 被引次数: 12


